

Abstract
Objective:
To determine the association of ultraearly hematoma growth (uHG) with the CT angiography (CTA) spot sign, hematoma expansion, and clinical outcomes in patients with acute intracerebral hemorrhage (ICH).
Methods:
We analyzed data from 231 patients enrolled in the multicenter Predicting Haematoma Growth and Outcome in Intracerebral Haemorrhage Using Contrast Bolus CT study. uHG was defined as baseline ICH volume/onset-to-CT time (mL/h). The spot sign was used as marker of active hemorrhage. Outcome parameters included significant hematoma expansion (>33% or >6 mL, primary outcome), rate of hematoma expansion, early neurologic deterioration, 90-day mortality, and poor outcome.
Results:
uHG was higher in spot sign patients (p < 0.001) and in patients scanned earlier (p < 0.001). Both uHG >4.7 mL/h (p = 0.002) and the CTA spot sign (p = 0.030) showed effects on rate of hematoma expansion but not its interaction (2-way analysis of variance, p = 0.477). uHG >4.7 mL/h improved the sensitivity of the spot sign in the prediction of significant hematoma expansion (73.9% vs 46.4%), early neurologic deterioration (67.6% vs 35.3%), 90-day mortality (81.6% vs 44.9%), and poor outcome (72.8% vs 29.8%), respectively. uHG was independently related to significant hematoma expansion (odds ratio 1.06, 95% confidence interval 1.03–1.10) and clinical outcomes.
Conclusions:
uHG is a useful predictor of hematoma expansion and poor clinical outcomes in patients with acute ICH. The combination of high uHG and the spot sign is associated with a higher rate of hematoma expansion, highlighting the need for very fast treatment in ICH patients.
The influence of baseline intracerebral hemorrhage (ICH) volume on outcome varies depending on time from symptoms onset to baseline CT scan. We previously reported that the adjustment of baseline ICH volume by onset to baseline CT time, coined as ultraearly hematoma growth (uHG), improves the ability of baseline ICH volume to predict clinical outcome and helps to identify patients at risk of hematoma expansion.1 However, the influence of uHG on hematoma expansion and subsequent poor clinical outcome may vary widely depending on the presence of active hemorrhage.
The CT angiography (CTA) spot sign is a marker of active hemorrhage and a strong predictor of hematoma expansion and poor outcome in acute ICH.2–6 Our previous study suggested that patients with the spot sign present higher uHG than those without.1 We hypothesized that patients with higher uHG have higher spot sign prevalence and are more likely to expand and to present poorer outcomes than those with lower uHG.
The objectives of this study were to determine the association of uHG with the CTA spot sign, hematoma expansion, and clinical outcomes in patients with acute ICH from the Predicting Haematoma Growth and Outcome in Intracerebral Haemorrhage Using Contrast Bolus CT (PREDICT) study.4 We also aimed to compare the ability of uHG, ICH volume, and the CTA spot sign to predict hematoma expansion and clinical outcome, and to validate the uHG in a multicenter cohort to address its generalizability.
METHODS
Participants.
The methodology of the PREDICT study has been described previously in detail.4 In brief, PREDICT was a multicenter, prospective, observational cohort study of consecutive adult patients with spontaneous ICH presenting within 6 hours from symptoms onset. In order to validate our previous findings, all patients from the entire PREDICT study cohort7 were eligible for the present study except those included by Vall d'Hebron University Hospital, Barcelona, Spain, since some of them were included in our previous single-center study.1
Standard protocol approvals, registrations, and patient consents.
The PREDICT study protocol was approved by the research ethics board of the University of Calgary, Alberta, Canada. Requirement for additional local ethics approval differed among participating countries and additional consent was obtained if required by the local ethics board. Patients, next of kin, or legal guardian gave written informed consent according to the requirements established by each site ethics board.
Procedures.
