

Abstract
Mass casualty decontamination is a public health intervention that would be employed by emergency responders following a chemical, biological, or radiological incident. The decontamination of large numbers of casualties is currently most often performed with water to remove contaminants from the skin surface. An online survey was conducted to explore US fire departments' decontamination practices and their preparedness for responding to incidents involving mass casualty decontamination. Survey respondents were asked to provide details of various aspects of their decontamination procedures, including expected response times to reach casualties, disrobing procedures, approaches to decontamination, characteristics of the decontamination showering process, provision for special populations, and any actions taken following decontamination. The aim of the survey was to identify any differences in the way in which decontamination guidance is implemented across US states. Results revealed that, in line with current guidance, many US fire departments routinely use the “ladder-pipe system” for conducting rapid, gross decontamination of casualties. The survey revealed significant variability in ladder-pipe construction, such as the position and number of fire hoses used. There was also variability in decontamination characteristics, such as water temperature and water pressure, detergent use, and shower duration. The results presented here provide important insights into the ways in which implementation of decontamination guidance can vary between US states. These inconsistencies are thought to reflect established perceived best practices and local adaptation of response plans to address practical and logistical constraints. These outcomes highlight the need for evidence-based national guidelines for conducting mass casualty decontamination.
Mass casualty decontamination would be employed by emergency responders following a chemical, biological, or radiological incident. An online survey was conducted to explore US fire departments’ decontamination practices and their preparedness for responding to such incidents. Respondents were asked to provide details of their decontamination procedures, including expected response times to reach casualties, disrobing procedures, approaches to decontamination, characteristics of the showering process, provision for special populations, and any actions taken following decontamination. The results provide important insights into the ways implementation of guidance can vary between US states.
The use of chemical, biological, radiological, and nuclear (CBRN) material and weapons remains a global threat.1,2 Because of the adverse health consequences of chemical incidents, the US government considers both deliberate and accidental release to be a serious threat to public health.3,4 National or regional guidelines are in place in the United States and many other countries for responding to mass casualty incidents arising from exposure to CBRN materials.3,5,6
One of the main interventions for reducing the risk posed by CBRN agents is decontamination. The aim of decontamination is to remove as much contaminant from the skin as possible, in order to prevent or minimize adverse health effects and to reduce the risk of secondary contamination of other people and places. Decontamination can involve various steps, including disrobing, showering with water, or dry decontamination with absorbent materials. While decontamination may be used in response to incidents involving biological and radiological materials, it is likely to be of most benefit during incidents involving chemical agents, since this type of exposure may be overt (it is immediately obvious that a release has occurred) and an immediate response is necessary in order to minimize injury and save lives.7 Mass decontamination is described as “the emergency removal of contamination quickly from large numbers of victims.”8(p172)
Although there are gaps in the research literature to date, evidence suggests that rapid physical removal of a hazardous agent is the most important aspect of decontamination.1,9 The act of disrobing has been shown to be a highly effective method for removing hazardous chemical contaminants from casualties and should be implemented at the earliest opportunity during incidents involving chemical agents.7,10 For incidents involving biological and radiological materials, a “wet strip flush” approach may be more effective, but the current survey focuses on response to chemical incidents, for which disrobing prior to showering has been shown to be most effective.7 It is important that casualties disrobe prior to showering, as failure to do so could facilitate increased transfer of any contaminant to the skin.7
Disrobing should then be followed by gross decontamination, which is the use of standard equipment to provide a rapid yet structured decontamination process for large numbers of people. One recommended method for conducting gross decontamination is the “ladder-pipe system” (LPS). Ladder-pipe system decontamination involves positioning ladders and hoses from 2 or more fire tenders to create a shower corridor through which contaminated casualties are moved (see Figure 1).11 Guidance recommends that water in this shower corridor be delivered in high volume but at relatively low pressures. Further, guidance recommends that instructions to casualties include the instruction to walk slowly through the corridor with their heads held back and arms extended and to turn around in the center of the corridor.12 Ladder-pipe system decontamination may then be followed by secondary or technical decontamination in specialized mass decontamination units. The decision as to whether or not to carry out secondary decontamination will usually depend on the type and extent of contamination.12
Figure 1.

Image of a Typical Ladder-Pipe System Decontamination Corridor.
