

Abstract
Among the running field tests that measure aerobic fitness indirectly, the 20-m shuttle run test is the one most commonly used among obese youth. However, this back and forth running test induces premature cessation of exercise in this population. The present study aimed to examine the psycho-physiological responses of obese adolescents to an intermittent (15-15) progressive and maximal run test as compared with a continuous shuttle run test. Eleven obese adolescents (age: 14-15 years; BMI = 34.01 ± 5.30 kg·m-2) performed both tests. A two-way ANOVA examined the main effects of the running test, participant’s sex, and their interaction on maximal aerobic performance (net exercise duration and final velocity), physiological values (heart rate, pulmonary oxygen uptake, respiratory exchange ratio and blood lactate concentration) and psychological responses (rating of perceived exertion, and physical self-perceptions). Oxygen uptake and heart-rate values at 9 km·h-1 were also compared. Compared with a 20-m shuttle run, the 15-15 test induced lower pulmonary oxygen uptake values at 9 km/h (28.3 ± 2.7 vs. 35.4 ± 2.7 ml·min-1·kg-1) and finished with higher maximal velocity and net exercise duration (566 ± 156 vs. 346 ± 156 s, p < 0.001), with no inter-test physiological difference. The 15-15 test also resulted in higher ratings of perceived exertion (16.0 ± 1.2 vs. 12.7 ± 1.6, p < 0.001) and improved perceived physical condition compared with the 20-m shuttle run (+1.4 ± 1.4 vs. +0.2 ± 1.0, p < 0.05). Both tests induced a maximal aerobic power of obese adolescents, but the 15-15 test provided a more progressive speed increment and longer exercise duration. The 15-15 test also elicited a significant improvement of perceived physical condition. In conclusion the 15-15 test can be considered a relevant field test for assessing the aerobic fitness of obese adolescents.
Key points.
In agreement with the previous results of Rey et al. (2013), the present study shows that obese adolescents demonstrated similar maximum physiological responses in both tests. However, they reached significantly higher running speeds and reported higher perceived physical condition in the 15-15 compared with a 20-m shuttle run test.
The 15-15 intermittent test is considered more suitable for obese adolescents, rather than the shuttle run test due to its progressive nature and its lack of directional change.
This 15-15 intermittent test will be helpful for practitioners to assess and promote exercise programs of similar nature and to promote perceived physical condition of obese adolescents.
Key words: Running test, aerobic fitness, paediatric obesity, physical self
Introduction
The worldwide trend of an increased sedentary state and obesity among youth calls for continued efforts to combat them. To this end, frequent and objective assessment of physical fitness, including cardiorespiratory fitness, should be promoted rather than solely relying on subjective assessment of exercise (Kyröläinen et al., 2010). However, although most exercise interventions for obese youth have been of aerobic type (for a review, see Paes et al., 2015), there is still a lack of appropriate running field tests allowing personalized training for cardiorespiratory fitness in this group.
Among the running field tests used to estimate cardiorespiratory fitness, the multistage 20-metre shuttle run developed by Léger et al. (1988) is the most commonly used among young people of normal weight (Olds et al., 2006; Voss and Sandercock, 2009) and adapted for overweight and obese youth with additional lower speed starting steps (Klijn et al., 2007; Quinart et al., 2014). However, this test presents some limiting factors that may not be counteracted when testing such a population. In particular, the 20-m shuttle run test includes 180 degree directional changes every 20 metres that require sudden braking and push-off muscle actions. In line with the high physiological demand of directional changes reported for ball-game players while running (Dellal et al., 2010; Hatamoto et al., 2014), the 20-m shuttle run test is reported as leading to earlier and higher peak blood lactate concentrations. Consequently, exhaustion is reached at lower maximal velocity than in a similar protocol with no directional changes (Ahmaidi et al., 1992). For normal-weight participants, this bias may be compensated for by the use of prediction equations for VO2max and maximal aerobic velocity (Léger et al., 1988). These equations have been repeatedly validated for adolescents (Boreham et al., 1990; Liu et al., 1992). Although obese youth require a greater proportion of their aerobic capacity to conduct weight-bearing physical activities (Ratel et al., 2006; Peyrot et al., 2009), and will be particularly affected by the directional changes due to their increased body mass, such equations are lacking for this population. To our knowledge, only the study of Quinart et al. (2014) has developed a prediction equation for the peak pulmonary oxygen uptake among obese adolescents taking into consideration sex and body mass index. Nevertheless, despite the use of this equation, maximal aerobic running velocity remains underestimated because running performance is considered as the final completed step (Cairney et al., 2008). This restricted performance evaluation and an early stop are often observed when this test is used with obese youth and the latter represent a clear methodological limitation for individual adjustments of training programme intensity (e.g., Bovet et al., 2007; Castro-Pineiro et al., 2011). Furthermore, it is expected that the early stop induced by a 20-m shuttle run test and the associated underestimation of the actual performance lead these adolescents to perceive themselves as physically less competent, especially regarding their objective physical condition. This is problematic as they are already characterized by significantly lower levels of physical self-perceptions than their normal-weight peers (e.g., Hau et al., 2005; Marsh et al., 2007). This is of major importance because physical self-perceptions are considered central for exercise motivation and, by extension, for adherence to exercise (Berger, 2004). If we consider the physical self-concept as a dynamic construct (i.e., sensitive to events or situation-specific), it can be hypothesized that the perceived physical condition of obese adolescents may be particularly influenced by their positive or negative experience (Ninot et al., 2004). In particular, they could perceive their physical abilities through their performances in a physical fitness test.