Relevant demographic and clinical characteristics were recorded. The NIH Stroke Scale (NIHSS) score on admission and at 24 hours was collected, as well as modified Rankin Scale (mRS) score at 90 days. Noncontrast CT scan at baseline and at 24 hours and single-phase CTA immediately after baseline CT scan were performed. Details of image acquisition, processing, and analysis have been described before.4 The time of onset was defined as the time of symptoms onset or the last time seen normal. uHG was defined as baseline ICH volume (mL) divided by onset to baseline CT time (hours).1 Therefore, uHG can be conceived of as the initial rate of growth of the hematoma. This conception of the meaning of uHG assumes that hematoma growth rates are linear in time. CTA spot sign was defined according to previously established criteria.8 The spot sign was used as marker of active hemorrhage.2–6
Outcomes.
The primary outcome parameter was significant hematoma expansion at 24-hour CT defined as ICH relative enlargement of more than 33% or absolute growth greater than 6 mL from baseline CT.4 The rate of hematoma expansion, defined as the difference between baseline and 24-hour ICH volume (mL) divided by baseline to 24-hour CT time (hours),9 was evaluated as a secondary outcome.
Clinical outcome parameters included early neurologic deterioration, mortality at 90 days, and poor outcome. Early neurologic deterioration was defined as an increase greater than or equal to 4 points in the NIHSS score or death at 24 hours, and poor outcome as an mRS score greater than 2 at 90 days. Patients with an mRS score greater than 2 at baseline were excluded from poor outcome analysis.
Statistical analysis.
Statistical analysis was performed using SPSS (Chicago, IL) 17.0 software. The categorical variables are presented as absolute values (%) and the continuous variables as means ± SD or medians (interquartile intervals). Statistical significance for intergroup differences was assessed by Pearson χ2 for categorical variables and by Student t test, Mann-Whitney U test, or Kruskal-Wallis test for continuous variables, as appropriate. The association between uHG and significant hematoma expansion was assessed using a Mann-Whitney U test. Multivariable logistic regression analysis was used to provide an adjusted estimate of the effect size of the association between uHG and significant hematoma expansion. Key covariates were age, sex, anticoagulant use, baseline NIHSS score, ICH location, and intraventricular extension. Specifically, baseline ICH volume and onset to baseline CT time were not covariates because these are components of the uHG construct. This analysis was repeated for clinical outcome parameters. Results are presented as odds ratio (OR) and 95% confidence interval (CI). A post hoc sensitivity analysis was performed to assess the association between uHG and significant hematoma expansion by tertiles of uHG. Receiver operating characteristic curves were drawn to estimate possible threshold values of uHG and baseline ICH volume that would optimally predict the primary outcome. The threshold was estimated at the simultaneous maximum sensitivity and specificity. The sensitivity, specificity, predictive values, and area under the curve (AUC) of uHG, baseline ICH volume, and the CTA spot sign were calculated. A 2-way analysis of variance was used to assess the interaction of uHG and CTA spot sign on rate of hematoma expansion. A 2-sided p value of <0.05 was considered significant for all tests.
RESULTS
Among 386 patients of the entire PREDICT study cohort, 231 were included in the present study. A total of 155 participants were excluded for the following reasons: 129 were included by Vall d'Hebron University Hospital, 20 underwent baseline CT scan beyond 6 hours, and 6 did not have available baseline CT or CTA images.
uHG, CTA spot sign, and onset to baseline CT time.
