

Abstract
The aims of this study were to review the clinicopathological characteristics of diminutive (≤ 5 mm) and small polyps (> 5 mm but < 10 mm) and to evaluate the risk factors of advanced adenoma for polyps of diameter < 10 mm in the colon. The medical records of 4,711 patients who underwent first colonoscopy at outpatient clinics or health promotion center were reviewed retrospectively. We analyzed the presence and risk factors of advanced adenoma, which was defined as a villous or tubulovillous polyp, high-grade dysplasia or intramucosal carcinoma histologically. Total 5,058 polyps were detected in the 4,711 patients, and 93.0% (4,704/5,058) polyps were < 10 mm in size. Among them, advanced adenoma was noted in 0.6% (28/4,704) with a villous component in 19, high-grade dysplasia in 3, and adenocarcinoma in 6. Advanced and non-advanced adenomas differed significantly in age group, gender, and polyp size. Multivariate analysis showed that an advanced age (> 65 years), a male gender, and a polyp size of > 5 mm were risk factors of advanced adenoma. The incidence of advanced adenoma in polyps of < 10 mm was 0.6%. Polyp size, male gender, and age of > 65 years are independent risk factors of advanced adenoma.
Keywords: Diminutive and Small, Advanced Adenoma, Colorectal Polyp
Graphical Abstract
INTRODUCTION
Worldwide, colorectal cancer is the fourth most common cancer in men and the third most common cancer in women. Each year more than 1 million new diagnoses are made and more than 500,000 die of the disease (1). Similarly, in Korea, colorectal cancer is a major cause of morbidity and mortality. The majority of colorectal cancers arise from preexisting adenomatous polyps (2), which can be classified as diminutive (≤ 5 mm), small (6-9 mm), sub-centimeter (< 10 mm), or large (≥ 10 mm) (3,4).
Hassan et al. (3) in an analysis of four studies, which included 20,562 screening subjects, found that advanced adenoma was detected in 1,155 (5.6%), and that diminutive, small, and large polyps accounted for 4.6%, 7.9%, and 87.5% respectively. In another study, advanced adenoma among small polyps was found to be relatively common (rates ranged from 6.6% to 12.5%), which was primarily attributed to the presence of villous features (5,6).
The management strategy for diminutive and small colorectal polyps has not been defined. However, a change in the paradigm of the western colonoscopic management of diminutive colorectal polyps was suggested recently. This is new strategy, which is referred to as the 'predict-resect-and-discard' policy, involves dispensing with postpolypectomy pathological examinations to improve the cost-effectiveness of screening colonoscopy (7,8).
According to the widely accepted adenoma-carcinoma sequence, which can explain > 80% of colorectal cancers development, colorectal cancer screening of average-risk adults is based on adenoma detection, especially the detection of advanced adenoma. Colonoscopy enables detection and removal of precancerous lesion, and may effectively prevent up to 90% of colorectal cancers (9,10).
Recently, due to the increased use of colonoscopy for health promotion, the detection rates of diminutive and small polyps are showing rapid increases. Previous studies on colorectal polyp in Korea have almost all focused on large polyps (≥ 10 mm). In the present study, we investigated the clinicopathological characteristics of diminutive and small polyps and sought to identify the risk factors of advanced adenoma.
MATERIALS AND METHODS
The medical records of 4,711 patients who underwent first colonoscopy at our hospital from January 2009 to December 2012 were reviewed retrospectively. The exclusion criteria applied were: 1) a diagnosis of colorectal cancer or a history of colectomy, 2) inflammatory bowel disease and subepithelial lesion or hereditary polyposis syndrome, 3) lack on information regarding polyp size and morphology of histologic findings, 4) a polyp of ≥ 10 mm, 5) previous colonoscopy for polypectomy or as a follow-up study. However, cases with confirmed malignancy after biopsy or endoscopic mucosal resection were included in the analysis.