Recent research involving specialized mass decontamination units has examined how various characteristics of the showering process can contribute to the effectiveness of decontamination. Findings show that in mass decontamination units, the optimal duration for shower-based decontamination is between 60 and 90 seconds, and the recommended water temperature for decontamination is 35°C (95°F).13,14 The use of detergent removes about 40% more contamination than water alone7,15 and is recommended to optimize shower-based decontamination.3,7,12,16-19 However, while research has examined the effectiveness of different showering characteristics using mass decontamination units, methods of gross decontamination have not undergone formal testing. In the conduct of gross decontamination, current guidance recommends that a high volume of water be delivered at a minimum of 60 pounds per square inch (psi) (4.14 bar) to ensure that hazardous agents are removed.11 Weather may affect the behavior of a toxic agent and will therefore have an impact on decontamination requirements. For example, strong wind, heavy rain, or temperatures below freezing may reduce the effects of a chemical agent.8 Decontamination during cold or adverse weather may also increase the risk of hypothermia, particularly for vulnerable groups such as older people, young children, and people with existing health conditions, and the decontamination process may need to be adapted accordingly—for example, implementing dry instead of wet decontamination and quickly providing casualties with temporary clothing and a place to shelter, in order to provide warmth and to address modesty concerns.3,12
The needs of a diverse population, and in particular vulnerable groups, must be considered during the decontamination process. Following the attacks of September 11, 2001, the National Organisation on Disability launched the Emergency Preparedness Initiative to ensure that emergency managers and first responders address disability concerns and that people with disabilities are included in all levels of emergency planning, response, and recovery.20 Guidance suggests that those with disabilities be allowed to retain any equipment that enables them to maintain independence and self-control.3 Further, recent research has suggested that emergency responders can look to casualties to support each other and to take key actions such as moving away from the source of contamination and initiating self-care decontamination procedures, helping those around them to do the same.20,21
An effective communication strategy is needed to convey the importance of these steps as emergency responders help to manage contaminated casualties.22,23 Guidance states that it may be challenging to communicate decontamination procedures with casualties who are non–English speaking or who have limited English proficiency (LEP).18,19,24 Research suggests that individuals who are non–English speaking or who have limited English proficiency are unlikely to follow instructions during a mass casualty event, possibly because they may have lower confidence in the communication they receive regarding appropriate actions to take.25 Guidance recommends that interpreters be included in the decontamination team and that emergency responders be fully trained to assist those who are non–English speaking and who have limited English proficiency.19,24
This study explored decontamination practices and preparedness for chemical incidents in US fire departments via an online survey, in order to explore regional variations and consistency with current evidence and guidance for mass casualty decontamination. Survey questions related to: the response time to reach contaminated casualties, approaches to disrobing, the characteristics of the decontamination showering process, provision for vulnerable groups, and the management of casualties post-decontamination (see supplementary information at www.libertonline.com/hs for full survey). The study informed an ongoing collaborative research program conducted by the University of Hertfordshire and Public Health England (PHE) on behalf of the US Department of Health and Human Services' (HHS) Biomedical Advanced Research and Development Authority (BARDA), which seeks to develop the evidence base for effective emergency decontamination procedures.
Methods
Survey Design
A 31-question online survey was created by researchers at Public Health England and the University of Hertfordshire. The survey was conducted using SelectSurvey.Net, hosted on PHE servers in the UK. This allowed data to be stored in accordance with the UK Data Protection Act 1998. As the survey was designed to capture information about current emergency decontamination practices, the survey was considered a form of service evaluation and therefore not subject to research ethics approval. This position was confirmed by the PHE Research and Development Office.
Survey questions were designed to ensure clarity and brevity and to avoid ambiguity to achieve good practice in survey design. A combination of closed, multiple-response, and open-ended response questions were used to address a range of questions. Multiple-response option questions were presented in a grid format, with the order of questions randomized in each grid to prevent response item ordering bias. Page conditions were used so that if, for example, a respondent reported that casualties would not be disrobed prior to decontamination, they would be directed to a subsequent set of questions and would not have to answer questions about predecontamination disrobing. Respondents were able to skip questions if they had insufficient information to respond.
Survey respondents were asked to report their level of experience concerning mass decontamination, including whether they had ever been involved in a CBRN incident, the number of real-life incidents they had been involved in, and the occurrence and frequency of emergency preparedness drills and exercises in their locality. Three questions were asked to identify the decontamination approach used by their fire department, the hose configurations they would use for ladder-pipe system decontamination, and the procedures they would use during cold weather. Two questions addressed the act of disrobing casualties during an incident response. The survey asked 5 specific questions about the decontamination showering process, which related to the temperature of the water, the water pressure (in psi), the duration of showering, whether detergent would be routinely added to shower water, and whether casualties would walk through the decontamination corridor alone or in groups. Further questions in the survey sought to collect data in key areas including the response time to reach contaminated casualties and the provision for vulnerable populations during mass decontamination. The full set of survey questions can be seen in the supplementary material accompanying this article.
Participants and Procedure
A cover letter with a link to the online survey was circulated to members of the US InterAgency Board (IAB). The IAB is “… a voluntary collaborative panel of emergency preparedness and response practitioners from a wide array of professional disciplines that represent all levels of government and the voluntary sector.”26 The cover letter explained the purpose of the study and invited recipients to take part in the survey.