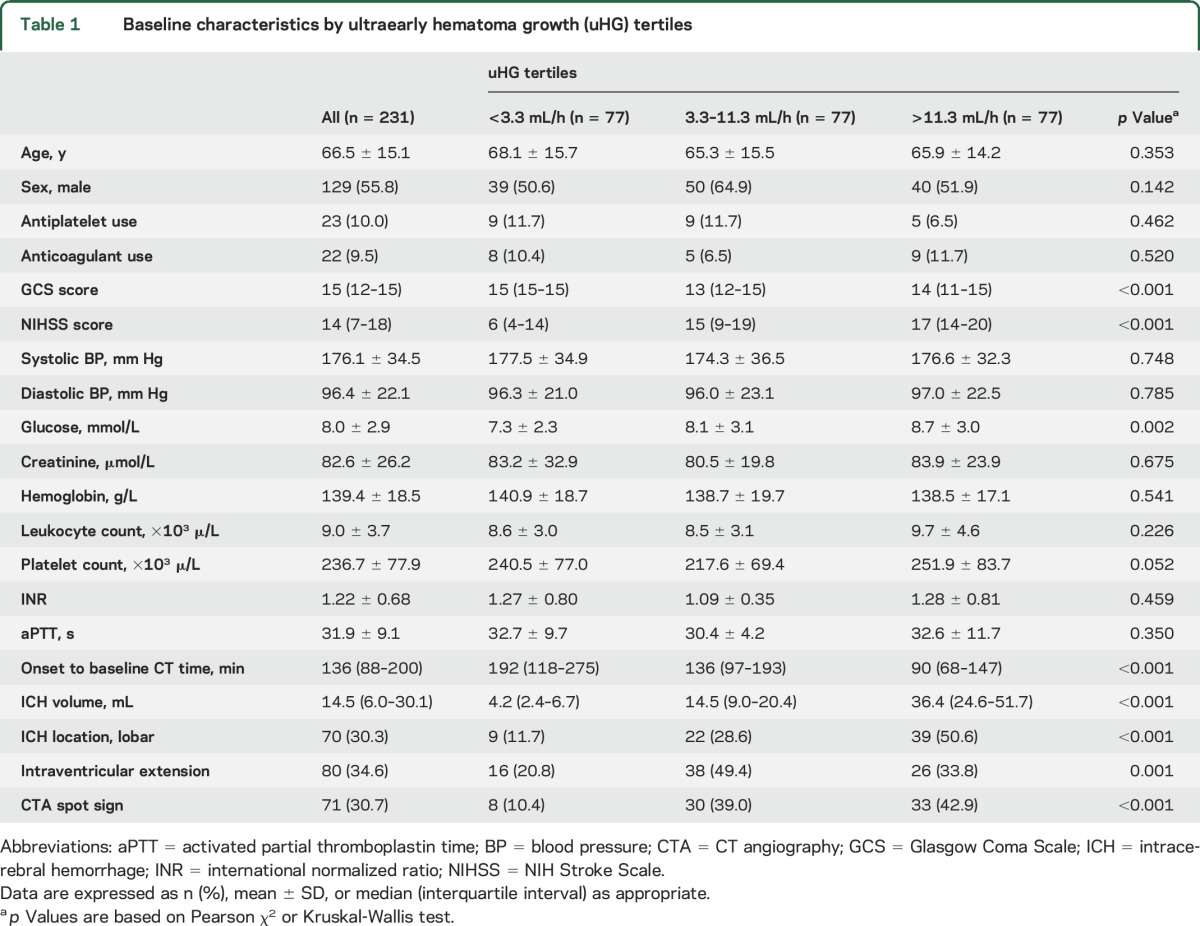
Median uHG was 6.5 (2.5–14.3) mL/h. Patients with higher uHG had lower Glasgow Coma Scale scores and higher NIHSS scores and glucose levels, and more frequently presented intraventricular extension and lobar location at baseline (table 1). The CTA spot sign was present in 71 (30.7%) patients, and 26 (36.6%) of them showed multiple spot signs. uHG was higher in patients with the CTA spot sign (11.1 [5.6–17.4] vs 4.2 [1.9–12.3] mL/h, p < 0.001) but similar in patients with multiple spot signs than those with a single spot sign (10.3 [5.7–16.6] vs 11.3 [5.4–18.5] mL/h, p = 0.642). uHG above the median value predicted the presence of a CTA spot sign with 71.8% sensitivity and 60% specificity.
Table 1.