Of the 2,525 patients, 4,704 polyps with diameter < 10 mm were detected. Polyps were classified into diminutive polyp (≤ 5 mm) or small polyp (> 5 mm and < 10 mm). Anatomic locations where classified as cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum, and they were reclassified into right side and left side colon polyp. Right-sided polyps were defined as proximal to and including the splenic flexure up to cecum, and left-sided polyps were defined as distal to the splenic flexure. Patient characteristics, and polyp sizes, gross morphologies, locations, and histologies were evaluated. Gross morphologies were classified as pedunculated (Ip), subpedunculated (Isp), sessile (Is), or flat polyp (IIa), and histologies as tubular adenoma, tubulovillous adenoma, villous adenoma, intramucosal adenocarcinoma, hyperplastic, lymphoid hyperplasia, and chronic inflammation. We also reclassified colorectal polyps histologically as neoplastic (adenomatous) or non-neoplastic (hyperplastic). Advanced adenoma was defined as villous or tubulovillous with or without high-grade dysplasia or intramucosal carcinoma that is determined histologically, a size of ≥ 10 mm, or > 3 polyps per patient (11,12,13).
We calculated the proportion of advanced adenomas among small and diminutive polyps and evaluate the risk factors of advanced adenoma in polyps of < 10 mm by comparing patient's clinical characteristics advanced and non-advanced adenoma.
SPSS version 15.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for the analysis and P values of < 0.05 were considered statistically significant. Results are expressed as means ± SDs (continuous variables) or as percentages (categorical data). Differences in clinical characteristics were explored using the χ2 test (categorical variables) or by analysis of variance (quantitative variables). Binary logistic regression analysis was used to identify risk factors of advanced adenoma.
Ethics statement
The study protocol was approved by the institutional review board of Yeungnam University Hospital (IRB No. YUH-13-O37). Informed consent was exempted by the board.
RESULTS
Baseline characteristics of patients and polyps
In the study population, the male to female ratio was 1:0.65 and mean age was 56.2 ± 13.0 years. Of the 4,711 patients, 2,525 (53.6%) patients were found to have polyps and total 5,058 polyps were detected. Of the 5,058 polyps, 93% (4,704) were < 10 mm, 2,230 polyps (47.4%) were right-sided and had mean size of 4 ± 2 mm. A cold biopsy technique was used for 82.2% of the polyps and the others were removed by standard polypectomy. Of the 4,704 polyps sized < 10 mm, adenomatous (neoplastic) polyps were detected in 58.7% (2,761/4,704) (Table 1). Of the 2,761 cases, 1,858 were diminutive (67.3%) and 903 were small (32.7%). Regarding, non-neoplastic and other histologies, 16.0% (754/4,704) were hyperplastic polyps, 24.0% (1,129/4,704) were attributed to non-specific inflammation, and 1.3% (60/4,704) to lymphoid hyperplasia. Among the 4,704 polyps sized < 10 mm, advanced adenomas were noted in 0.6% (28/4,704). Among them, 19 had a villous component, 3 were of high-grade dysplasia, and 6 were of adenocarcinoma (Table 2). Mean size of advanced adenomas was 6 ± 2 mm, the sessile type was the most common and were most commonly detected in rectum (Table 3).
Table 1. Baseline characteristics.
| Variables | Findings |
|---|---|
| Age, yr | 56.2 ± 13.0 |
| Gender (male: female) | 1:0.65 |
| Detection rate of polyps, No. with polyp/No. of examined | 2,525/4,711 (53.6%) |
| Mean number of polyps per patient | 2.0 (5,058/2,525) |
| Rate of sub-centimeter (below 10 mm) polyps | 4,704/5,058 (93.0%) |
| Rate of sub-centimeter (below 10 mm) adenomas | 2,761/4,704 (58.7%) |
Table 2. Analysis of the 4,704 polyp(s) with a diameter of less than 10 mm.
| Variables | Findings |
|---|---|
| Size, mm | 4 ± 2 |
| Distribution | |
| Right | 2,230 (47.4%) |
| Left | 2,474 (52.6%) |
| Histology | |
| Tubular adenoma | 2,733 (58.1%) |
| Tubulovillous adenoma | 18 (0.4%) |
| Villous adenoma | 1 (0.02%) |
| Serrated adenoma | 7 (0.1%) |
| High grade dysplasia | 3 (0.01%) |
| Adenocarcinoma | 6 (0.1%) |
| Hyperplastic polyp | 754 (16.0%) |
| Chronic inflammation | 1,122 (23.9%) |
| Lymphoid hyperplasia | 60 (1.3%) |
| Advanced adenoma* | 28 (0.6%) |
*Villous or tubulovillous polyps and/or high-grade dysplasia or intramucosal carcinoma.