In order to circumvent the aforementioned limitation of a 20-m shuttle run among obese adolescents, an intermittent-type (15-15) of progressive and maximal running test has recently been developed (Rey et al., 2013). The intermittent type of run with intermediate passive rest periods of 15 seconds and the absence of sudden directional changes allowed the obese adolescents to reach significantly higher final velocities (Vpeak; 11.5 vs. 9.4 km·h-1) and net running times (8.7 vs. 5.3 min) than in the standard shuttle run test, while reaching similar peak heart-rate values and ratings of perceived exertion (RPE). To complete these initial findings, inter-test comparison of the direct pulmonary oxygen uptake measures remains to be assessed. An additional and promising advantage of the 15-15 test lies in the fact that it provides peak velocity values that should favour the individual setting of high intensity interval training (HIIT). Compared with traditional forms of continuous exercise, HIIT-type training has been recently highlighted as significantly efficient for improving cardiorespiratory fitness (Lau et al., 2015), perceived pleasure (Bartlett et al., 2011) and health perception (Shepherd et al., 2015) among overweight and obese youth. Based on this information it can be hypothesized that the aforementioned advantage of the 15-15 test will lead obese youth to perceive themselves as physically more competent.
The present study aims at investigating the combined physiological and psychological responses of obese adolescents to an intermittent progressive and maximal running test (15-15 test) compared with a 20-m shuttle run test. The 15-15 test is expected to generate similar peak heart rate, peak pulmonary oxygen uptake and RPE values to the 20-m shuttle run test, while resulting in significant improvements in running performance (Vpeak) and in perceived physical condition.
Methods
Participants and procedures
Eleven 14-15 year old obese adolescents (5 girls and 6 boys, male and female Tanner stage 3-4) schooled in a pediatric rehabilitation center participated in the present study. All of them were defined as obese according to the International Obesity Task Force’s cut-off based on body mass and height (Cole et al., 2000). None of the participants had undergone medical treatment or possessed any metabolic disorder, cardiac or orthopedic pathology that might have interfered with the tests.
The protocol was constructed in accordance with the Declaration of Helsinki and met the French ethical requirements for human research. Permission to conduct the study was first obtained from the administration and medical staff of the pediatric rehabilitation center. An information letter was then sent to the adolescents’ parent or legal representative, and only adolescents who returned the signed consent forms participated. All tests were conducted under the supervision of the medical staff of the pediatric rehabilitation center.
Running test protocol
The protocol included two progressive and maximal running tests, a continuous 20-m shuttle run test (Léger et al., 1988) and the intermittent 15-15 test (Rey et al., 2013). Both running tests were performed one month after the participants’ arrival in the pediatric rehabilitation centre and were preceded by a test familiarization session with accompanying investigators at low velocity (warm-up and first stage). The actual running tests were randomly and individually performed at a 48-h interval and in the same conditions (e.g. no spectators except the investigation staff, same time of the day, same timed normative encouragement sentences for both tests).
The 20-m shuttle run test involves running continuously back and forth between two lines 20 metres apart. The runs are synchronized with a pre-recorded audio CD, which plays audio sounds (‘beeps’) at pre-set intervals. The starting speed is set for 1 min of warm-up at 8 km/h before being progressively incremented by 0.5 km·h-1 per stage (1 min) until it was impossible for the runner to keep in synchrony with the beeps at the lines twice consecutively.
The 15-15 test differs from the 20-m shuttle run test by its intermittent rather than continuous form and by the absence of 180° directional changes. In this test, the warm-up stage is set at 8 km·h-1 with successive speed increments of 1 km·h-1 every 3 min. Each stage includes 3 back and forth runs performed in a 15/15 way, with 15 seconds to reach a given stage mark, 15 s to rest passively at the mark and 15 s to come back to the start line. As in the 20-m shuttle run test, the runners are stopped by the experimenter when they cannot keep in synchrony with the beeps at the stage marks twice in succession. As illustrated in the Appendix, this test requires a rectangular track of 75 x 10 m to be constructed using different marks set at the distances corresponding to each running speed (from 33.36 m at 8 km·h-1 to 75.06 m at 18 km·h-1, by increments of 4.17 m per stage).
Measurements
All anthropometric measures were performed by the medical staff. They included the participants’ height using a Harpenden stadiometer (with a precision of ± 1.0 cm) and their body mass, percentage of body fat (Cole et al., 2005), and fat-free mass, using a Tanita® impedance measurement device (BC 418, Japan).
Running performance was evaluated through the net run duration (excluding the intermediate rest periods) and the peak velocity value (Vpeak), which took into account the last fully completed stage and additional run time. In the 15-15 test, Vpeak was adjusted by 0.33 km·h-1 per additional minute run (i.e., every third of the last step duration). In the 20-m shuttle run test, the adjustment was 0.25 km·h-1 per 15 s (i.e., every quarter of the last step duration).
Physiological measurements were performed at rest, during and after each running test as follows:
The respiratory and pulmonary gas-exchange variables were measured using a breath-by-breath telemetric gas analyzer (Cosmed® K4 b², Rome, Italy) for 1 minute at standing rest and every 5 seconds during the time course of each running test. The initial calibration was performed according to the manufacturer’s instructions. The peak pulmonary oxygen uptake (VO2peak) was obtained for the 20-m shuttle run test by averaging the last four consecutive VO2 values of the last minute to avoid artifacts. For the 15-15 test, the four highest values of the last step of 3 minutes were averaged taking account of the variability of VO2 during resting periods. The respiratory exchange ratio (RER) was also calculated as the ratio of the expired volume of carbon dioxide and inspired volume of oxygen (VCO2 / VO2).
