

Abstract
The aim of this study is to assess the actual epidemiologic features of Kawasaki disease (KD) in Korea using the data from Health Insurance Review & Assessment Service (HIRA) claims from 2007 to 2014. We investigated HIRA claims of patients who had KD (International Classification of Diseases-10, M30.3) as a major diagnosis and were given intravenous immunoglobulin (IVIG) from 2007 to 2014. A total of 39,082 patients were reported during the period. The male-to-female ratio was 1.42 and the median age was 28 months. The incidence rates were 168.3 per 100,000 population aged 0 to 4 years in 2007, 159.1 in 2008, 167.3 in 2009, 190.4 in 2010, 188.2 in 2011, 190.2 in 2012, 210.4 in 2013 and 217.2 in 2014. These rates were much higher than those in the previous studies in Korea. KD occurred more often in early summer (May, June and July) and winter (December and January). The annual incidence rate of KD had been increasing every year, reaching 217.2 per 100,000 population aged 0 to 4 years in 2014. It is the second highest incidence rate of KD in the world after Japan.
Keywords: Kawasaki Disease, Epidemiology, Annual Incidence, Korea
Graphical Abstract
INTRODUCTION
Kawasaki disease (KD) is well known as the disease causing acute systemic vasculitis that predominantly affects children younger than 5 years of age (1). KD has become a leading cause of acquired heart diseases among children in developed countries, replacing rheumatic heart disease (2). After Dr. Tomisaku Kawasaki described KD first in 1967, KD has been reported all over the world, while its incidence rates varied among countries. High incidence rates were noted in Northeast Asia, especially Japan and Korea, and the incidence rate of KD has been increasing continually in both countries (3,4,5,6,7,8,9,10,11). The incidence rate of KD in Japan was 264.8 per 100,000 population aged 0 to 4 years in 2012, which was the highest incidence rate in the world (3).
In Korea, the first nationwide survey for KD was conducted from 1991 to 1993. Since then, surveys have been conducted at an interval of 3 years to investigate the incidence rates and epidemiologic features of KD (6,7,8,9,10,11). According to the latest survey conducted from 2009 to 2011, the incidence rates were 115.4 per 100,000 population aged 0 to 4 years in 2009, 132.9 in 2010 and 134.4 in 2011 (6). These results were obtained from a retrospective survey collecting data through questionnaires for patients with KD who were admitted to the hospitals with the pediatric residency program (6,7,8,9,10,11). The results might not represent the actual incidence rate of KD.
In this study, we attempted to get close to the actual epidemiologic features of KD in Korea by using Health Insurance Review & Assessment Service (HIRA) claims from 2007 to 2014.
MATERIALS AND METHODS
We investigated HIRA claims of the patients who received IVIG under the diagnosis of KD (ICD-10, M30.3) from January 2007 through December 2014. The annual-incidence rate of KD was calculated by dividing the number of newly diagnosed KD patients who were younger than 5 years old by the total number of children at the same range of age in each year, and it was described as the number of patients with KD per 100,000 children younger than 5 years old. The data on the Korean population were acquired from the database of the Statistics Korea.
For descriptive analyses, frequencies and percentages were calculated for categorical variables, and means and standard deviations were calculated for continuous variables. All statistical analyses were performed using the R program.
Ethics statement
This study was approved by the institutional review board of Severance Hospital, Yonsei University Health System on September 1, 2015 (IRB approval number: 4-2015-0643). Informed consent was waived by the board.