Table 3. Characteristics of advanced and non-advanced adenoma.
| Variables | Advanced group | Non-advanced group | P value |
|---|---|---|---|
| Age | 65.4 ± 9.6 | 61.2 ± 11.1 | 0.030 |
| Gender | |||
| M:F ratio | 1:0.87 | 1:0.40 | 0.038 |
| Size | |||
| Diminutive | 6 (21.4%) | 1,852 (67.8%) | < 0.001 |
| Small | 22 (78.6%) | 881 (32.2%) | |
| Mean size, cm | 0.6 ± 0.2 | 0.4 ± 0.2 | 0.005 |
| Shape | |||
| Is | 12 (42.9%) | 1,530 (56.0) | 0.142 |
| IIa | 8 (28.6%) | 780 (28.5) | |
| Isp | 6 (21.4%) | 390 (14.3) | |
| Ip | 2 (7.1%) | 33 (1.2) | |
| Distribution | |||
| Right | 14 (50%) | 1,522 (55.7%) | 0.547 |
| Left | 14 (50%) | 1,211 (44.3%) |
M, male; F, female; Ip, pedunculated polyp; Isp, subpedunculated polyp; Is, sessile polyp; IIa, flat polyp.
Advanced vs. non-advanced adenoma
Patients with advanced adenoma were significantly older than non-advanced adenoma group (65.4 ± 9.6 vs. 61.2 ± 11.1, P = 0.03). Furthermore, the proportion of males was significantly higher in the advanced adenoma group (15:13 vs. 71.4:28.6, P = 0.038). Among 28 advanced polyps sized < 10 mm, 6 were diminutive polyps and 22 were small polyps. Advanced adenomas were larger than non-advanced adenoma (6 ± 2 mm vs. 4 ± 2 mm, P = 0.005). Advanced adenomas were detected in the rectum (28.6%), A-colon (25%), and T-colon (14.3%). However, the distribution of advanced adenomas of < 10 mm was equal for right and left sides (right:left = 14:14). The shape of advanced adenoma consist of Is (42.9%), IIa (28.6%), Isp (21.4%) and Ip (7.1%). There is no meaningful statistical difference in shape and distribution between advanced and non-advanced adenoma (Table 3). Histologically, tubulovillous adenoma was noted in 18 (64%), villous adenoma in 1 (4%), high-grade dysplasia in 3 (11%), and adenocarcinoma in 6 (21%). All of the high-grade dysplasias were detected in men and sessile type. Adenocarcinoma was also noted in 6 patients, and was more common in men (4 cases vs. 2 cases, P = 0.024). Among the carcinomas, three involved diminutive polyps. Adenocarcinoma rates were similar for right and left colons.
Risk factors of advanced adenoma
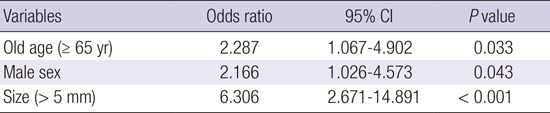
For small and diminutive polyps, age, gender, and polyp size were significantly different for advanced and non-advanced adenoma. Patients older than 65 had more advanced adenoma (P = 0.033, OR 2.287), men had a higher risk of advanced adenoma than women (P = 0.043, OR 2.166), and small polyps had a 6-fold higher risk of advanced adenoma than diminutive polyps (P < 0.001, OR 6.306). Multivariate analysis showed that an age of > 65, a male gender, and a polyp size > 5 mm were risk factors of advanced adenoma for polyps < 10 mm (Table 4).
Table 4. Multivariable analysis for the risk factors of advanced adenoma among small and diminutive polyps.
| Variables | Odds ratio | 95% CI | P value |
|---|---|---|---|
| Old age (≥ 65 yr) | 2.287 | 1.067-4.902 | 0.033 |
| Male sex | 2.166 | 1.026-4.573 | 0.043 |
| Size (> 5 mm) | 6.306 | 2.671-14.891 | < 0.001 |
CI, confidence interval.
DISCUSSION
Colonoscopy studies have reported that colorectal adenoma could be detected 40% in those aged > 50 years (14,15). In the present study, polyps of < 10 mm constituted the majority (93%) detected by colonoscopy. Recently, a 'resect and discard' strategy was recommended for small polyps based on considerations of cost effectiveness. Before such strategy is adopted, we need to be aware of the clinical significance of colorectal polyps of < 10 mm. However, few Korean studies on diminutive or small polyps have been reported during the last ten years. Accordingly, the aim of the present study was to evaluate the clinical significances of diminutive and small polyps by analyzing clinical characteristics and by determining the frequency of advanced adenoma.
