

Introduction
Schizophrenia is a severe psychotic disorder characteristically marked by a retreat from reality with delusion formation, hallucinations, emotional disharmony, and regressive behaviour. Affecting approximately 1% of the worldwide population and is associated with a high rate of morbidity and mortality. Studies suggest that genetics, early environment, neurobiology and psychological and social processes are important contributory factors. Family, twin, and adoption studies provided strong evidence of a genetic contribution to the aetiology of schizophrenia. However, attempts to isolating specific genes that confer vulnerability to the disorder have thus far been only moderately succesful. Schizophrenia is a condition of complex inheritance, with several genes possibly interacting to generate risk for schizophrenia. Schizophrenia is a chronic disease without remission and the treatment requires the use of antipsychotic drugs. Antipsychotics have a multitarget profile without a clear mechanism of action. The aims of pharmacogenetic investigations are the identification of genes influencing response, validation of targets, prediction of treatment response, prediction of side-effects, identification of patients likely to respond to a particular treatment, and the selection of most beneficial treatment according to genetic profile. Identification of drug-target mutations with a direct influence on treatment outcome would constitute evidence of specific mediators of drug activity (1). Currently available antipsychotic drugs achieve a certain degree of clinical improvement in the treatment of psychosis in about 50% of schizophrenia patients (1-3). Antipsychotic treatment failure has substantial clinical and economic costs. Delay in finding an adequate treatment for psychosis has a detrimental effect on patients prognosis’ and chances of recovery (4-5). These strong implications reinforce the need for pharmacogenetic research into factors affecting antipsychotic response and ways to predict clinical outcome.
Aim of study
The standardisation of methods to genotype three polymorphism (5HT2A 102 T/C, 5HTTLPR and rs25531) and two microsatellite markers (D1S2709 and D1S 2833), in order to study these polymorphisms in schizophrenia patients. A sample of 200 Spanish Caucasian first episode schizophrenia patients and a sample of 340 healthy control subjects matched for ethnic origin were used in the study. These patients were evaluated at baseline, and after 3, 6 and 12 months after the start of the treatment to assess treatment response.
Methods 1. Selection of polymorphisms
Polymorphisms were selected from previous reports which showed association with schizophrenia and treatment outcome.
1.1 Serotonin system
Alterations of the serotonergic system have been implicated in depression, anxiety, eating disorders and negative symptoms of schizophrenia. Antipsychotic drugs, specially the atypical antipsychotics, show affinity for serotonin (5-HT) neurotransmitter receptors and the most extensively studied have been the 5HT2A and 5-HT2C. Many reports have associated a silent 5HT2A 102-T/C polymorphism with the response to clozapine and risperidone. This polymorphism is in nearly complete linkage disequilibrium (LD) with a -1438-G/A promoter polymorphism in Caucasian populations (1,6,7,8). The selective serotonin reuptake inhibitors (SSRIs) are the most widely prescribed antidepressants worldwide. Despite recent advances in antidepressant pharmacotherapy, response rates are variable and can be low as 60 % for the first drug administered. The underlying mechanism for this variation is complex, involving both environmental and genetics factors and their interactions. One possible genetic mechanism involves the serotonin transporter gene (SLC6A4) which encodes the serotonin transporter (5-HTT) protein. This protein initiates the antidepressant effect of SSRIs, which are drugs that are thought to act primarily by terminating serotonin reuptake by the presynaptic serotonergic neuron. Genetic variations in 5-HTT-LPR polymorphism have been also found to be associated with variations in antipsychotic drug response (Arranz et al., 2000 (9). Most studies have focused on a single common polymorphism located in the promoter region of the SLC6A4. This insertion/deletion polymorphism, reported to be 43 bp in length, is commonly subdivided into S (short) and L (long) (10,11) alleles. The long allele has shown a higher protein transcription than the short allele (12). Recent reports have detected a single nucleotide polymorphism (SNP), rs25531 A>G, near the promoter region of the SLC6A4 (13). This SNP subdivided the previous S and L polymorphism into LA, SA, LG and SG.
1.2 Disrupted-in -Schizophrenia-1 (DISC 1)
Disrupted-in -Schizophrenia-1 (DISC-1) was identified as the sole gene in which a mutant truncation by a balanced traslocation (1; 11) (p42.1; q14.3) is cosegregated with schizophrenia in a large Scottish Family (14). The DISC1 locus has now been implicated by cytogenetics, linkage and association studies as a predisposing risk factor for neuropsychiatric illnesses, including schizophrenia, schizophrenia spectrum, bipolar, depression and autism spectrum disorders. Despite a few negative reports, the accumulating genetic evidence is strongly positive. We selected two microsatellite markers D1SC2709 and the D1S2833 which were found by Ekelund and colleagues. These two microsatellite markers in the DISC1 gene provided strong evidence for linkage to schizophrenia in a Finnish family (15,16).