RESULTS
Age and gender distributions
The sum of patients with KD during the study period was 39,082 (4,477 in 2007, 4,208 in 2008, 4,364 in 2009, 4,970 in 2010, 4,869 in 2011, 5,013 in 2012, 5,519 in 2013 and 5,662 in 2014). There were 22,907 male and 16,175 female patients. The male-to-female ratio was 1.42, and the ratio was relatively constant during the period (1.47 in 2007, 1.52 in 2008, 1.44 in 2009, 1.43 in 2010, 1.38 in 2011, 1.37 in 2012, 1.40 in 2013 and 1.37 in 2014) (Fig. 1). The mean age at the diagnosis of KD was 32.6 ± 24.4 months, and the median age was 28 months with a range of 1 month and 17 years. Most patients were young children: the number of the patients younger than 5 years old were 34,346 and the average proportion of them was 87.9% during the period (87.1% in 2007, 87.1% in 2008, 87.3% in 2009, 87.4% in 2010, 89.4% in 2011, 88.2% in 2012, 88.1% in 2013 and 88.1% in 2014) (Table 1).
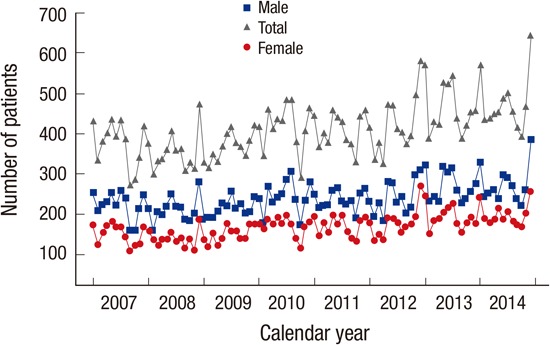
Fig. 1.

Total number of patients with KD by calendar year, 2007-2014.
The sum of patients with KD during the study period was 39,082 (4,477 in 2007, 4,208 in 2008, 4,364 in 2009, 4,970 in 2010, 4,869 in 2011, 5,013 in 2012, 5,519 in 2013 and 5,662 in 2014). There were 22,907 male and 16,175 female patients.
Table 1. Incidence rate of KD in children younger than 5 years of age by calendar year, 2007-2014.
| Year | No. of total patients | Population < 5 yr | Patients < 5 yr | Incidence per 100,000 | ||
|---|---|---|---|---|---|---|
| Total | Male | Female | ||||
| 2007 | 4,477 | 2,316,155 | 3,899 | 168.3 | 195.5 | 139.1 |
| 2008 | 4,208 | 2,302,912 | 3,665 | 159.1 | 185.4 | 131.0 |
| 2009 | 4,364 | 2,276,742 | 3,810 | 167.3 | 190.1 | 143.0 |
| 2010 | 4,970 | 2,281,200 | 4,343 | 190.4 | 217.4 | 161.7 |
| 2011 | 4,869 | 2,313,461 | 4,355 | 188.2 | 211.4 | 163.6 |
| 2012 | 5,013 | 2,324,347 | 4,422 | 190.2 | 215.1 | 163.9 |
| 2013 | 5,519 | 2,310,731 | 4,862 | 210.4 | 240.3 | 178.8 |
| 2014 | 5,662 | 2,297,244 | 4,990 | 217.2 | 244.5 | 188.4 |
Annual incidence rate
The annual incidence rate of KD had been markedly increasing every year from 168.3 per 100,000 population aged 0 to 4 years in 2007 to 217.2 in 2014, with two small peaks in 2007 and 2010 (168.3 in 2007 and 190.4 in 2010) (Table 1). The annual incidence rates of KD in male were 195.5 per 100,000 population aged 0 to 4 years in 2007, 185.4 in 2008, 190.1 in 2009, 217.4 in 2010, 211.4 in 2011, 215.1 in 2012, 240.3 in 2013, and 244.5 in 2014. The annual incidence rates of KD in female were 139.1 per 100,000 population aged 0 to 4 years in 2007, 131.0 in 2008, 143.0 in 2009, 161.7 in 2010, 163.6 in 2011, 163.9 in 2012, 178.8 in 2013, and 188.4 in 2014.