Additional emergency responders were identified using snowball sampling, a nonprobability sampling technique in which respondents are asked to assist researchers in identifying other potential participants. The cover letter and survey link requested that IAB members circulate the survey to other colleagues among the emergency response community. Respondents were provided with PHE contact details should they have any further questions about the survey. Informed consent from survey respondents was collected via a question on the first screen of the survey, following an introduction to the aims of the survey, the time commitment involved, and information on the way in which respondents' information would be processed and stored.
Results
The survey elicited a relatively low response. A total of 68 emergency response professionals responded to the survey, but only 42 completed the survey, with 26 skipping 1 or more questions. Of the 68 participants, 49 identified their location (see Figure 2), with at least 1 response coming from each of 21 different US states. In all, 34 participants identified the city in which their fire department was located; according to the 2010 US Census,27 31 of these cities are classified as urban areas (≥50,000 people), while 3 are classified as urban cluster areas (at least 2,500 and fewer than 50,000 people). Fifty-two survey respondents disclosed their emergency response role, with responses indicating varying levels of experience in emergency preparedness and response. Eleven respondents indicated that they were directly involved in decontamination, CBRN, and/or hazmat at an operational level. Two respondents reported that they were responsible for producing guidance on the subject. Almost half of the respondents who completed the survey (n = 23) held leadership positions at the senior level, such as director or chief. Overall, respondents' job roles indicated that they were well qualified to describe the emergency response procedures in their locality.
Figure 2.

Locations of Emergency Response Professionals Who Responded to the Survey.
Response Time
Twenty-five respondents estimated the time between receiving a 911 call and the arrival of fire tenders at the incident scene. The estimated response times during peak traffic ranged from 3 to 15 minutes (mean response time [M] = 8.01 minutes), while the estimated response times during non-peak traffic ranged from 3 to 12 minutes (M = 5.36 minutes). Twenty respondents estimated the time between arrival of fire tenders at the scene and the start of emergency decontamination. The estimated time between arrival of fire engines and decontamination of the first casualty ranged from 20 seconds to 20 minutes (M = 5.65 minutes), with 5 of 20 respondents providing estimates of 2 minutes or less. Twenty-eight respondents estimated the time allowed between disrobing and beginning emergency decontamination, with times ranging from 0 to 60 minutes (M = 6.29 minutes).
Removal of Contaminated Clothing
The majority of respondents (64%) reported that, in a real incident involving a chemical contaminant, casualties would be instructed to disrobe prior to showering (see Figure 3). Respondents were asked to specify at what point during the decontamination process they would ask casualties to disrobe. This open-ended question revealed that nearly half of the respondents (13/28) said that casualties would be asked to disrobe immediately. Other responses included: “response would be situation/incident dependent” (n = 11); “casualties would be instructed to disrobe after gross decontamination” (n = 3); and “unsure” (n = 1).
Figure 3.
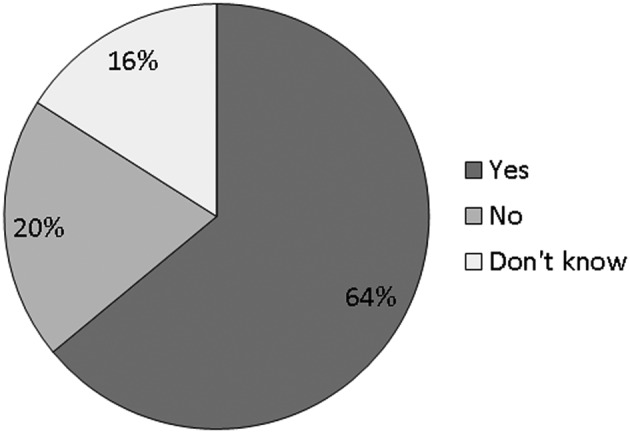
Percentage of Responders Who Would Ask Casualties to Disrobe Before Showering.
Respondents were asked what they would do if casualties were unwilling to disrobe. The question allowed respondents to select more than 1 option from several strategies; responses are presented in Table 1. The most commonly selected procedure (n = 18) was to “offer a privacy corridor.” The 7 respondents who selected “other” were asked to specify the alternative strategies they would use, with responses including “several of the above,” “situational,” and “separated into a different refuge area (control until decontamination can be metered or quality assurance measures are verified).”
Table 1.
If casualties are unwilling to disrobe, how would you respond?
| Procedure | No. of Times Selected |
|---|---|
| Allow casualties to proceed through the decontamination procedure fully clothed | 14 |
| Refuse to decontaminate until they disrobe | 1 |
| Explain the importance of disrobing in order to encourage them to disrobe | 15 |
| Offer a “privacy corridor” | 18 |
| Other | 7 |
Note. Respondents could select as many options as applicable.
Methods of Decontamination
Thirty-six of 51 respondents confirmed that the ladder-pipe system is the preferred approach for decontaminating multiple casualties affected by a chemical incident. A number of different or additional approaches were reported including “technical decontamination,” “reactive skin decontamination lotion (RSDL),” “multiple decontamination shower tents,” and “outdoor plumbing and fixtures around military hospitals to quickly set up mass decontamination lines for community and military support.”