Baseline characteristics by ultraearly hematoma growth (uHG) tertiles
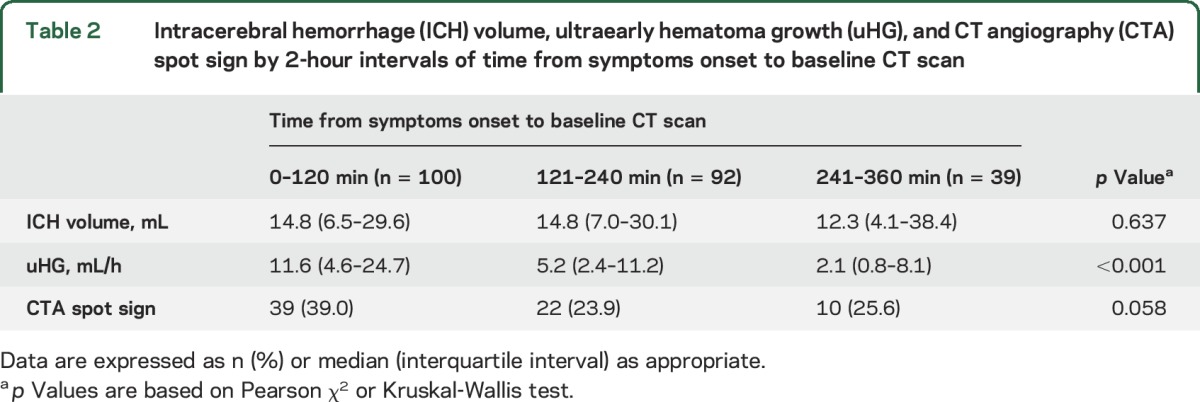
Patients scanned earlier presented higher uHG and tended to present a CTA spot sign more frequently despite having similar ICH volumes (table 2). By 2-hour intervals from symptoms onset, the uHG was higher the earlier the patients were scanned in patients with the spot sign (13.6 [7.1–28.9], 9.2 [5.3–12.8], and 9.5 [2.4–14.9] mL/h, p = 0.041) but particularly in those without the spot sign (11.1 [3.1–20.7], 3.7 [1.9–10.3], and 1.4 [0.6–3.5] mL/h, p < 0.001), respectively. Baseline NIHSS score was higher in patients scanned earlier (15 [8–19], 13 [7–17], and 9 [3–19], respectively, p = 0.042), while other baseline characteristics were not related to onset to baseline CT time (p ≥ 0.050 for all comparisons, data not shown).
Table 2.
Intracerebral hemorrhage (ICH) volume, ultraearly hematoma growth (uHG), and CT angiography (CTA) spot sign by 2-hour intervals of time from symptoms onset to baseline CT scan
uHG, CTA spot sign, and hematoma expansion.
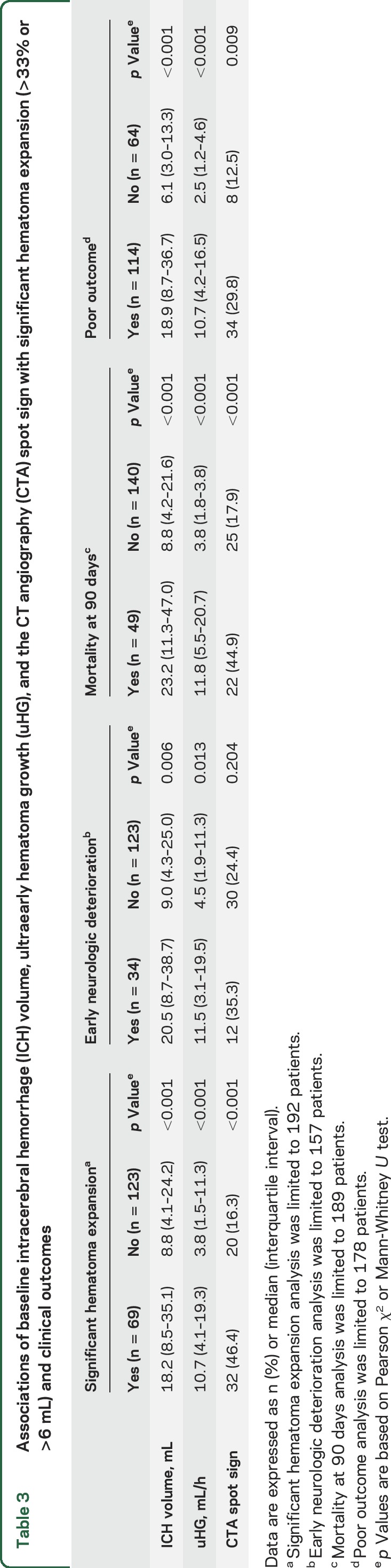
Outcome analyses were limited to 202 patients after the exclusion of 14 patients treated with off-label recombinant factor VIIa and 15 who underwent a neurosurgical procedure (hematoma evacuation or ventriculostomy). Significant hematoma expansion (>33% or >6 mL) occurred in 69 (35.9%) of 192 patients who had a 24-hour CT scan. Both uHG and the CTA spot sign were positively related to significant hematoma expansion (table 3). The association of both uHG (OR 1.07, 95% CI 1.04–1.11) and the CTA spot sign (OR 3.16, 95% CI 1.52–6.57) with the primary outcome remained significant in separate multivariate models adjusted for age, sex, anticoagulant use, baseline NIHSS score, ICH location, and intraventricular extension. In a post hoc sensitivity analysis, the frequency of significant hematoma expansion was higher by tertiles of uHG (21.1%, 38.3%, and 50.8%, respectively, p = 0.002).