Age-specific incidence rate
The age-specific incidence rate was the highest in children under 1 year of age, and gradually decreased with age, becoming below 100.0 per 100,000 population after 5 years (Fig. 2). The age-specific incidence rates were 245.7 per 100,000 population under 1 year, 222.8 in age 1, 198.3 in age 2, 160.0 in age 3, 108.7 in age 4, 59.8 in age 5, 29.6 in age 6, 12.6 in age 7, 7.5 in age 8, 4.1 in age 9, and 2.4 in age 10. The age-specific incidence rates in male were 292.9 per 100,000 population under 1 year, 256.4 in age 1, 221.8 in age 2, 175.6 in age 3, 120.3 in age 4, 64.8 in age 5, 32.8 in age 6, 13.9 in age 7, 8.2 in age 8, 5.0 in age 9, and 2.8 in age 10. The age-specific incidence rates in female were 195.7 per 100,000 population under 1 year, 187.1 in age 1, 173.3 in age 2, 143.3 in age 3, 96.2 in age 4, 54.5 in age 5, 26.1 in age 6, 11.1 in age 7, 6.8 in age 8, 3.1 in age 9, and 2.0 in age 10.
Fig. 2.

Age-specific incidence rate of KD.
The age-specific incidence rate was the highest in children under 1 year of age, and gradually decreased with age, becoming below 100.0 per 100,000 population after 5 years.
Monthly distribution
KD occurred more often in early summer (May, June and July) and winter (December and January), and occurred less often in spring and fall. The incidence of KD was high in December (9.95% of total patients with KD) and July (9.08%), and was low in October (7.06%) and February (7.13%) (Fig. 3).
Fig. 3.

Number of patients with KD by month, 2007-2014.
KD occurred more often in early summer and winter. The incidence of KD was high in December (9.95% of total patients with KD) and July (9.08%), and was low in October (7.06%) and February (7.13%).
We observed similar seasonal variations every year. The incidence of KD was relatively high in January, May, July, and December in 2007, June and December in 2008, July and December in 2009, July, August, and December in 2010, May and December in 2011, May, June, November, and December in 2012, January and July in 2013, and January, July, and December in 2014. The incidence of KD was the lowest in September 2007 and the highest in December 2014 during the period (Fig. 4).
Fig. 4.

Number of patients with KD by month in every year, 2007-2014.
We observed similar seasonal variations every year. The incidence of KD was the lowest in September 2007 and the highest in December 2014 during the period.
DISCUSSION
The nationwide epidemiologic surveys for KD had been conducted almost every 2 years since 1970 in Japan (2,3,4,5). In the surveys, questionnaires and diagnostic guidelines for KD were mailed to all specialized pediatric hospitals and general hospitals having pediatric departments with 100 or more beds (3,4,5). The incidence rate of KD had been increasing rapidly since mid-1990s, and approximately 300,000 patients with KD were registered in Japan (3). The latest incidence rates in Japan were 243.1 per 100,000 population aged 0 to 4 years in 2011 and 264.8 in 2012 (3). Those were the highest incidence rates in the world (3).
In Korea, 5 patients with KD were first reported in 1973 and 2,224 patients with KD had been reported until 1986 (12,13). The Korean Pediatric Heart Society had been conducting nationwide epidemiologic surveys every 3 years since 1991 (6-11). They reported 1,709 patients with KD in 1991-1993, 2,680 in 1994-1996, 3,862 in 1997-1999, 9,150 in 2000-2002, 9,662 in 2003-2005, 9,039 in 2006-2008, and 13,031 in 2009-2011 (6-11). The results were obtained from retrospective surveys that collected data using questionnaires for the patients with KD who were admitted to the hospitals with the pediatric residency program (6,7,8,9,10,11). The results didn't include the data of the patients with KD who were admitted to the hospitals without the pediatric residency program. Therefore, the results could underestimate the actual incidence rate of KD.