2. Genotyping methods
2.1 Genotyping by RFLP of 5-HT2A 102-T/C and the 5-HTT LPR & 25531 polymorphisms
We standardised two polymerase chain reaction protocols followed by restriction fragment length polymorphism analyses (PCR-RFLP) for genotyping the 5-HT2A 102-T/C and the 5 HTT LPR & 25531 polymorphisms. DNA was amplified in 25uL containing 50 ng genomic DNA, 10mM dNTPs, 0.5 U of Taq polymerase, a final concentration of MgCl2 of 3mM for the 5-HT2A 102-T/C and 1 mM for the 5-HTT LPR & 25531.
Table 1 shows the final concentrations and the sequences of oligonucleotide primers for each polymorphism. Thermal cycling consisted of 35 cycles of 96 oC (35s), 60oC (60s) for the 5HT2A 102-T/C or 65.5oC (60s) for the 5-HTT LPR & 25531 and 72o (60s) each with a final extension step of 10 min at 72aC. Subsequently, 15 uL of PCR product were digested by Msp I at 37oC overnight. Finally the PCR and the digestion product were loaded onto an agarose gel and visualized by ethidium bromide (Table 1, Figure 1 and 2).
Table 1.
Description of the primers concentrations, sequences and PCR products.
| Polymorphism and oligonucleotide primer concentrations and sequences. | Amplicon and restritriction fragment lengths of alkks | |
|---|---|---|
| 5-HT2A 102-T/C 400 nM of F: 5′-tct gct aca agt tct ggc tt-3′ 400 nM of R: 5′-ctg cag ctt ttt ctc tag gg-3′ |
PCR product | MSp I |
| 372bp | T-372bp C-156+216bp |
|
| 5-HTT LPR & 25531 200 nM of F:5′-tcctccgctttggcgcctcttcc- 3′ 200 nM of R: 5′-tgggggttgcaggggagatcctg- 3′ |
S-469bp L-512bp |
SA-469 bp SG-402 + 67 bp LA-512 bp LO-402 + 110 bp |
| Microsatellite of the DISC1 | ||
| Oligonucleotide primer concentrations and sequences | PCR product | |
| DIS 2709 200nM of F: 5′FAM-tcataccatatca gaatgtc- 3′ 200nM of R: 5′-atcaatcagtatctaatagcatca- 3′ |
191-197 bp | |
| DIS 2833 150nM of F: 5′-FAM-tttgggggtaatttgttacatagc c- 3′ 150nM of R: 5′ ttc tga gcc cca gat tga cac tg 3′ |
128-146 bp | |
Figure 1.
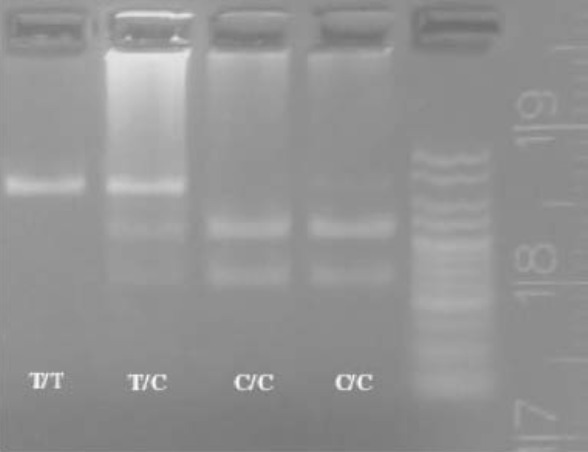
PCR product of the 5-HT2A 102-T/C. The picture shows the three possibles genotypes T/T,T/C and C/C.
Figure 2.

5-HTT LPR & 25531 genotype. The first lane of each individual represent the PCR product, and the second one, the digestion product.
2.2 Automatic genotyping of D1S2709 and D1S2833 microsatellites
DNA was amplified in 25uL containing 2ng genomic DNA, 10mM dNTPs, 0.5 U of Taq polymerase, a final concentration of MgCl2 of 2mM for the D1S 2709 and 1mM for the D1S 2833. Thermal cycling consisted of 35 cycles of 96oC (35s), 60oC(60s) for the D1S 2709 or 63oC (60s) for the D1S 2833 and 72oC (60s) each with a final extension step of 10 min at 72oC. The primer sequences and concentrations are shown in Table 1. Subsequently, the length of the PCR product was analyzed in the ABI prism® 3100 by capillary electrophoresis. Our electrophoregrams results showed a microsatellite size range between 191-197 bp for the D1S2709 and 128-146 bp for the D1S2833.
Results
Atthe moment we have the results of the genotyping of 5-HT2A 102-T/C and the 5-HTT LPR & 25531 polymorphisms in controls and patients. However, we only have the first results for the DISC1 microsatellite genotyping and more tests should be carried out. Now we have to check the sequence of the microsatellite polymorphism in order to identify the true length of the allele between the stutter products. The aim is to know the allele frequencies of these polymorphisms in our population and to study the association between each polymorphism and the treatment response. For this study we are going to use statistical analyses of frequency distribution and haplotype combinations.