Table 3.
Associations of baseline intracerebral hemorrhage (ICH) volume, ultraearly hematoma growth (uHG), and the CT angiography (CTA) spot sign with significant hematoma expansion (>33% or >6 mL) and clinical outcomes
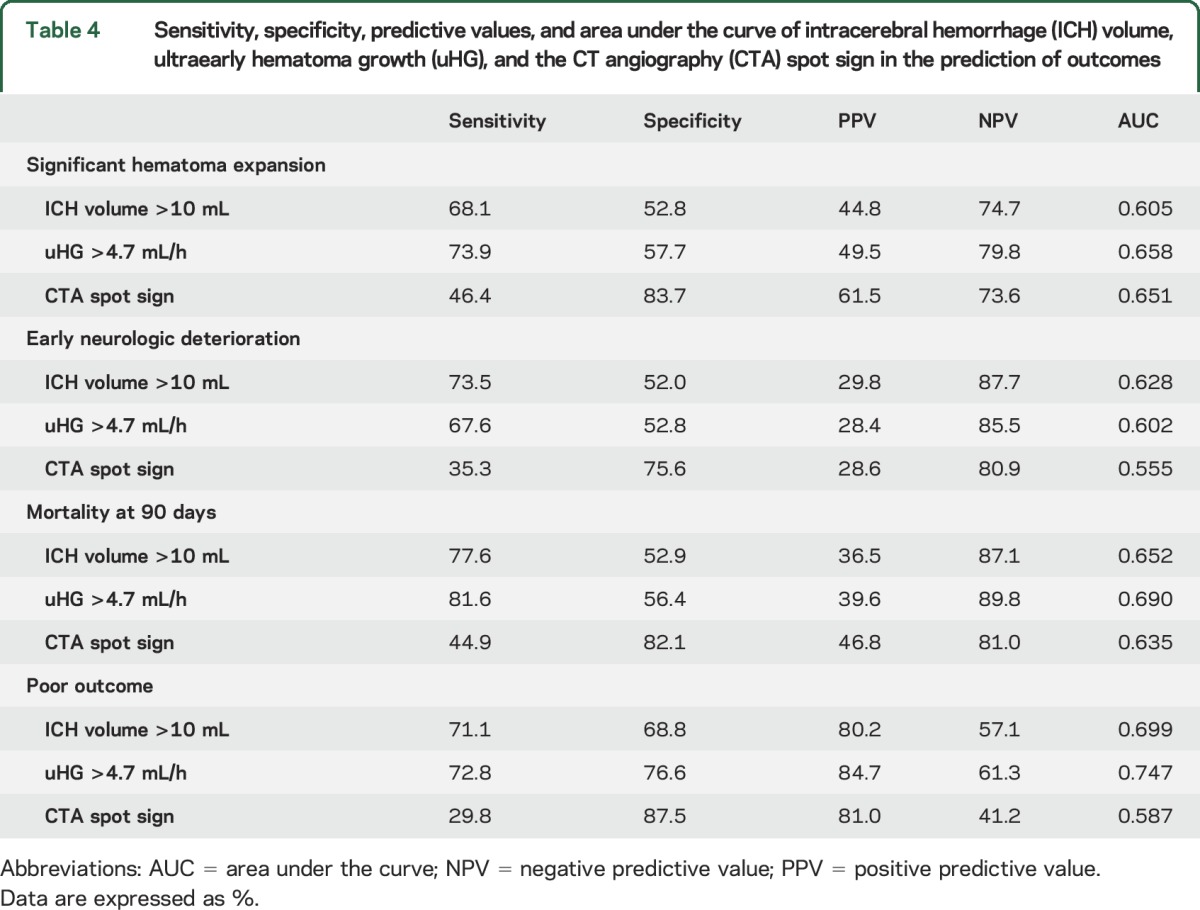
The simultaneous maximum sensitivity and specificity for uHG in predicting the primary outcome was 4.7 mL/h and for baseline ICH volume 10 mL. uHG >4.7 mL/h improved the ability of baseline ICH volume >10 mL to predict significant hematoma expansion (table 4). Further, uHG >4.7 mL/h had higher sensitivity and negative predictive value but lower specificity and positive predictive value than the CTA spot sign (table 4). The composite of uHG >4.7 mL/h or CTA spot sign (AUC 0.632) as well as of uHG >4.7 mL/h and CTA spot sign (AUC 0.631) did not improve the AUC of uHG or CTA spot sign separately (table 4).
Table 4.