In this study, we used HIRA claims of the patients who received IVIG under the diagnosis of KD (ICD-10, M30.3) from January 2007 through December 2014. The entrance into the National Health Insurance is mandatory for everyone in Korea, so we could collect the entire data of the patients with KD who received IVIG. We thought that almost all patients with KD were included in our data, although we did not include the data of some patients with KD who did not receive IVIG (93.6% of patients with KD were given IVIG between 2009 and 2011 according to the survey by the Korean Pediatric Heart Society) (6). We counted as a case when a patient received IVIG several times, and 1,142 patients (2.92% of total patients of KD) received IVIG twice or more during the period. We could not confirm the diagnosis of KD, and the presence of cardiac complications, because we just investigated HIRA claims for the use of IVIG. So the actual incidence rate of KD may be a little different with those of our study. Although our study has some limitations, it is the first attempt using the national database of patients with KD in Korea.
This study revealed again that KD occurred more often in male and the male-to-female ratio was 1.42. KD occurred mainly in children younger than 5 years and infants, and the average proportion of them was 87.9%. The incidence rate decreased markedly below 100 per 100,000 population after 5 years, and below 1 per 100,000 population after 11 years. The results were consistent with those of the previous studies in Korea and Japan (3,4,5,6,7,8,9,10,11).
The incidence rate of KD was much higher in this study compared to those of the former surveys conducted by the Korean Pediatric Heart Society during the same period (6,7,8,9,10,11). The latest incidence rate was 217.2 per 100,000 population aged 0 to 4 years in 2014 in this study. However, both studies showed an increasing trend of the incidence rate of KD every year, and it was consistent with the results of the studies by the Japan Kawasaki Disease Research Committee (3,4,5,6,7,8,9,10,11). Because the cause of KD is still unknown, the reason for the increase in the incidence rate is also unknown. If the cause of KD is infection, changes in the toxicity of causative microorganisms may be the reason for the increasing incidence rate (5). The increased awareness of KD among physicians and the general population in Korea may be another reason (6). Anyway, the incidence rate of KD in Korea is the second highest in the world after Japan (Table 2) (3). We also observed that there were two small peaks of incidences of KD in 2007 and 2010 in Korea (Table 2). It may imply that infectious agents might be the cause of KD.
Table 2. Comparison of incidence rates of KD in children younger than 5 years of age (No./ 100,000).
| Year | Incidence rate in the surveys by the Korean Pediatric Heart Society (6-8) | Incidence rate in this study | Incidence rate in the surveys by the Japan Kawasaki Disease Research Committee (3-5) |
|---|---|---|---|
| 2004 | 106.4 | 174.0 | |
| 2005 | 104.6 | 181.1 | |
| 2006 | 108.7 | 188.1 | |
| 2007 | 118.3 | 168.3 | 215.3 |
| 2008 | 112.5 | 159.1 | 218.6 |
| 2009 | 115.4 | 167.3 | 206.2 |
| 2010 | 132.9 | 190.4 | 239.6 |
| 2011 | 134.4 | 188.2 | 243.1 |
| 2012 | 190.2 | 264.8 | |
| 2013 | 210.4 | ||
| 2014 | 217.2 |
Taiwan reported that the incidence rate of KD was 66 per 100,000 population aged 0 to 4 years from 1996 to 2002, and 69 from 2003 to 2006 (14,15). Taiwan has the third highest incidence rate of KD in the world. China reported that the incidence rate of KD was 18.2-27.8 per 100,000 population aged 0 to 4 years from 1995 to 1999 and 40.9-55.1 from 2000 to 2004 in Beijing (16,17). In addition, the incidence rate was 16.79-36.76 per 100,000 population aged 0 to 4 years from 1998 to 2002 and 46.3 from 2003 to 2007 in Shanghai, and 26 from 1994 to 1997 and 39 from 1997 to 2000 in Hong Kong (18,19,20). An increasing trend of the incidence rate of KD was also distinctive in China, as in Japan and Korea. However, the incidence rate of KD was much lower in other continents. The incidence rate of KD was reported below 10 per 100,000 population aged 0 to 4 years in several countries in Europe (England, Denmark, Sweden, Finland, France, and Netherlands) (21,22,23,24,25). In Australia, the average annual incidence rate was 2.82 per 100,000 population aged 0 to 4 years from 1980 to 1989, 7.96 from 1990 to 1999, and 9.34 from 2000 to 2009 (26). In Canada, the average annual incidence rate was 14.4 per 100,000 population aged 0 to 4 years from 1995 to 1997 and 26.2 from 2004 to 2006 (27). In the United States, the hospitalization rate for KD was 17.5 per 100,000 population aged 0 to 4 years in 1997, 17.1 in 2000, 19.6 in 2003, and 20.8 in 2006 (28,29). The increasing trend of the incidence rate of KD was disdinctive in Northeast Asia, but was not in other continents (29). We postulated that some genetic or environmental factors might involve the difference.