Conclusion
Pharmacogenetics findings constitute a clear advance towards a future tailoring of antipsychotic treatment to individual needs. However, further development of the field can be obtained by the application of pharmacogenomic strategies to the identification of novel factors influencing response.
Acknowledgements
I would like to thank the IFCC (International Federation of Clinical Chemistry and Laboratory Medicine) for its support and the SEQC (Spanish Society of Clinical Biochemistry and Molecular Pathology). I am also grateful to all the staff of the Section of Clinical Neuropharmacology at the Institute of Psychiatry in London, specially Dr. María Jesús Arranz.
References
- 1.Arranz MJ, de Leon J. Pharmacogenetics and pharmacogenomics of schizophrenia: a review of last decade of research. Mol Psychiatry. 2007. Aug;12(8):707-747. [DOI] [PubMed] [Google Scholar]
- 2.Miyamoto S, Duncan GE, Marx CE, Lieberman JA. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005. Jan;10(1):79-104. [DOI] [PubMed] [Google Scholar]
- 3.Kerwin RW, Osborne S. Antipsychotic drugs. Medicine 2000; 28: 23-25. [Google Scholar]
- 4.Perkins DO, Gu H, Boteva K, Lieberman JA. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: a critical review and meta-analysis. Am J Psychiatry. 2005. Oct;162(10):1785-1804. [DOI] [PubMed] [Google Scholar]
- 5.Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, Keefe RS, Davis SM, Davis CE, Lebowitz BD, Severe J, Hsiao JK; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005. Sep 22;353(12):1209-1223. [DOI] [PubMed] [Google Scholar]
- 6.Arranz MJ, Munro J, Sham P, Kirov G, Murray RM, Collier DA, Kerwin RW. Meta-analysis of studies on genetic variation in 5-HT2A receptors and clozapine response. Schizophr Res. 1998. Jul 27;32(2):93-99. [DOI] [PubMed] [Google Scholar]
- 7.Arranz MJ, Munro J, Owen MJ, Spurlock G, Sham PC, Zhao J, Kirov G, Collier DA, Kerwin RW. Evidence for association between polymorphisms in the promoter and coding regions of the 5-HT2A receptor gene and response to clozapine. Mol Psychiatry. 1998. Jan;3(1):61-66. [DOI] [PubMed] [Google Scholar]
- 8.Lane HY, Chang YC, Chiu CC, Chen ML, Hsieh MH, Chang WH. Association of risperidone treatment response with a polymorphism in the 5-HT(2A) receptor gene. Am J Psychiatry. 2002. Sep;159(9):1593-1595. [DOI] [PubMed] [Google Scholar]
- 9.Arranz MJ, Bolonna AA, Munro J, Curtis CJ, Collier DA, Kerwin RW. 2000. The serotonin transporter and Clozapine response. Molecular Psychiatry 5:124-130. [DOI] [PubMed] [Google Scholar]
- 10.Serretti A. Artioli. Pharmacogennomics J 2004; 4: 233-244. [DOI] [PubMed] [Google Scholar]
- 11.Murphy DL, Lerner A, Rudnick G, Lesch KP. Serotonin transporter: gene, genetic disorders, and pharmacogenetics. Mol Interv. 2004. Apr;4(2):109-123 [DOI] [PubMed] [Google Scholar]
- 12.Lesch KP, Balling U, Gross J, Strauss K, Wolozin BL, Murphy DL, Riederer P. Organization of the human serotonin transporter gene. J Neural Transm Gen Sect. 1994;95(2):157-162 [DOI] [PubMed] [Google Scholar]
- 13.Kraft JB, Peters EJ, Slager SL, Jenkins GD, Reinalda MS, McGrath PJ, Hamilton SP. Analysis of association between the serotonin transporter and antidepressant response in a large clinical sample. Biol Psychiatry. 2007. Mar 15;61(6):734-742. [DOI] [PubMed] [Google Scholar]
- 14.Millar JK, James R, Christie S, Taylor MS, Devon RS, Hogg G, et al. Functional characterisation of DISC 1, a candidate susceptibility gene for major psychiatric illness. Am J Med Genet 2002; 114: 748. [Google Scholar]
- 15.Ekelund J, Lichtermann D, Hovatta I, Ellonen P, Suvisaari J, Terwilliger JD, et al. Genome-wide scan for schizophrenia in the Finnish population: evidence for a locus on chromosome 7q22. Hum Mol Genet. 2000. Apr 12;9(7):1049-1057. [DOI] [PubMed] [Google Scholar]
- 16.Ekelund J, Hovatta I, Parker A, Paunio T, Varilo T, Martin R, et al. Chromosome 1 loci in Finnish schizophrenia families. Hum Mol Genet. 2001. Jul 15;10(15):1611-1617. [DOI] [PubMed] [Google Scholar]