Blood lactate concentration [La-]b was measured using a validated (Pyne et al., 2000) portable lactate analyzer (Lactate Pro®, Arkray, Japan). Taking account of the time-delay of lactate diffusion into the blood, and to obtain the peak [La-]b value, a blood sample was taken by the medical staff from the participants’ earlobe 3 minutes after each running test (e.g., Poortmans and Boisseau, 2003).
Heart rate (HR) was recorded throughout each test (Polar® RS 400, Polar Electro Oy, Kempele, Finland). Peak heart-rate value (HRpeak) was calculated similarly to the method used for the VO2peak. In order to compare the metabolic cost at the same sub-maximal velocity in both tests, VO2 and HR values were also measured at the 9 km·h-1-step (third minute of the net run duration), which corresponded to the highest stage reached by each runner in both tests.
Rating of perceived exertion was expressed by each participant immediately after each running test on a 6–20 scale (Borg, 1982) validated for adolescents (Eston and Williams, 1986). This scale was introduced and explained to the participants during the familiarization session.
Physical self-perceptions were measured before and after each test, using a revised version of the validated physical self-inventory with six items (PSI-6b; Ninot et al., 2001, 2006). The PSI-6b measures global self-esteem and the five physical self-perceptions proposed by Fox and Corbin (1989). It has been used with obese adolescents (e.g., Mercier et al., 2010) and includes six items measuring six physical self-dimensions: global self-worth (GSW; “Globally, I have a good opinion of myself”), physical self-worth (PSW; “I am proud of what I can do physically”), physical condition (PC; “I am satisfied with my physical endurance”), sport competence (SC; “I am satisfied with my sport competencies”), physical attractiveness (PA; “I am satisfied with my body appearance”), and physical strength (PS; “I am satisfied with my physical strength”). Participants answered each item using a visual analog scale (VAS; a 10-centimetre horizontal segment defined by two extreme anchors: not at all and absolutely). More specifically, they were asked to indicate, by marking a perpendicular line on the VAS, the extent to which the above-mentioned items characterized their present state. Consequently, the position of the perpendicular line on the VAS was a function of the intensity of their present state. The VAS has been specifically developed to increase sensitivity and fluctuation in participants’ responses (Ninot et al., 2006). The VAS was introduced and explained to participants during familiarization. Each trait was measured to a precision of one decimal place. To facilitate comparison with the physiological measures, only the pre-post delta (Δ) score (post-test – pre-test) was used.
Statistical analyses
All analyses were performed using Statistica 7.0 (Statsoft Inc., Tulsa, OK, USA). The distribution normality was assessed using a Kolmogorov-Smirnov test. An independent-samples Student’s t-test was used to examine the sex differences regarding the age and anthropometric characteristics of the participants, as well as the initial physical self-perceptions. The main effects of the running test (20-m shuttle run vs. 15-15), the participant’s sex and their interaction (“running test by sex”) on running performance (Vpeak, net test duration), physiological parameters (VO2peak, RER, [La-]b, HRpeak), and psychological measures (RPE, physical self-perceptions) were examined using a two-way analysis of variance (ANOVA). The same analysis was also used for all measures recorded at the end of the 9 km/h-step. In cases of significance (p < 0.05), a Student’s Newman-Keuls post-hoc test was used.
The effect sizes were estimated using the Cohen’s d (small effect size: 0.2 ≤ d < 0.5, medium effect size: 0.5 ≤ d < 0.8, large effect size: 0.8 ≤ d (Cohen, 1988; Norman et al., 2003) for the absolute and delta changes in significant physiological and psychological variables.
Results
Participants’ age and anthropometric characteristics
The participants’ analyses did not reveal any significant sex differences regarding age (p = 0.492), body mass (p = 0.275), BMI (p = 0.946), or body-fat percentage (p = 0.743). However, the boys were taller (p = 0.037, d = 1.38) and had a higher fat-free mass (p = 0.026, d = 1.51) compared with the girls (Table 1).
Table 1.
Participants’ demographic and anthropometric measures. Values are means (±SD).
| Total (n = 11) |
Boys (n = 6) |
Girls (n = 5) |
|
|---|---|---|---|
| Age (years) | 14.8 (.7) | 14.6 (.8) | 15.0 (.7) |
| Height (m) | 1.68 (.09) | 1.73 (.08) * | 1.62 (.06) * |
| Body mass (kg) | 96.4 (20.0) | 102.7 (25.1) | 88.9 (9.2) |
| BMI (kg·m-2) | 34.0 (5.3) | 34.1 (6.8) | 33.9 (3.6) |
| Body fat (%) | 37.3 (8.1) | 36.5 (10.5) | 38.2 (4.9) |
| Fat-free mass (kg) | 59.3 (6.5) | 63.1 (4.5)* | 54.8 (5.8) * |
BMI = body mass index.
* Significant difference (p < 0.05).
Maximal values of running performance
As shown in Table 2, significant inter-test differences were found for the maximal running performance values. The findings showed that the 15-15 test led to higher net exercise duration (F1,18 = 17.46, p < 0.001, d = 1.41) and Vpeak (F1,18 = 32.51, p < 0.001, d = 2.02) compared with the 20-m shuttle run test (Figure 1).
Table 2.