In the present study, the overall percentage of polyps of < 10 mm was 93.0% (4,704/5,058) and of these 58.7% (2,761/4,704) were adenomatous (1,858 diminutive and 903 small), which concur percentages obtained in the West. Furthermore, the frequency of advanced adenoma determined in the present study was also similar to those determined by previous western studies (Tables 5 and 6) (5,16,17).
Table 5. Histologic results of advanced adenomas according to polyp size.
| Variables | No. (%) | |
|---|---|---|
| Diminutive adenomas | Small adenomas | |
| Tubulovillous adenomas | 4 (66.7) | 15 (68.2) |
| Villous adenomas | 0 (0.0) | 1 (4.5) |
| High-grade dysplasia | 0 (0.0) | 2 (9.1) |
| Intramucosal adenocarcinoma | 2 (33.3) | 4 (18.2) |
| Total | 6 (100.0) | 22 (100.0) |
Table 6. Prevalence of advanced adenoma by polyp size.
| Studies | No. (%) of advanced adenoma by size | ||||
|---|---|---|---|---|---|
| ≤ 5 mm | 6-9 mm | < 10 mm | ≥ 10 mm | Total | |
| Pickhardt et al. (16) (n = 1,233) | 1 (0.08) | 6 (0.5) | 7 (0.6) | 48 (3.9) | 55 (4.5) |
| Kim et al. (17) (n = 3,163) | 3 (0.09) | 11 (0.3) | 14 (0.4) | 103 (3.3) | 139 (6.4) |
| Lieberman et al. (5) (n = 13,992) | 45 (0.3) | 62 (0.4) | 107 (0.8) | 737 (5.3) | 844 (6.0) |
| The present study (n = 5,058) | 6 (0.1) | 22 (0.4) | 28 (0.6) | 254 (5.0) | 282 (5.6) |
Colorectal cancer (CRC) screening aims to reduce CRC mortality by identifying and subsequently removing advanced adenoma. However, the frequency of advanced adenoma are rare in diminutive or small polyps, and therefore, the limited clinical significance of polyps of < 10 mm supports the recently proposed 'resect and discard' strategy (7,18).
Previously, many authors have suggested that the risk factors of advanced adenoma are strongly associated with polyp size, location (19,20,21). And current reports have identified a male gender, old age, obesity, and cigarette smoking as independent risk factors of advanced adenoma (19,20,21). In spite of efforts to identify the risk factors of adenomatous colonic polyps, study is lacking regarding the risk factors of advanced adenoma for polyps of < 10 mm. In the present study, polyp size, male sex, and an age of > 65 were found to be independent risk factors of advanced adenoma. An advanced age has been previously associated with advanced histology amongst polyps of < 10 mm (5,6,22).
The American Society for Gastrointestinal Endoscopy (ASGE) has recommended two strategies, namely, a 'predict-resect-and-discard' strategy without pathological assessment for non-rectosigmoid lesions of < 5 mm and a 'predict-and-do-not-resect' strategy for rectosigmoid diminutive polyps predicted to be hyperplastic by electronic chromoendoscopy (EC) (18). These strategies offer cost savings with respect to polypectomy and postpolypectomy pathological examinations in a substantial proportion of cases. However, EC-based strategies require careful reassessment of current postpolypectomy surveillance guidelines (23).
In the present study, the percentage of hyperplastic polyp in the rectosigmoid colon was 11.0% (555/5,058), and most (98.2%) were < 5 mm in diameter. Generally, most hyperplastic polyps are small, are found on the left side, and are not associated with an increased risk of colon cancer. Therefore, routine comprehensive resection for diminutive or small hyperplastic polyps of the rectosigmoid colon could be unnecessary. However, in Korea, a 'predict-resect-and-discard' strategy could not be adopted because electronic chromoendoscopy data is limited and the technique is not commonly available.
According to current western trends, uniform resection of diminutive polyp is not recommended for reasons of cost effectiveness in countries with high medical costs. Furthermore, the complete resection rate of subcentimetric lesions by forcep biopsy is not satisfactory and removal might have no clinical meaning. Nevertheless, regardless of size, advanced polyps, especially advanced adenoma, should be removed completely.