Characteristics of the Ladder-Pipe System
Respondents were asked to describe the hose and nozzle arrangement employed during ladder-pipe system decontamination and to provide details about water temperature and pressure used, shower duration, and instructions provided to affected casualties. Twenty-five of the 36 respondents who used the ladder-pipe system approach answered these questions.
Configuration of Hoses and Nozzles
Respondents were asked to specify the configuration of hoses and nozzles they would use to carry out the ladder-pipe system. The questions in this section allowed respondents to select more than 1 option from several strategies. The most common response reported by 19 of the 25 respondents was the use of 3 positions: hoses mounted to fire tenders either side of the decontamination corridor and overhead hoses. Two respondents indicated that only side mounted hoses were used, while 7 respondents stated that some other configuration was used. Respondents reported a variety of different brands and types of shower nozzles used at each hose position, including Turbo Master, Hy-D, Akron Fog Nozzles, and Task Force Tips.
Control of Water Temperature
The majority of the respondents (20/25, 80%) said they were unable to control the temperature of the shower water. Only 2 respondents (8%) stated that temperature control was possible (see Figure 4). The respondents who said they were unable to control the water temperature were asked the approximate hydrant temperature on the coldest and hottest days of the year. Ten respondents estimated the hydrant temperature on the coldest and hottest days of the year, with temperatures ranging from 30 to 76°F (−1.1 to 24.4°C) for the coldest day and 50 to 79°F (10 to 26.1°C) for the hottest day.
Figure 4.
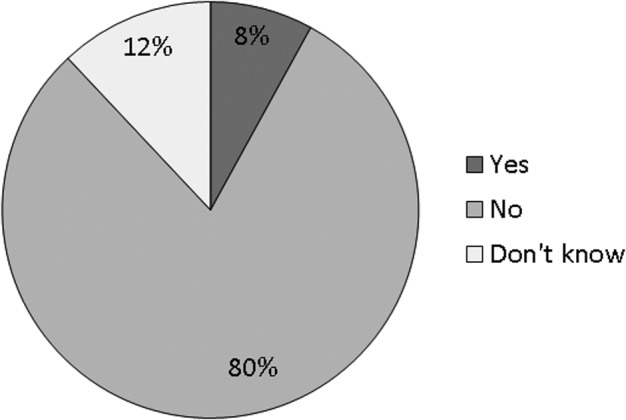
Percentage of Responders Who Stated that They Would Not Be Able to Control the Temperature of the Shower Water.
Water Pressure
The respondents were asked to estimate the water pressure used to decontaminate casualties. Ten of 25 respondents estimated the water pressure used, with responses ranging from 30 to 150 psi (M = 66 psi) (2.07 to 10.3 bar [M = 4.6 bar]). Factors influencing decisions about water pressure included satisfactory spray pattern, corridor length, and adequate “fog.” Nine respondents did not know the water pressure used for decontamination.
Shower Duration
The respondents were asked to specify how long they would let casualties spend in the shower. Twenty of the 25 respondents (80%) gave numerical estimations of the duration of decontamination, ranging from 5 to 10 seconds to 10 minutes, with half of the respondents stating that shower duration would be between 30 and 60 seconds (10/20, 50%). A further 4 respondents (20%) stated that shower duration would be 2 minutes; 3 respondents (15%) greater than 5 minutes (5 to 10 minutes); and 3 respondents (15%) stated that shower duration would be less than 30 seconds (5 to 20 secs).
Detergent Use
Eleven of 25 respondents (44%) stated that they were unable to add detergent to the water dispensed from the fire hoses during ladder-pipe decontamination. A comparable 10 respondents (40%) said that they were able to carry out this process. Four respondents (16%) selected “don't know” (see Figure 5). Follow-up questions explored the type and concentration of detergents, if used. Only 3 respondents referenced specific brands (Dawn, n = 2; Johnson's Baby Shampoo, n = 1), while 4 respondents provided generic information such as “Class A foams” and “dish soap.” No indication of the concentration of detergent used was provided.
Figure 5.
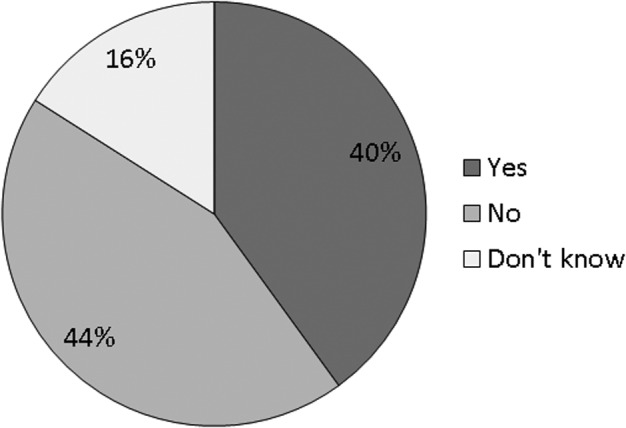
Percentage of Responders Who Stated that They Would Be Able to Add Detergent During Decontamination.