Descriptive statistics of performance, physiological and psychological measures according to the running test and the participants’ sex. Values are means (±SD).
| 15-15 | 20-m shuttle run | |||||
|---|---|---|---|---|---|---|
| Total | Boys | Girls | Total | Boys | Girls | |
| Performance measures | ||||||
| Net run duration (s) | 566(156)*** | 651(179) | 500(149) | 346(156)*** | 433(163) | 243(153) |
| Vpeak (km·h-1) | 13.09 (1.86)*** | 14.05 (2.16) | 12.36 (.72) | 9.86 (1.29)*** | 10.58 (1.33) | 9.00 (.50) |
| Physiological measures | ||||||
| HRpeak (bpm) | 190(5) | 193(4) | 187(6) | 189(6) | 190(8) | 187(4) |
| VO2peak (ml·min-1·kg-1) | 34.2 (5.0) | 36.0 (3.8) | 33.5 (5.6) | 38.4 (6.1) | 41.7 (5.4) | 34.4 (4.6) |
| RER | 1.12 (.02) | 1.13 (.02) | 1.11 (.02) | 1.11 (.04) | 1.10 (.05) | 1.13 (.02) |
| [La-]b (mmol·l-1) | 6.8 (1.9) | 6.9 (1.5) | 7.1 (2.2) | 6.3 (1.4) | 6.1 (1.6) | 6.4 (1.3) |
| Physiological measures at 9 km/h | ||||||
| VO2 (ml·min-1·kg-1) | 28.3 (2.7)*** | 28.9 (1.6) | 28.2 (3.7) | 35.4 (2.7)*** | 36.3 (2.4) | 33.4 (3.1) |
| HR (bpm) | 167(15) | 159(16) | 177(7) | 174(12) | 171(13) | 178(11) |
| Psychological measures | ||||||
| RPE | 16.0 (1.2)*** | 16.0 (1.5) | 16.0 (.7) | 12.7 (1.6)*** | 12.5 (1.8) | 13.0 (1.7) |
| Δ GSW | .2 (1.1) | -.1 (1.1) | .6 (1.1) | .0 (1.1) | -.4 (1.1) | .6 (1.0) |
| Δ PSW | .9 (1.8) | .6 (1.3) | 1.1 (2.3) | -.2 (1.4) | -.4 (1.8) | .1 (.9) |
| Δ PC | 1.4 (1.4)* | 1.3 (1.4) | 1.5 (1.5) | .2 (1.0)* | .2 (1.1) | .2 (.9) |
| Δ SC | 1.1 (1.9) | 1.1 (2.1) | 1.2 (2.0) | -.2 (1.4) | -.8 (1.2) | .6 (1.3) |
| Δ PA | .3 (1.0) | -.3 (.9) | 1.1 (.7) | -.1 (.8) | -.2 (1.0) | .1 (.3) |
| Δ PS | .6 (1.9) | .5 (2.4) | .7 (1.4) | .1 (.9) | .5 (.6) | -.3 (1.1) |
Significant inter-test (15-15 vs. 20-m shuttle run) differences: * p < 0.05;
** p < 0.01;
*** p < 0.001. SD = standard deviation. Vpeak = peak running velocity; HRpeak = peak heart rate; VO2peak = peak oxygen uptake; RER = respiratory exchange ratio; [La-]b = blood lactate concentration; RPE = rating of perceived exertion; GSW = global self-worth; PSW = physical self-worth; PC = physical condition; SC = sport competence; PA = physical attractiveness; PS = physical strength; Δ = measures of the delta between post- and pre-test.
Figure 1.
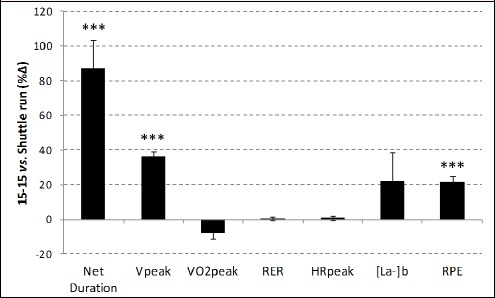
Relative inter-test difference in running performance, physiological measures and rating of perceived exertion. *** Significant difference (p < 0.001).
Additionally, a sex effect revealed that the boys ran for a higher net run duration (F1,18 = 9.03, p = 0.008, d = 1.06), and reached higher Vpeak (F1,18 = 7.47, p = 0.014, d = 1.25) compared with the girls. However, no significant “running test by sex” interaction was found.
Maximal physiological responses
No significant inter-test difference was found in any of the physiological measures (Table 2). However, a sex effect revealed that the boys reached higher VO2peak (F1,18 = 5.59, p = 0.029, d = 1.01) values than the girls (Table 2). Finally, no significant “running test by sex” interaction was found.
Physiological responses at 9 km·h-1
At 9 km·h-1 (Table 2), the 15-15 run test presented lower VO2 values than the 20-m shuttle run test (F1,18 = 22.25, p < 0.001, d = -2.63). Additional results showed that girls presented higher HR values than boys (F1,18 = 4.64, p = 0.046, d = 1.04). However, no significant sex differences were observed in VO2 (F1,18 = 2.47, p = 0.13). Finally no significant “running test by sex” interaction was observed.
Rating of perceived exertion
A higher perceived exertion (F1,18 = 24.99, p < 0.001, d = 2.33) was reported at the end of the 15-15 test (Figure 1) without any effect of sex (F1,18 = 0.341, p = 0.705) or interaction “running test by sex” (F1,18 = 0.341, p = 0.705).
Physical self-perception
At baseline, no significant difference was found for the initial physical self-perception scales between boys and girls except for PA (F2,8 = 5.76, p = 0.028). The post-hoc test revealed that the girls had lower values of PA compared with the boys (p = 0.007, d = -1.24).
After the running tests, the physical self-perceptions analysis revealed a significant difference only for the physical condition (PC) subscale (F1,18 = 5.13, p = 0.036, d = 0.99). The findings showed that the 15-15 test led to higher positive delta score levels compared with the 20-m shuttle run test (Figure 2). Additionally, a sex effect revealed that the girls showed higher and positive delta changes in PA subscale scores than the boys (F1,18 = 5.22, p = 0.035, d = 1.12). Finally, no significant “running test by sex” interaction was observed.
Figure 2.