This study revealed relatively high incidence rates of KD in winter and summer with small variations in each year. It was similar to the results of former studies in Korea and Japan, but was different from those of studies in Beijing, Shanghai, and Taiwan, in which they observed relatively high incidence rates in spring and summer (3,4,5,6,7,8,9,10,11,14,15,16,17,18,19). We postulated that Korea and Japan showed similar seasonal variations, because the two countries are very close geographically to each other and have similar climates, in contrast to China and Taiwan. Such seasonal variations in the incidence rate of KD were noted across the non-tropical Northern hemisphere, and were not in the tropics and the Southern hemisphere (30). It may imply that possible causative agents of KD may be mainly spread in the non-tropical Northern hemisphere and be predominant in some seasons in the regions (30). Therefore we could postulate that KD might be caused by infectious agents, and some genetic or environmental factors might influence the occurrence of KD.
In conclusion, this study was the first attempt using the national database including the patients with KD who were given IVIG, and showed that the incidence rates of KD in Korea were much higher than those of the former surveys by the Korean Pediatric Heart Society during the same period. In addition, the incidence rates had been increasing every year, reaching 217.2 per 100,000 population aged 0 to 4 years in 2014. It was the second highest incidence rate in the world after Japan.
Footnotes
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conception and design of this study: Ha S, Seo GH, Kim DS. Acquisition, analysis and interpretation of data: Seo GH. Writing manuscript: Ha S. Critical review: Kim KY, Kim DS. Approval of final draft: all authors.
References
- 1.Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. 1967;16:178–222. [PubMed] [Google Scholar]
- 2.Taubert KA. Epidemiology of Kawasaki disease in the United States and worldwide. Prog Pediatr Cardiol. 1997;6:181–185. [Google Scholar]
- 3.Makino N, Nakamura Y, Yashiro M, Ae R, Tsuboi S, Aoyama Y, Kojo T, Uehara R, Kotani K, Yanagawa H. Descriptive epidemiology of Kawasaki disease in Japan, 2011-2012: from the results of the 22nd nationwide survey. J Epidemiol. 2015;25:239–245. doi: 10.2188/jea.JE20140089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nakamura Y, Yashiro M, Uehara R, Sadakane A, Tsuboi S, Aoyama Y, Kotani K, Tsogzolbaatar EO, Yanagawa H. Epidemiologic features of Kawasaki disease in Japan: results of the 2009-2010 nationwide survey. J Epidemiol. 2012;22:216–221. doi: 10.2188/jea.JE20110126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nakamura Y, Yashiro M, Uehara R, Oki I, Watanabe M, Yanagawa H. Epidemiologic features of Kawasaki disease in Japan: results from the nationwide survey in 2005-2006. J Epidemiol. 2008;18:167–172. doi: 10.2188/jea.JE2008001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kim GB, Han JW, Park YW, Song MS, Hong YM, Cha SH, Kim DS, Park S. Epidemiologic features of Kawasaki disease in South Korea: data from nationwide survey, 2009-2011. Pediatr Infect Dis J. 2014;33:24–27. doi: 10.1097/INF.0000000000000010. [DOI] [PubMed] [Google Scholar]