Cold Weather Considerations
Eleven of 25 respondents confirmed that they would employ ladder-pipe system decontamination even under cold weather conditions. Fifteen of 25 respondents identified other measures, including “using tents with warm air and a warm water supply,” “dry decontamination,” “providing protection from the cold environment,” and “using nearby facilities such as nearby building lobbies.”
Management of Casualties
Nineteen of 25 respondents (76%) reported that they have no fixed rules for how casualties would walk through the shower corridor. Five respondents (20%) reported that casualties would walk through the shower individually, and 1 respondent (4%) reported that they didn't know whether casualties would be asked to walk through the process individually or in groups. Eight out of 25 respondents (32%) reported that they would use a bullhorn or other type of public address system to direct casualties through the decontamination process. Seven respondents (28%) gave details of the instructions they would provide to casualties during the decontamination process. The most commonly reported instructions included asking casualties to walk slowly through the decontamination corridor, extend arms, and turn occasionally.
Provision for Vulnerable Groups
Survey respondents were asked to elaborate on their procedures for managing casualties with additional or special needs during mass decontamination, specifically during disrobing and re-robing. Groups who may have special needs during decontamination include those with mental or physical health conditions, children, nonambulatory casualties, and those who require supportive aids such as wheelchairs, prosthetic limbs, and assistance animals. Respondents were asked how they would manage groups who are unable to undress and re-dress themselves because of physical and/or mental health conditions (see Table 2). The most commonly selected approach was to “have a member of their team disrobe them and re-robe them at the other end” (n = 21). Those who selected “other” (n = 8) were asked to specify the approach they used. Responses included: “depends on the situation,” “any of the above may be applicable,” “male and female hazardous materials technicians are available inside the decontamination tent to assist,” and “generate a by-pass lane or privacy corridor and/or tarp the tent interior to create support space.”
Table 2.
How do you manage groups who are unable to undress/re-dress themselves due to physical and/or mental health conditions?
| Procedure | No. of Times Selected |
|---|---|
| Allow them to proceed through the decontamination procedure fully clothed | 11 |
| Have a member of your team disrobe them and re-robe them at the other end | 21 |
| Request help from an able-bodied casualty to assist with the disrobe process | 12 |
| Other | 8 |
Note. Respondents could select as many options as applicable.
Respondents were asked if parents or guardians were allowed to carry young children through the decontamination shower. Of 48 responses to this question, 41 respondents stated that parents would be allowed to carry young children through decontamination, with only 2 respondents suggesting that this is not permitted. In addition, respondents were asked to identify their procedures for managing casualties who are unable to walk (nonambulatory) during decontamination (see Table 3). The most common option was: “allocate a designated decontamination area and crew specifically to deal with nonambulatory casualties” (n = 34). Other responses included: “dependent on agent,” “level of exposure,” “onset of symptoms,” “available staff,” “number of casualties requiring decontamination,” “ask victims to assist and provide extra time in the decontamination shower area for the group to reduce contamination as much as possible for all involved,” and “assist nonambulatory casualties with responders in PPE [personal protective equipment].” When asked if they would allow those with physical impairments to take supportive aids through the decontamination procedure, the majority of respondents indicated that guide dogs (74%), walking sticks (79%), wheelchairs (74%), prosthetic limbs (79%), and glasses (84%) were all permitted to pass through decontamination with casualties.
Table 3.
What would you do if presented with casualties who are unable to walk (nonambulatory) during the decontamination procedure?
| Procedure | No. of Times Selected |
|---|---|
| Prioritize the decontamination of ambulatory over nonambulatory casualties | 12 |
| Allocate a designated decontamination area and crew specifically to deal with nonambulatory casualties | 34 |
| Send nonambulatory casualties to hospital without decontamination | 2 |
| Other | 11 |
Note. Respondents could select as many options as applicable.
Postdecontamination Care
The majority of respondents (22/28, 79%) would provide temporary clothing packs to casualties following emergency decontamination. Only 4 respondents (14%) said no, while the remaining 2 respondents (7%) said they did not know. When asked whether the emergency department of a local hospital would be prepared to accept casualties who had undergone only ladder-pipe system decontamination, 16 of 25 respondents (64%) answered yes. However, 7 respondents (28%) said the emergency department would be prepared to accept casualties “only after more thorough/technical decontamination.” Two respondents (8%) said they did not know.
Discussion
The online survey presented in this article describes a cross-section of current decontamination practices and preparedness for chemical incidents across 21 different US states. Responses to the survey indicate that decontamination practices differ substantially, suggesting that current protocols are not always consistent with current evidence and best-practice guidance. The survey focused on a number of different aspects of mass decontamination: response time to reach contaminated casualties, approaches to disrobing and decontamination, characteristics of the decontamination showering process, and provision for special populations.