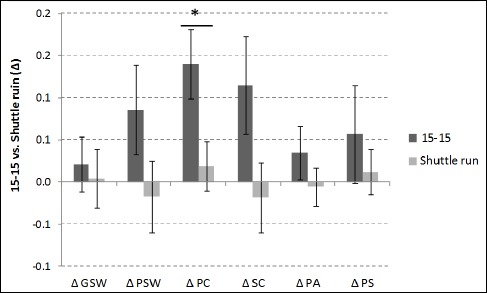
Absolute pre-post running test changes in physical self-perceptions * Significant difference (p < 0.05).
Discussion
This study aimed at investigating obese adolescents’ physiological and psychological responses to an intermittent (15-15 test) compared with the classical 20-m shuttle run test. Confirming most of our expectations, the 15-15 test generated similar maximal physiological values compared with the 20-m shuttle run test, while resulting in significant improvements in running performance and in perceived physical condition.
As reflected by the peak blood lactate concentration and RER values which were close to those reported in the literature for assessing maximal aerobic capacities (Howley et al., 1995), the 15-15 test ensured a maximal aerobic response. However, even if the HRpeak values were over the criterion of 185 bpm (Klasson-Heggebø et al., 2006) and more than 90% of theoretical maximal heart rate (using the equation of Tanaka et al. 2001), values remained slightly lower (by 6 bpm on average) than those classically reported for young people (Voss and Sandercock, 2009) or obese adolescents (Rey et al., 2013) but nearer to those reported by Quinart et al. (2014). This cannot be explained by the design of the two tests, which elicited the same level of physiological outcomes. On the other hand, higher RPE values were reported at the end of the 15-15 test compared with the 20-m shuttle run test. Although the elevated RPE values after the 15-15 test might receive some support from the increasing perception of effort reported across serial bouts of running exercise, such a difference was not found in a previous comparison of both these tests with obese adolescents (Rey et al., 2013). It can be hypothesized that the participants’ rating of perceived exertion could have been influenced by the mechanical work associated with the more intensive short bouts of running velocity in the 15-15 test. As expected, the 20-m shuttle run test led to shorter net exercise duration than the 15-15 test while resulting, in the present study, in lower mean RPE values. These low values cannot be explained by the classical HR/RPE decoupling reported in children (Groslambert and Mahon, 2006). In the absence of any major physiological difference, it can be suggested that the 20-m shuttle run test ended so rapidly (in less than 6 min) that exhaustion was not felt as maximal.
In line with the previous findings of Rey et al. (2013), the present results show that the 15-15 test allowed obese adolescents to produce a higher endurance running performance. In addition, the observed gains in both duration and Vpeak with the 15-15 test are in line with the lower maximal speed values reported by other studies when using the 20-m shuttle run test to compare obese and non-obese youth (Olds et al., 2006; Cairney et al., 2008; Castro-Pineiro et al., 2011). This inter-test difference is attributed, first, to the introduction of partial recovery periods, which are beneficial for either obese or normal-weight youth (Marinov et al., 2002; Peyrot et al., 2009), and secondly, to the absence of the costly 180° directional changes that are repeatedly performed in the 20-m shuttle run test. As reported for obese children in walking and running (Maffeis et al. 1993) and for obese adolescents in walking (Peyrot et al., 2009), weight-bearing activities are performed at a greater net metabolic cost compared with their normal-weight peers when normalized by body mass. This led these last authors to suggest that the limiting factor in aerobic-type exercises for obese individuals would rather be their motor efficiency than their cardiorespiratory system. Greater mediolateral centre of mass displacement associated with greater step widths have thus been demonstrated in walking (Peyrot et al., 2009), but data are still lacking in running, especially when including sudden directional changes. It is thus hypothesized that this biomechanical limitation can be transposed to running, in particular during a low speed, continuous and progressive design. Moreover, emphasizing the additional cost induced by the 20-m shuttle run test, the present inter-test comparison at the submaximal stage of 9 km·h-1 already revealed significantly higher relative VO2 values compared with the 15-15 test. However, because the early cessation of exercise is linked to an extra load in addition to low locomotion efficiency, it is possible that the intermittent type of running could erase such biomechanical fatigue. As recently demonstrated in ball-game players (Dellal et al., 2010), even low running velocities have relatively high physiological demands when the frequency of the directional changes increases (Hatamoto et al., 2014). Directional changes should therefore be avoided when testing obese people whose excess of body fat is already reported as negatively affecting their submaximal aerobic power (Goran et al., 2000) and energy cost (Ratel et al., 2006). These earlier results give additional support to the present choice of an intermittent running protocol with no brisk 180° directional changes.
The higher performance reached in the 15-15 test is also likely to have contributed to the pre-post improvement for boys and girls in perceived physical condition (PC). These results are noteworthy considering the lower levels of physical condition reported by obese adolescents compared with their normal-weight peers (e.g., Hau et al., 2005; Marsh et al., 2007). In the present study, the obese adolescents perceived their own PC more positively after the long and intensive effort produced in the 15-15 test. In contrast to the 20-m shuttle run test, the longer effort in the 15-15 test can be interpreted by these obese adolescents as an indicator of ‘good physical condition’. As a consequence, they may feel more competent and assess themselves more positively. First, the repeated pride experienced in intense running bouts could enhance acute physical self-efficacy (Bandura, 1977), satisfaction and pleasure. But, to our knowledge, no study has examined the acute effects of a progressive, continuous and intermittent test on physical self-perceptions of obese adolescents. Secondly, the 15-15 test acute differences in PC are original and promising and the results in line with Mercier et al. (2010), who demonstrated the situational variability of obese anxiety and self-perception. However, no effect was observed for the other perceived physical abilities (strength and sport competence) or for physical appearance. This may be explained by the fact that these other physical self-perceptions (SC, PA, and PS) were less influenced by the motor skills induced in the two running tests. Indeed, the main focus of both running tests would be to involve the physical condition of the participants.