- 7.Park YW, Han JW, Hong YM, Ma JS, Cha SH, Kwon TC, Lee SB, Kim CH, Lee JS, Kim CH. Epidemiological features of Kawasaki disease in Korea, 2006-2008. Pediatr Int. 2011;53:36–39. doi: 10.1111/j.1442-200X.2010.03178.x. [DOI] [PubMed] [Google Scholar]
- 8.Park YW, Han JW, Park IS, Kim CH, Cha SH, Ma JS, Lee JS, Kwon TC, Lee SB, Kim CH, et al. Kawasaki disease in Korea, 2003-2005. Pediatr Infect Dis J. 2007;26:821–823. doi: 10.1097/INF.0b013e318124aa1a. [DOI] [PubMed] [Google Scholar]
- 9.Park YW, Han JW, Park IS, Kim CH, Yun YS, Cha SH, Ma JS, Lee SB, Kim CH, Lee HJ, et al. Epidemiologic picture of Kawasaki disease in Korea, 2000-2002. Pediatr Int. 2005;47:382–387. doi: 10.1111/j.1442-200x.2005.02079.x. [DOI] [PubMed] [Google Scholar]
- 10.Park YW, Park IS, Kim CH, Ma JS, Lee SB, Kim CH, Yun YS, Lee HJ, Lee SK, Tockgo YC. Epidemiologic study of Kawasaki disease in Korea, 1997-1999: comparison with previous studies during 1991-1996. J Korean Med Sci. 2002;17:453–456. doi: 10.3346/jkms.2002.17.4.453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Park YW, Kim CH, Park IS, Ma JS, Lee SB, Kim CH, Yun YS, Lee KS, Lee SK, Tockgo YC. Epidemiologic study of Kawasaki disease in Korea, 1994-1996: comparison of previous study in 1991-1993. J Korean Pediatr Soc. 1999;42:1255–1260. [Google Scholar]
- 12.Park JS, Seo CJ, Cho SH, Lee DB. Clinical observation of mucocutaneous lymph node syndrome: 5 cases. J Korean Pediatr Soc. 1973;16:61–67. [Google Scholar]
- 13.Lee DB. Epidemiologic study of Kawasaki disease in Korea. Prog Clin Biol Res. 1987;250:55–60. [PubMed] [Google Scholar]
- 14.Huang WC, Huang LM, Chang IS, Chang LY, Chiang BL, Chen PJ, Wu MH, Lue HC, Lee CY, Kawasaki Disease Research Group Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics. 2009;123:e401–5. doi: 10.1542/peds.2008-2187. [DOI] [PubMed] [Google Scholar]
- 15.Chang LY, Chang IS, Lu CY, Chiang BL, Lee CY, Chen PJ, Wang JT, Ho HN, Chen DS, Huang LM, Kawasaki Disease Research Group Epidemiologic features of Kawasaki disease in Taiwan, 1996-2002. Pediatrics. 2004;114:e678–82. doi: 10.1542/peds.2004-0726. [DOI] [PubMed] [Google Scholar]
- 16.Du ZD, Zhao D, Du J, Zhang YL, Lin Y, Liu C, Zhang T, Beijing Kawasaki Research Group Epidemiologic study on Kawasaki disease in Beijing from 2000 through 2004. Pediatr Infect Dis J. 2007;26:449–451. doi: 10.1097/01.inf.0000261196.79223.18. [DOI] [PubMed] [Google Scholar]
- 17.Du ZD, Zhang T, Liang L, Meng X, Li T, Kawasaki T, Nakamura Y, Yanagawa H. Epidemiologic picture of Kawasaki disease in Beijing from 1995 through 1999. Pediatr Infect Dis J. 2002;21:103–107. doi: 10.1097/00006454-200202000-00004. [DOI] [PubMed] [Google Scholar]
- 18.Ma XJ, Yu CY, Huang M, Chen SB, Huang MR, Huang GY, Shanghai Kawasaki Research Group Epidemiologic features of Kawasaki disease in Shanghai from 2003 through 2007. Chin Med J (Engl) 2010;123:2629–2634. [PubMed] [Google Scholar]