Response Time
All respondents reported that they would reach contaminated casualties within 15 minutes of receiving a 911 call and that response times could be as little as 3 minutes. However, there was wide variability in the length of time between fire tenders arriving at the scene and the first casualty being decontaminated, with estimations ranging between 20 seconds and 20 minutes. This emphasizes the need to quickly initiate disrobing of casualties, as this is an effective step that can be taken soon after emergency responders arrive at the incident scene.7 It may be that the respondents assumed that the decision to decontaminate would already have been made in this scenario, and they may also have made the assumption that initial decontamination could be conducted with on-vehicle water reservoirs and hoses, rather than with a full ladder-pipe system configuration in place. However, this is speculative, so we acknowledge that these times might be unrealistic, and further investigation is required.
Approaches to Disrobing and Decontamination
Most of the respondents stated that they would ask casualties to disrobe prior to showering, with just over half stating that they would ask casualties to disrobe as soon as possible. However, a proportion of respondents stated that they would not ask casualties to disrobe prior to showering. Disrobing has been shown to be one of the most effective steps to reduce exposure to a contaminant, and to maximize this protective effect, disrobing should occur as soon as possible following possible contamination.10 While a large number of respondents acknowledged the importance of rapid disrobing, this was not universally recognized.
When asked what actions they would take if casualties were unwilling to disrobe, most respondents stated that they would either offer a privacy corridor or provide further explanation about the benefits of disrobing (or both). However, half of the respondents stated that they would allow casualties to proceed through the decontamination process fully clothed. Allowing casualties to undergo decontamination while fully clothed could increase the transfer of contaminants through the clothing, leading to greater contamination of the skin.7
The majority of respondents stated that they would employ the ladder-pipe system method of decontamination, as recommended in current guidance.3,11,12 The most common hose configuration for the ladder-pipe system was to use hoses mounted to the side of fire tenders, as well as a hose suspended from a ladder attached to an aerial truck. The type of nozzle attachments generating the shower spray was shown to vary among respondents, with no clear indication of preferred models or spray pattern. The majority of respondents recognized that it might be necessary to adapt ladder-pipe system decontamination systems during cold weather, with suggested adaptations including using tents with warm air and warm water, or carrying out dry decontamination instead. However, some respondents stated that they would carry out the same method of decontamination during cold or adverse weather. Current guidance suggests that, in cold environments, it might be necessary to avoid water-based decontamination, to minimize the likelihood of cold weather injuries.3 This is particularly the case when decontaminating vulnerable groups, such as older adults or children, who are at increased risk of adverse effects from the cold.
Decontamination Showering Process
The majority of respondents stated that they were unable to control the temperature of the water used for decontamination. There were a wide range of different water pressures reportedly used for decontamination, but over half of the respondents were unclear as to the pressure employed. Approximately a quarter of respondents stated that the pressure they would use would be around or below 60 psi (4.14 bar), the minimum recommended water pressure for decontamination.11 The majority of participants (14 of 25) were either unable to add detergent to the water dispensed from fire hoses or did not know if this was possible and were therefore unable to follow the recommendation of decontaminating casualties using detergent.3,16-19 Only 3 respondents made reference to specific brands of detergent appropriate for the decontamination of casualties, and no indication of the concentration of detergent used was provided. Respondents reported a wide range in shower duration, ranging from 5 seconds to 10 minutes. Half of respondents reported that shower duration would be between 30 and 60 seconds, below the recommended shower duration of 60 to 90 seconds identified in controlled studies of emergency decontamination.13,14
Only a quarter of respondents reported that they would provide instructions to casualties about how to progress through the decontamination process. Where details of specific instructions were given, these included asking participants to walk slowly through the decontamination corridor, turn occasionally, and extend arms; these instructions were therefore broadly in line with current guidance, based on perceived best practice.12 However, research into the effectiveness of showering in mass decontamination units suggests that active washing will be important.14
Providing for Vulnerable Populations
When asked how they would manage the decontamination of casualties who were unable to undress or re-dress themselves because of physical or mental health conditions, the majority of respondents stated that they would ask a member of their team to help the casualty to disrobe and re-robe. This was the most common way to manage nonambulatory casualties through the decontamination process. However, depending on the number of casualties with additional needs, these actions could strain responder resources and may not be practical.
Another option selected by respondents was to ask an able-bodied casualty to help other casualties to disrobe and re-robe. Recent research suggests that casualties may be willing to help others during decontamination, provided they have received practical, health-focused information from emergency responders concerning the importance of undergoing decontamination.21-23
Guidance states that the decontamination team should include interpreters in order to assist casualties who are non–English speaking or who have limited English proficiency.19,24 The survey did not ask questions specifically related to communication with non–English speaking casualties; further work is needed to explore the management of this vulnerable group during mass decontamination. The survey questions relating to vulnerable groups also did not distinguish between casualties who were nonambulatory due to preexisting conditions and casualties who had become nonambulatory as a result of the incident. It is likely that emergency responders might choose to manage these 2 groups differently, and this is therefore an aspect that requires further study.
