

Abstract
A dermatoscope is an important tool in a dermatologist's armamentarium as it can eliminate the need for a biopsy in a wide array of conditions. Porokeratosis was described by Mibelli and Respighi in 1893, as a disorder of keratinization which on the basis of distribution patterns was described as five clinical variants that portrayed a coronoid lamella on histopathology. We describe a case of asymptomatic, long-standing palmar and plantar pits, which on dermatoscopy showed features suggestive of porokeratosis, which was later reconfirmed by histopathologic sections. This report depicts diagnostic features of porokeratosis and obviates the need for invasive procedures for its diagnosis.
Keywords: Coronoid lamella, palmar pits, punctate porokeratosis
Porokeratosis is a heterogeneous group of disorders that are characterized clinically by a keratotic ridge with a central groove and histologically by the presence of a coronoid lamella.[1] It has been hypothesized that the condition may occur due to ultraviolet exposure,[2] immunosuppression,[3] or radiation therapy hence leading to the understanding that porokeratosis may be a premalignant condition.[4]
A 40-year-old man, without a remarkable medical history, presented with multiple asymptomatic pits on the palms and soles, which were static over the last 5 years. Physical examination showed minute discreet 2–3 mm crateriform lesions with surrounding normal skin and scaly well-defined borders on the palms [Figure 1]. Similar lesions were seen on the plantar aspect of feet [Figure 2]. No other cutaneous or mucosal pathology was noticed. Dermatoscopy of the lesions was done, which revealed multiple yellowish annular structures that resembled volcanic craters. The periphery of each lesion showed a “white-track” structure with homogeneous tan brown globules in the center [Figure 3]. Gentian violet application stained and highlighted the lesion periphery on dermatoscopy [Figure 4]. The lesions were diagnosed on the basis of dermatoscopy as porokeratosis palmaris et plantaris, which was confirmed on biopsy. Serial histopathology sections, with H & E staining, revealed compact hyperkeratosis with small zones of perpendicularly oriented parakeratosis, hence confirming the dermatoscopic diagnosis of porokeratosis [Figure 5].
Figure 1.

Minute discrete 2–3 mm crateriform lesions with surrounding normal skin and scaly well-defined borders
Figure 2.

2–3 mm crateriform minute lesions with well-defined borders on the plantar aspect of feet
Figure 3.

The periphery of each lesion showed a “white-track” structure with homogenous tan brown globules in the center on dermatoscopy
Figure 4.

Gentian violet application stained and highlighted the lesion periphery on dermatoscopy
Figure 5.
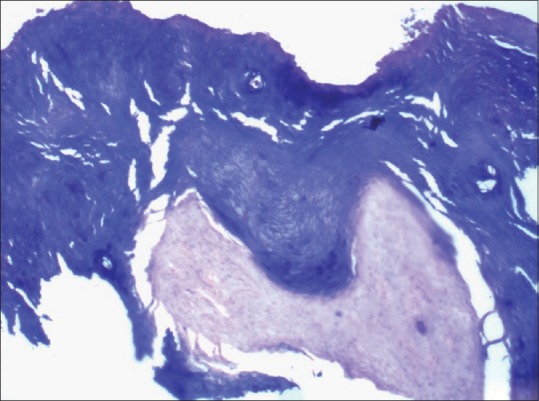
Compact hyperkeratosis with zones of parakeratosis, which are perpendicularly oriented (H and E, 10x)
Multiple methodologies have been recruited to diagnose porokeratosis without the need for a biopsy. These include the application of gentian violet over the lesion and removal of excess dye with alcohol.[5] This method highlights the keratotic ridge due to accumulation of the dye in the groove. In the same manner, povidone iodine has also been used to accentuate the groove.[6] Delfino et al. described their findings of porokeratosis, using a 10-fold magnification stereomicroscope, as the outline of a volcanic crater observed from a high point.[7] In our case, dermatoscopic features were consistent with porokeratosis and a diagnosis was made prior to procuring the histology report. The lesions were multiple and minute involving only the palms leading to a final diagnosis of punctate porokeratosis.
The classical coronoid lamella may be missed if the biopsy does not involve the hyperkeratotic ridge. Serial sections may be required to identify the cornoid lamella when the hyperkeratotic ridge is biopsied; however, sometimes the cornoid lamella may be small that it may be missed. This report highlights dermatoscopic features that aid in the diagnosis of porokeratosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Palleschi GM, Torchia D. Porokeratosis of Mibelli and superficial disseminated porokeratosis. J Cutan Pathol. 2008;35:253–5. doi: 10.1111/j.1600-0560.2007.00787.x. [DOI] [PubMed] [Google Scholar]
- 2.Katugampola RP, Finlay AY. Fake sun tan diagnosis of porokeratosis. J Eur Acad Dermatol Venereol. 2006;20:224–6. doi: 10.1111/j.1468-3083.2006.01381.x. [DOI] [PubMed] [Google Scholar]
- 3.Cha SH, Park HJ, Lee JY, Cho BK. Atypical porokeratosis developing following bone marrow transplantation in a patient with myelodysplastic syndrome. Ann Dermatol. 2010;22:206–8. doi: 10.5021/ad.2010.22.2.206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Karthikeyan K, Thappa DM, Udayashankar C. Porokeratosis of Mibelli with nail dystrophy. J Dermatol. 2003;30:420–2. doi: 10.1111/j.1346-8138.2003.tb00410.x. [DOI] [PubMed] [Google Scholar]
- 5.Thomas CJ, Elston DM. Medical pearl: Gentian violet to highlight the cornoid lamella in disseminated superficial actinic porokeratosis. J Am Acad Dermatol. 2005;52(3 Pt 1):513–4. doi: 10.1016/j.jaad.2004.06.050. [DOI] [PubMed] [Google Scholar]
- 6.Redondo P, Sola MA, Lloret P. Porokeratosis and povidone-iodine: A new clinical diagnostic sign. Br J Dermatol. 2002;147:383. doi: 10.1046/j.1365-2133.2002.04635.x. [DOI] [PubMed] [Google Scholar]
- 7.Delfino M, Argenziano G, Nino M. Dermoscopy for the diagnosis of porokeratosis. J Eur Acad Dermatol Venereol. 2004;18:194–5. doi: 10.1111/j.1468-3083.2004.00462.x. [DOI] [PubMed] [Google Scholar]