In accordance with the literature, the findings showed that girls have significantly lower scores on perceived physical appearance than boys at baseline. These results are consistent with recent findings showing that obese girls reported lower perceived physical appearance and body attractiveness than their male counterparts (e.g., Franklin et al., 2006). Additionally, the present findings also revealed that the girls had a higher perceived physical appearance delta scores than the boys. Consequently, this study showed that the girls’ perceived physical appearance was more sensitive to their participation in the running tests compared with the boys. The reason for these results must be more clearly addressed in future research among obese adolescents.
The present study has some limitations. First, this study was performed on a single small sample of obese late adolescents. Therefore, it is unknown whether these results can be replicated with a larger sample comprising both early and late adolescents. Secondly, this sample was only composed of obese adolescents and their level of obesity was not taken into consideration. Consequently, it is unknown whether these results: (a) can be replicated with a sample of overweight adolescents, (b) could be of similar magnitude among adolescents with different types of obesity (i.e., obesity, severe obesity, and morbid obesity), (c) both tests were completed only once by participants. It is thus unknown whether the data could be replicated when these tests are used on several occasions. Finally, the number of physical self-perceptions sub-domains that were assessed in the present study was limited and these sub-domains were only assessed by one item. Consequently, it is unknown whether similar effects could be obtained using another questionnaire such as the short form of the physical self-description questionnaire (e.g., Marsh et al., 2010; Maïano et al., 2015).
Conclusion
The 15-15 test can be considered a relevant field test for assessing the aerobic fitness of obese adolescents. This test induces maximal aerobic responses through more progressive speed increments and thus longer exercises duration. Importantly for obese adolescents, it results in positive effects on perceived physical condition. Along this line, HIIT, as a condition close to the 15-15 test, is reported to induce positive impact on perceived self-efficacy and enjoyment in adults (Jung et al., 2014) and could be a worthy alternative to continuous-exercise-type training among obese adolescents. In contrast, intense and aerobic continuous forms of exercise as conditions close to the 20-m shuttle run test, are reported as unfavorable to perceived pleasure (Ekkekakis et al., 2011). The 15-15 test may thus be considered promising for assessing and individually adjusting the optimal range of running velocities and heart-rate values that could be used in HIIT programmes with obese adolescents.
Acknowledgements
We thank the pediatric rehabilitation centre, the staff and the youth of AJO® Les Oiseaux, Pediatric Obesity Follow-up and Rehabilitation Care of "Le Noble Age" group for their support and participation in the present study. No competing financial interests exist. The authors have no competing interests.
Biographies

Olivier REY
Employment
Former aggregate in Physical Education, Ecole Supérieure du Professorat et de l’Education, Aix-Marseille University
Laboratory Motricité Humaine, Sport, Sante (LAMHESS, EA 6312), France
Degree
MS
Research interests
Exercise physiology, physical activities psychology, obesity, rehabilitation, physical education
E-mail: olivier.rey@univ-amu.fr

Christophe MAÏANO
Employment
Associate Professor, Department of Psychoeducation and Psychology, Université du Québec en Outaouais (UQO), Canada
Degree
PhD
Research interests
Social psychology, psychoeducation, adapted physical activities and rehabilitation
E-mail: christophe.maiano@uqo.ca

Caroline NICOL
Employment
Senior Lecturer, Institute of Movement Sciences, UMR 7287, Aix-Marseille Université, CNRS, Marseille, France
Degree
PhD, HDR
Research interests
Neuromuscular adjustments, stretch-shortening cycle, fatigue and rehabilitation
E-mail: caroline.nicol@univ-amu.fr
Charles-Symphorien MERCIER
Employment
Medical Director, AJO® Les Oiseaux”, Pediatric Obesity Follow-up and Rehabilitation Care, Le Noble Age Group, France
Degree
PhD, MD
Research interests
Assessment of rehabilitation in obesity, nutrition, metabolic clinic trials, therapeutics, adapted physical activity
E-mail: rd.lesoiseaux@orange.fr

Jean-Marc VALLIER
Employment
Professor at the University of Toulon, France. Laboratory Motricité Humaine, Sport, Sante (LAMHESS, EA 6312), France
Degree
PhD, MD
Research interests
Exercise physiology, rehabilitation medicine, sports, medicine, neuromuscular fatigue
E-mail: vallier@univ-tln.fr
References
- Ahmaidi S., Collomp K., Préfaut C. (1992) The effect of shuttle test protocol and the resulting lactacidaemia on maximal velocity and maximal oxygen uptake during the shuttle exercise test. European Journal of Applied Physiology and Occupational Physiology 65(5), 475-479. [DOI] [PubMed] [Google Scholar]
- Bandura A. (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychological Review 84(2), 191-215. [DOI] [PubMed] [Google Scholar]
- Bartlett J.D., Close G.L., MacLaren D.P., Gregson W., Drust B., Morton J.P. (2011) High-intensity interval running is perceived to be more enjoyable than moderate-intensity continuous exercise, implications for exercise adherence. Journal of Sports Sciences 29(6), 547-553. [DOI] [PubMed] [Google Scholar]