The majority of respondents stated that they would allow various different types of service equipment, including guide dogs, walking sticks, wheelchairs, prosthetic limbs, and glasses, to be taken through the decontamination shower; this is in line with recommendations in decontamination guidance.3 Only a small minority stated that they would not allow this equipment to go through the decontamination shower. While allowing service equipment to be taken through the shower is likely to enable casualties to progress through decontamination more independently, consideration should be given to equipment that cannot go through the showering process (eg, some types of prosthetic limbs). In such cases, casualties should be decontaminated as nonambulatory casualties.3
Implications
Reported decontamination procedures varied substantially among different survey respondents. In certain aspects, such as initiating disrobing as quickly as possible, employing a ladder-pipe system method of decontamination, and providing re-robe packs to casualties following decontamination, responses were broadly in line with guidance and evidence for decontamination practices. However, in several aspects of decontamination, most notably characteristics of the decontamination shower (shower duration, shower temperature, and shower pressure), responses varied and were often not consistent with current guidance. Failure to adhere to recommended decontamination processes could result in casualties receiving less than effective decontamination and possibly experiencing more adverse effects or injury.
The variability in the responses presented here may be a result of the fact that there are several national guidance documents for mass decontamination that are not always consistent with each other. Some of these guidance documents are based on evidence from research, while others are based on perceived best practice. The findings from the survey reported here therefore suggest that there is a need to ensure that decontamination guidance documents are consistent across US states and updated routinely with the developing evidence base in this area.
Study Limitations
There are 2 main limitations to this study. First, snowball sampling was used to reach respondents; this method is dependent on participants forwarding the survey on to others. The population of interest was emergency response personnel with either experience or training in the management of CBRN incidents; such responders are likely to have busy and demanding roles, which may have affected their ability and willingness to complete the survey. However, the variability in response in a relatively small sample could be indicative of wider variability in decontamination practices, or at least variability within the bounds of the responses of the current sample, emphasizing the need for evidence-based, national-level guidance.
A second limitation is that the survey is based on self-report data. While we acknowledge that self-reported data can be biased, this represents the most efficient method to capture responder experiences and understanding of decontamination methods. While the responses may be subject to some bias, it is likely the responses reflect “perceived best-practice” and local adaptation of response plans to address practical and logistical constraints.
Future Work
There is currently no standard procedure for carrying out gross decontamination, and this is reflected in the fact that responses varied so much between participants. Future work is needed to identify optimum procedures for carrying out gross decontamination. Guidance should then be updated and standardized based on evidence from research, rather than relying on perceived best practice.
Supplementary Material
Acknowledgments
This project has been funded in whole or in part with federal funds from the Office of the Assistant Secretary for Preparedness and Response, Biomedical Advanced Research and Development Authority, under Contract No. HHSO100201200003C. Holly Carter and Richard Amlôt are partially funded by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Emergency Preparedness and Response at King's College London in partnership with Public Health England (PHE). The views expressed are those of the authors and not necessarily those of the funders, NHS, the NIHR, HHS, or Public Health England.
References
- 1.HM Government. The United Kingdom's Strategy for Countering Chemical, Biological, Radiological and Nuclear (CBRN) Terrorism. London: HM Government; 2010. http://webarchive.nationalarchives.gov.uk/20100418065544/http:/security.homeoffice.gov.uk/news-publications/publication-search/cbrn-guidance/strat-countering-use-of-CBRN?view=Binary Accessed June14, 2016 [Google Scholar]
- 2.Schneidmiller C. Nuclear smuggling shows terrorist WMD threat persists: State Department. Global Security Newswire August 1, 2012. http://www.nti.org/gsn/article/state-report/ Accessed Accessed June14, 2016
- 3.US Department of Homeland Security; US Department of Health and Human Services. Patient Decontamination in a Mass Chemical Exposure Incident: National Planning Guidance for Communities. Washington, DC: DHS, HHS; 2014. http://www.regulations.gov/#!documentDetail;D=DHS-2014-0012-0002 Accessed June14, 2016 [Google Scholar]