This study was undertaken to determine the proportion of advanced adenomas among diminutive and small polyps and to identify the risk factors of advanced adenoma. In the present study, when polyp size was restricted to < 10 mm, the rate of advanced adenoma was 0.6%, and for diminutive polyps, the rate of advanced adenoma was only 0.1%. Although two cases of intramucosal adenocarcinoma were found among diminutive polyps, the clinical significance of diminutive polyps is extremely low when we consider the incidence. However, in countries like Korea, where the costs of colonoscopy and polyp resection are relatively low, efforts to detect small and diminutive polyps can be helpful. Furthermore, in view of relatively high missing rate of polyp, incomplete resection rates and relatively low medical costs, in Korea, meticulous efforts are needed to find and remove polyps of < 10 mm completely, especially in older men with a polyp of > 5 mm. We suggest more study be undertaken to determine the efficacy of resecting diminutive polyps.
The present study is intrinsically limited by its retrospective nature. In addition, the accuracies of polyp sizes are questionable because they were determined using endoscopic findings. Furthermore, the achievement of complete resection was indeterminate in many cases, because resection margins were not detailed in pathologic reports. However, the present study involved a larger cohort than previous studies, and efforts were made to minimize errors having an endoscopist review endoscopic findings.
Summarizing, in our center, the prevalence of polyps of < 10 mm was 93%, and the advanced adenoma rate for these polyps was 0.6%. Polyp size ≥ 5 mm, a male gender, and an age of > 65 years are identified risk factors of advanced adenoma for polyps of < 10 mm in this study. Although the risk is low, meticulous attention is required to avoid missing and to achieve complete removal of advanced adenoma among polyps smaller than 10 mm, especially in the patients with these three risk factors.
Footnotes
Funding: This study was supported by a Yeungnam University Research Grant (2015).
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Study design: Jeong YH, Kim KO. Acquisition of data: Jeong YH, Kim KO, Park CS, Kim SB, Lee SH, Jang BI. Statistical analysis and interpretation of data: Park CS, Kim SB, Lee SH. Writing the draft: Jeong YH. Revision of manuscript: Kim KO. Approval of the final version: all authors.
References
- 1.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 2.Nouraie M, Hosseinkhah F, Brim H, Zamanifekri B, Smoot DT, Ashktorab H. Clinicopathological features of colon polyps from African-Americans. Dig Dis Sci. 2010;55:1442–1449. doi: 10.1007/s10620-010-1133-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hassan C, Pickhardt PJ, Kim DH, Di Giulio E, Zullo A, Laghi A, Repici A, Iafrate F, Osborn J, Annibale B. Systematic review: distribution of advanced neoplasia according to polyp size at screening colonoscopy. Aliment Pharmacol Ther. 2010;31:210–217. doi: 10.1111/j.1365-2036.2009.04160.x. [DOI] [PubMed] [Google Scholar]
- 4.Lee S, Kim SH, Lee DY, Sun JH, Park JS, Park JS, Yang DH, Na HY, Kim KT. Clinicopathologic features and clinical significance of small and diminutive colorectal polyps. J Korean Soc Coloproctol. 2005;21:6–12. [Google Scholar]
- 5.Lieberman D, Moravec M, Holub J, Michaels L, Eisen G. Polyp size and advanced histology in patients undergoing colonoscopy screening: implications for CT colonography. Gastroenterology. 2008;135:1100–1105. doi: 10.1053/j.gastro.2008.06.083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Unal H, Selcuk H, Gokcan H, Tore E, Sar A, Korkmaz M, Bilezikci B, Demirhan B, Gur G, Yilmaz U. Malignancy risk of small polyps and related factors. Dig Dis Sci. 2007;52:2796–2799. doi: 10.1007/s10620-007-9782-8. [DOI] [PubMed] [Google Scholar]
- 7.Radaelli F. The resect-and-discard strategy for management of small and diminutive colonic polyps. Gastroenterol Hepatol (N Y) 2013;9:305–308. [PMC free article] [PubMed] [Google Scholar]