- Berger B.G. (2004) Subjective well-being in obese individuals: The multiple roles of exercise. Quest 56(1), 50-76. [Google Scholar]
- Boreham C.A., Paliczka V.J., Nichols A.K. (1990) A comparison of the PWC170 and 20-MST tests of aerobic fitness in adolescent schoolchildren. Journal of Sports Medicine and Physical Fitness 30(1), 19-23. [PubMed] [Google Scholar]
- Borg G.A. (1982) Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise 14(5), 377-381. [PubMed] [Google Scholar]
- Bovet P., Auguste R., Burdette H. (2007) Strong inverse association between physical fitness and overweight in adolescents, a large school-based survey. International Journal of Behavioral Nutrition and Physical Activity 4 (1), 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cairney J., Hay J.A., Faught B.E., Léger L., Mathers B. (2008) Generalized self-efficacy and performance on the 20-metre shuttle run in children. American Journal of Human Biology 20(2), 132-138. [DOI] [PubMed] [Google Scholar]
- Castro-Pineiro J., Ortega F.B., Keating X.D., Gonzales-Montesinos J.L., Sjostrom M., Ruiz J.R. (2011) Percentile values for aerobic performance running/walking field tests in children aged 6 to 17 years, influence of weight status. NutriciÓn Hospitalaria 26(3), 572-578. [DOI] [PubMed] [Google Scholar]
- Cohen J. (1988) Statistical power analysis for the behavioral sciences, 2nd edition. Lawrence Erlbaum Associates, Hillsdale: 567. [Google Scholar]
- Cole T.J., Bellizzi M.C., Flegal K.M., Dietz W.H. (2000) Establishing a standard definition for child overweight and obesity worldwide, international survey. British Medical Journal 320, 1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole T.J., Faith M.S., Pietrobelli A., Heo M. (2005) What is the best measure of adiposity change in growing children: BMI, BMI%, BMI z-score or BMI centile? European Journal of Clinical Nutrition 59(3), 419-425. [DOI] [PubMed] [Google Scholar]
- Dellal A., Keller D., Carling C., Chaouachi A., Wong D.P., Chamani K. (2010) Physiologic effects of directional changes in intermittent exercise in soccer players. Journal of Strength and Conditioning Research 24(12), 3219-3226. [DOI] [PubMed] [Google Scholar]
- Ekkekakis P., Parfitt G., Petruzzello S.J. (2011) The pleasure and displeasure people feel when they exercise at different intensities. Sports Medicine 41(8), 641-671. [DOI] [PubMed] [Google Scholar]
- Eston R.G., Williams J.G. (1986) Exercise intensity and perceived exertion in adolescent boys. British Journal of Sports Medicine 20(1), 27-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox K.R., Corbin C.B. (1989) The Physical Self Perception Profile: Development and preliminary validation. Journal of Sport and Exercise Psychology 11, 408-430. [Google Scholar]
- Franklin J., Denyer G., Steinbeck K.S., Caterson I.D., Hill A.J. (2006) Obesity and risk of low self-esteem: A statewide survey of Australian children. Pediatrics 118(6), 2481-2487. [DOI] [PubMed] [Google Scholar]
- Goran M., Fields D.A., Hunter G.R., Herd S.L., Weinsier R.L. (2000) Total body fat does not influence maximal aerobic capacity. International Journal of Obesity and Related Metabolic Disorders 24, 841-848. [DOI] [PubMed] [Google Scholar]
- Groslambert A., Mahon A.D. (2006) Perceived exertion. Sports Medicine 36(11), 911-928. [DOI] [PubMed] [Google Scholar]
- Hatamoto Y., Yamada Y., Sagayama H., Higaki Y., Kiyonaga A., Tanaka H. (2014) The relationship between running velocity and the energy cost of turning during running. PlosOne 9 (1), e81850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hau K.T., Sung R.Y.T., Yu C.W., Marsh H.W., Lau P.W.C. (2005) Factorial structure and comparison between obese and non-obese Chinese children’s physical self-concept. The new frontiers of self research. Eds: Marsh H.W., Craven R., McInerney D.M. Information Age Charlotte, NC: 259-272. [Google Scholar]
- Howley E.T., Bassett D.R., Welch H.G. (1995) Criteria for maximal oxygen uptake, review and commentary. Medicine and Science in Sports and Exercise 27(9), 1292-1301. [PubMed] [Google Scholar]
- Jung M.E., Bourne J.E., Little J.P. (2014) Where Does HIT fit? An examination of the affective response to high-intensity intervals in comparison to continuous moderate- and continuous vigorous-intensity exercise in the exercise intensity-affect continuum. PlosOne 9 (12), e114541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klasson-Heggebø L., Andersen L.B., Wennlöf A.H., Sardinha L.B., Harro M., Froberg K., Anderssen S.A. (2006) Graded associations between cardiorespiratory fitness, fatness, and blood pressure in children and adolescents. British Journal of Sports Medicine 40(1), 25-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klijn P.H., van der Baan-Slootweg O.H., van Stel H.F. (2007) Aerobic exercise in adolescents with obesity: preliminary evaluation of a modular training program and the modified shuttle test. BMC Pediatrics 7(1), 7-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kyröläinen H., Santtila M., Nindl B. C., Vasankari T. (2010) Physical fitness profiles of young men. Sports Medicine, 40(11), 907-920. [DOI] [PubMed] [Google Scholar]
- Lau P. W., Wong D. P., Ngo J. K., Liang Y., Kim C. G., Kim H. S. (2015) Effects of high-intensity intermittent running exercise in overweight children. European Journal of Sport Science, 15(2), 182-190. [DOI] [PubMed] [Google Scholar]