- 4.US Department of Health and Human Services. Implementation Plan for the National Health Security Strategy of the United States of America. May 2012. http://www.phe.gov/Preparednessplanning/authority/nhss/ip/Documents/nhss-ip.pdf Accessed June14, 2016
- 5.Annelli JR. The national incident management system: a multi-agency approach to emergency response in the United States of America. Rev Sci Tech 2006;25(1):223-231 [PubMed] [Google Scholar]
- 6.Baker DJ. The management of casualties following toxic agent release: the approach adopted in France. In: Marrs TC, Maynard RL, Sidell FR, eds. Chemical Warfare Agents: Toxicology and Treatment. Chichester: John Wiley & Sons; 2007:261-275 [Google Scholar]
- 7.Chilcott RP. Managing mass casualties and decontamination. Environ Int 2014;72:37-45 [DOI] [PubMed] [Google Scholar]
- 8.Maniscalco P, Christen JR, Hank JR. Homeland Security. Principles and Practice of Terrorism Response. Sudbury, MA: Jones & Bartlett; 2010 [Google Scholar]
- 9.Houston M, Henderickson RG. Decontamination. Crit Care Clin 2005;21(4):653-672 [DOI] [PubMed] [Google Scholar]
- 10.Matar H, Price SC, Chilcott RP. Temporal effects of disrobing on the skin absorption of chemical warfare agents and CW agents simulants. Toxicology 2010;278(3):344-345 [Google Scholar]
- 11.Lake WA, Fedele PD, Marshall SM. Guidelines for mass casualty decontamination during a terrorist chemical agent incident. US Army Soldier and Biological Chemical Command; 2000. http://www.ecbc.army.mil/downloads/cwirp/ECBC_cwirp_gls_mass_casualty_decon.pdf Accessed July14, 2016 [Google Scholar]
- 12.Lake WA, Schulze P, Gougelet RM. Guidelines for Mass Casualty Decontamination During a HAZMAT/Weapon of Mass Destruction Incident. Volumes 1 and 2 (Update). Fort Leonard Wood, MO: Army Chemical Biological Radiological Nuclear School; 2013 [Google Scholar]
- 13.Larner J, Jones DR, Price SC, Chilcott RP. Modified static diffusion cells for decontamination modelling. Toxicology 2010;278(3):351-352 [Google Scholar]
- 14.Amlôt R, Larner J, Matar H, et al. Comparative analysis of showering protocols for mass-casualty decontamination. Prehosp Disaster Med 2010;25(5):435-439 [DOI] [PubMed] [Google Scholar]
- 15.Wester RC, Melendres J, Maibach HI. In vivo percutaneous absorption and skin decontamination of alachlor in rhesus monkey. J Toxicol Environ Health 1992;36(1):1-12 [DOI] [PubMed] [Google Scholar]
- 16.Jones DR, Larner J, Price SC, Chilcott RP. Optimisation of mass casualty decontamination procedures in vitro. Toxicology 2010;278(3):363-364 [Google Scholar]
- 17.Health Protection Agency. CBRN Incidents: Clinical Management & Health Protection. 2008. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/340709/Chemical_biological_radiological_and_nuclear_incidents_management.pdf Accessed June14, 2016
- 18.Harvard School of Public Health; Emergency Preparedness and Response Exercise Program. Strategies for First Receiver Decontamination: A Collection of Tactics to Assist Hospitals Address Common Challenges Associated with All-Hazards Decontamination of Patients. 2013. https://cdn1.sph.harvard.edu/wp-content/uploads/sites/1608/2014/10/Hospital-Decontamination-Resources-Section-3.pdf Accessed June14, 2016
- 19.US Army Chemical, Biological, Radiological and Nuclear School. Guidelines for Military Mass Casualty Decontamination Operations During Domestic Hazmat/Weapons of Mass Destruction Incident. 2011. http://www.agile-x.com/hrfdemo/dashboard/JobAids/Final_Draft_MCD_Guidelines_for_USACBRNS.pdf Accessed July14, 2016
- 20.Bruhn KD, Brodeur JM. Addressing functional needs at a mass casualty decontamination site. CBRNe World 2014:45-48
- 21.Carter H, Drury J, Rubin GJ, Williams R, Amlôt R. Public experiences of mass casualty decontamination. Biosecur Bioterror 2012;10(3):280-289 [DOI] [PubMed] [Google Scholar]
- 22.Carter H, Drury J, Rubin GJ, Williams R, Amlôt R. The effect of communication during mass decontamination. Disaster Prev Manag 2013;22(2):132-147 [Google Scholar]
- 23.Carter H, Drury J, Amlôt R, Rubin GJ, Williams R. Effective responder communication improves efficiency and psychological outcomes in a mass decontamination field experiment: implications for public behaviour in the event of a chemical incident. PLoS One 2013;9(3):e89846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Home Office. Guidance for the United Kingdom Emergency Services on Decontamination of People Exposed to Hazardous Chemical, Biological or Radiological Substances. London: Home Office; 2013 [Google Scholar]
- 25.Stevens G, Agho K, Taylor M, Barr M, Raphael B, Jorm L. Terrorism in Australia: factors associated with perceived threat and incident-critical behaviours. BMC Public Health 2009;9:91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.The InterAgency Board. https://iab.gov/AboutUs.aspx/ Accessed December3, 2014
- 27.US Department of Commerce, Census Bureau, Geography Division (US Census). US Census Urbanized Areas Redlands, California: 2010. Accessed May12, 2015 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.