- 8.Kang YK. Diminutive and small colorectal polyps: the pathologist's perspective. Clin Endosc. 2014;47:404–408. doi: 10.5946/ce.2014.47.5.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Winawer SJ, Zauber AG, O'Brien MJ, Ho MN, Gottlieb L, Sternberg SS, Waye JD, Bond J, Schapiro M, Stewart ET, et al. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study Workgroup. N Engl J Med. 1993;328:901–906. doi: 10.1056/NEJM199304013281301. [DOI] [PubMed] [Google Scholar]
- 10.Winawer SJ, Zauber AG, Ho MN, O'Brien MJ, Gottlieb LS, Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. doi: 10.1056/NEJM199312303292701. [DOI] [PubMed] [Google Scholar]
- 11.Atkin WS, Morson BC, Cuzick J. Long-term risk of colorectal cancer after excision of rectosigmoid adenomas. N Engl J Med. 1992;326:658–662. doi: 10.1056/NEJM199203053261002. [DOI] [PubMed] [Google Scholar]
- 12.Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251–2270. doi: 10.1002/cncr.2820360944. [DOI] [PubMed] [Google Scholar]
- 13.Winawer SJ, Zauber AG. The advanced adenoma as the primary target of screening. Gastrointest Endosc Clin N Am. 2002;12:1–9. doi: 10.1016/s1052-5157(03)00053-9. [v.] [DOI] [PubMed] [Google Scholar]
- 14.Rickert RR, Auerbach O, Garfinkel L, Hammond EC, Frasca JM. Adenomatous lesions of the large bowel: an autopsy survey. Cancer. 1979;43:1847–1857. doi: 10.1002/1097-0142(197905)43:5<1847::aid-cncr2820430538>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 15.Vatn MH, Stalsberg H. The prevalence of polyps of the large intestine in Oslo: an autopsy study. Cancer. 1982;49:819–825. doi: 10.1002/1097-0142(19820215)49:4<819::aid-cncr2820490435>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 16.Pickhardt PJ, Choi JR, Hwang I, Butler JA, Puckett ML, Hildebrandt HA, Wong RK, Nugent PA, Mysliwiec PA, Schindler WR. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003;349:2191–2200. doi: 10.1056/NEJMoa031618. [DOI] [PubMed] [Google Scholar]
- 17.Kim DH, Pickhardt PJ, Taylor AJ, Leung WK, Winter TC, Hinshaw JL, Gopal DV, Reichelderfer M, Hsu RH, Pfau PR. CT colonography versus colonoscopy for the detection of advanced neoplasia. N Engl J Med. 2007;357:1403–1412. doi: 10.1056/NEJMoa070543. [DOI] [PubMed] [Google Scholar]
- 18.Rex DK, Kahi C, O'Brien M, Levin TR, Pohl H, Rastogi A, Burgart L, Imperiale T, Ladabaum U, Cohen J, et al. The American Society for Gastrointestinal Endoscopy PIVI (preservation and incorporation of valuable endoscopic innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2011;73:419–422. doi: 10.1016/j.gie.2011.01.023. [DOI] [PubMed] [Google Scholar]
- 19.Terry MB, Neugut AI, Bostick RM, Sandler RS, Haile RW, Jacobson JS, Fenoglio-Preiser CM, Potter JD. Risk factors for advanced colorectal adenomas: a pooled analysis. Cancer Epidemiol Biomarkers Prev. 2002;11:622–629. [PubMed] [Google Scholar]
- 20.Chaput U, Alberto SF, Terris B, Beuvon F, Audureau E, Coriat R, Roche H, Gaudric M, Prat F, Chaussade S. Risk factors for advanced adenomas amongst small and diminutive colorectal polyps: a prospective monocenter study. Dig Liver Dis. 2011;43:609–612. doi: 10.1016/j.dld.2011.02.002. [DOI] [PubMed] [Google Scholar]
- 21.Martínez ME, Sampliner R, Marshall JR, Bhattacharyya AK, Reid ME, Alberts DS. Adenoma characteristics as risk factors for recurrence of advanced adenomas. Gastroenterology. 2001;120:1077–1083. doi: 10.1053/gast.2001.23247. [DOI] [PubMed] [Google Scholar]
- 22.Nusko G, Mansmann U, Partzsch U, Altendorf-Hofmann A, Groitl H, Wittekind C, Ell C, Hahn EG. Invasive carcinoma in colorectal adenomas: multivariate analysis of patient and adenoma characteristics. Endoscopy. 1997;29:626–631. doi: 10.1055/s-2007-1004268. [DOI] [PubMed] [Google Scholar]
- 23.Rex DK, Goldblum JR. Pro: Villous elements and high-grade dysplasia help guide post-polypectomy colonoscopic surveillance. Am J Gastroenterol. 2008;103:1327–1329. doi: 10.1111/j.1572-0241.2008.02005_2.x. [DOI] [PubMed] [Google Scholar]