- Léger L. A., Mercier D., Gadoury C., Lambert J. (1988) The multistage 20 metre shuttle run test for aerobic fitness. Journal of Sports Sciences 6(2), 93-101. [DOI] [PubMed] [Google Scholar]
- Liu N.Y.S., Plowman S.A., Looney M.A. (1992) The reliability and validity of the 20-meter shuttle test in American students 12 to 15 years old. Research Quarterly for Exercise and Sport 63(4), 360-365. [DOI] [PubMed] [Google Scholar]
- Maffeis C., Schutz Y., Schena F., Zaffanello M., Pinelli L. (1993) Energy expenditure during walking and running in obese and nonobese prepubertal children. The Journal of Pediatrics 123(2), 193-199. [DOI] [PubMed] [Google Scholar]
- Maïano C., Morin A.J.S., Mascret N. (2015) Psychometric properties of the short form of the Physical Self-Description Questionnaire in a French adolescent sample. Body Image 12, 89-97. [DOI] [PubMed] [Google Scholar]
- Marinov B., Kostianev S., Turnovska T. (2002) Ventilatory efficiency and rate of perceived exertion in obese and non-obese children performing standardized exercise. Clinical Physiology and Functional Imaging 22, 254-260. [DOI] [PubMed] [Google Scholar]
- Marsh H.W., Hau K.T., Sung R.Y.T., Yu C.W. (2007) Childhood obesity, gender, actual-ideal body image discrepancies, and physical self-concept in Hong Kong children, cultural differences in the value of moderation. Developmental Psychology 43(3), 647-662. [DOI] [PubMed] [Google Scholar]
- Marsh H.W., Martin A.J., Jackson S. (2010) Introducing a short version of the physical self description questionnaire: New strategies, short-form evaluative criteria, and applications of factor analyses. Journal of Sport and Exercise Psychology 32(4), 438-482. [DOI] [PubMed] [Google Scholar]
- Mercier C.S., Maïano C., Nicol C., Sepulcre J., Brisswalter J. (2010) Étude des relations entre les valeurs d’anxiété, d’estime globale de soi et la perception de l’effort lors de l’exercice physique chez des adolescentes obèses et non obèses [Relationship between anxiety, global self-esteem and perceived exertion values during exercise in obese and non-obese adolescent girls]. Science & Sports 25(6), 323-326. [Google Scholar]
- Norman G.R., Sloan J.A., Wyrwich K.W. (2003) Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Medical Care 41, 582-592. [DOI] [PubMed] [Google Scholar]
- Ninot G., Fortes M., Delignières D. (2001) A psychometric tool for the assessment of the dynamics of the physical self. European Review of Applied Psychology 51(3), 205-216. [Google Scholar]
- Ninot G., Fortes M., Delignières D., Maïano C. (2004) The dynamic adjustment of physical self in adults. Individual Differences Research 2(2), 137-151. [Google Scholar]
- Ninot G., Fortes M., Delignières D. (2006) Validation of a shortened assessment of physical self in adults. Perceptual and Motors Skills 103(2), 531-542. [DOI] [PubMed] [Google Scholar]
- Olds T., Tomkinson G., Léger L., Cazorla G. (2006) Worldwide variation in the performance of children and adolescents. An analysis of 109 studies of the 20-m shuttle run test in 37 countries. Journal of Sports Sciences 24(10), 1025-1038. [DOI] [PubMed] [Google Scholar]
- Paes S.T., Marins J.C.B., Andreazzi A.E. (2015) Metabolic effects of exercise on childhood obesity: a current view. Revista Paulista de Pediatria 33(1), 122-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peyrot N., Thivel D., Isacco L., Morin J.B., Duché P., Belli A. (2009) Do mechanical gait parameters explain the higher metabolic cost of walking in obese adolescents? Journal of Applied Physiology 106(6), 1763-1770. [DOI] [PubMed] [Google Scholar]
- Poortmans J.R., Boisseau N. (2003) Biochimie des activités physiques. 2nd edition. Brussels: De Boeck Supérieur; 143-147. [Google Scholar]
- Pyne D.B., Boston T., Martin D.T., Logan A. (2000) Evaluation of the Lactate Pro blood lactate analyser. European Journal of Applied Physiology 82(1-2), 112-116. [DOI] [PubMed] [Google Scholar]
- Quinart S., Mougin F., Simon-Rigaud M.L., Nicolet-Guénat M., Nègre V., Regnard J. (2014) Evaluation of cardiorespiratory fitness using three field tests in obese adolescents, validity, sensitivity and prediction of peak. Journal of Science and Medicine in Sport 17(5), 521-525. [DOI] [PubMed] [Google Scholar]
- Ratel S., Duché P., Williams C.A. (2006) Muscle fatigue during high-intensity exercise in children. Sports Medicine 36(12), 1031-1065. [DOI] [PubMed] [Google Scholar]
- Rey O., Rossi D., Nicol C., Mercier C. S., Vallier J-M., Maïano C. (2013) Évaluation indirecte de la capacité aérobie d’adolescents obèses : intérêt d’un test de course à pied intermittent court, progressif et maximal [Indirect assessment of aerobic capacity of obese adolescents; interest of a short, progressive and maximal intermittent running test]. Science & Sports 28(5), e133-e139. [Google Scholar]
- Shepherd S.O., Wilson O.J., Taylor A.S., ThØgersen-Ntoumani C., Adlan A.M., Wagenmakers A.J., Shaw C.S. (2015) Low-volume high-intensity interval training in a gym setting improves cardio-metabolic and psychological health. PlosOne 10 (9), e0139056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanaka H., Monahan K.D., Seals D.R. (2001) Age-predicted maximal heart rate revisited. Journal of the American College of Cardiology 37(1), 153-156. [DOI] [PubMed] [Google Scholar]
- Voss C., Sandercock G. (2009) Does the twenty meter shuttle-run test elicit maximal effort in 11- to 16-year-olds? Pediatric Exercise Science 21(1), 55-62. [DOI] [PubMed] [Google Scholar]