- 19.Huang GY, Ma XJ, Huang M, Chen SB, Huang MR, Gui YH, Ning SB, Zhang TH, Du ZD, Yanagawa H, et al. Epidemiologic pictures of Kawasaki disease in Shanghai from 1998 through 2002. J Epidemiol. 2006;16:9–14. doi: 10.2188/jea.16.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ng YM, Sung RY, So LY, Fong NC, Ho MH, Cheng YW, Lee SH, Mak WC, Wong DM, Yam MC, et al. Kawasaki disease in Hong Kong, 1994 to 2000. Hong Kong Med J. 2005;11:331–335. [PubMed] [Google Scholar]
- 21.Harnden A, Alves B, Sheikh A. Rising incidence of Kawasaki disease in England: analysis of hospital admission data. BMJ. 2002;324:1424–1425. doi: 10.1136/bmj.324.7351.1424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Harnden A, Mayon-White R, Perera R, Yeates D, Goldacre M, Burgner D. Kawasaki disease in England: ethnicity, deprivation, and respiratory pathogens. Pediatr Infect Dis J. 2009;28:21–24. doi: 10.1097/inf.0b013e3181812ca4. [DOI] [PubMed] [Google Scholar]
- 23.Fischer TK, Holman RC, Yorita KL, Belay ED, Melbye M, Koch A. Kawasaki syndrome in Denmark. Pediatr Infect Dis J. 2007;26:411–415. doi: 10.1097/01.inf.0000259964.47941.00. [DOI] [PubMed] [Google Scholar]
- 24.Schiller B, Fasth A, Björkhem G, Elinder G. Kawasaki disease in Sweden: incidence and clinical features. Acta Paediatr. 1995;84:769–774. doi: 10.1111/j.1651-2227.1995.tb13753.x. [DOI] [PubMed] [Google Scholar]
- 25.Heuclin T, Dubos F, Hue V, Godart F, Francart C, Vincent P, Martinot A, Hospital Network for Evaluating the Management of Common Childhood Diseases Increased detection rate of Kawasaki disease using new diagnostic algorithm, including early use of echocardiography. J Pediatr. 2009;155:695–699.e1. doi: 10.1016/j.jpeds.2009.04.058. [DOI] [PubMed] [Google Scholar]
- 26.Saundankar J, Yim D, Itotoh B, Payne R, Maslin K, Jape G, Ramsay J, Kothari D, Cheng A, Burgner D. The epidemiology and clinical features of Kawasaki disease in Australia. Pediatrics. 2014;133:e1009–14. doi: 10.1542/peds.2013-2936. [DOI] [PubMed] [Google Scholar]
- 27.Lin YT, Manlhiot C, Ching JC, Han RK, Nield LE, Dillenburg R, Pepelassis D, Lai LS, Smythe JF, Chahal N, et al. Repeated systematic surveillance of Kawasaki disease in Ontario from 1995 to 2006. Pediatr Int. 2010;52:699–706. doi: 10.1111/j.1442-200X.2010.03092.x. [DOI] [PubMed] [Google Scholar]
- 28.Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29:483–488. doi: 10.1097/INF.0b013e3181cf8705. [DOI] [PubMed] [Google Scholar]
- 29.Uehara R, Belay ED. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J Epidemiol. 2012;22:79–85. doi: 10.2188/jea.JE20110131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Burns JC, Herzog L, Fabri O, Tremoulet AH, Rodó X, Uehara R, Burgner D, Bainto E, Pierce D, Tyree M, et al. Seasonality of Kawasaki disease: a global perspective. PLoS One. 2013;8:e74529. doi: 10.1371/journal.pone.0074529. [DOI] [PMC free article] [PubMed] [Google Scholar]