Sensitivity, specificity, predictive values, and area under the curve of intracerebral hemorrhage (ICH) volume, ultraearly hematoma growth (uHG), and the CT angiography (CTA) spot sign in the prediction of outcomes
Median rate of hematoma expansion from baseline to 24-hour CT scan was 0.05 (0–0.33) mL/h. The rate of hematoma expansion was higher in patients with uHG >4.7 mL/h (0.17 [0.02–0.71] vs 0.01 [0–0.06] mL/h, p < 0.001) and in those with the presence of the CTA spot sign (0.32 [0.06–1.05] vs 0.02 [0–0.15] mL/h, p < 0.001). A 2-way analysis of variance showed effects of both uHG >4.7 mL/h (p = 0.002) and the CTA spot sign (p = 0.030) but not its interaction (p = 0.477) on rate of hematoma expansion (figure).
Figure. Relationship between ultraearly hematoma growth (uHG), CT angiography (CTA) spot sign, and rate of hematoma expansion.
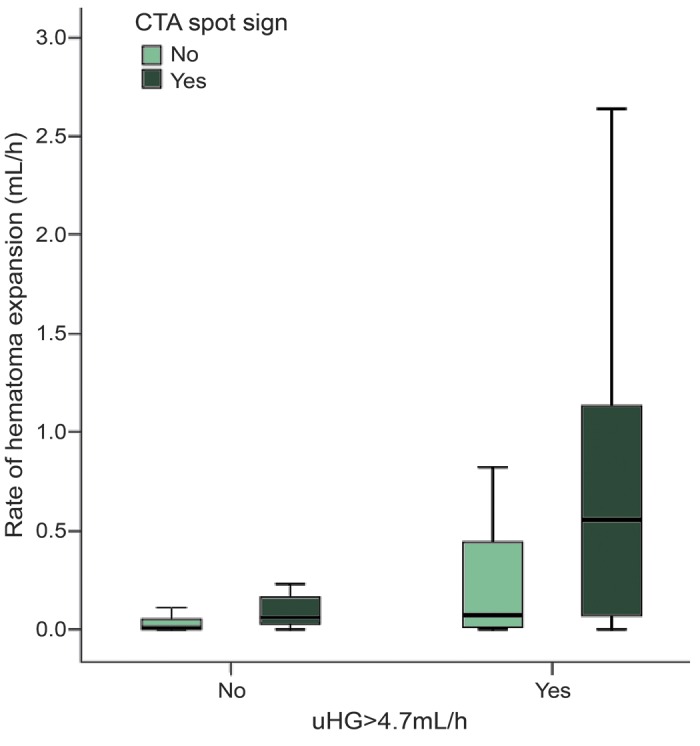
Boxplot graphs of rate of hematoma expansion categorized by uHG >4.7 mL/h and clustered by the presence of the CTA spot sign. Higher rate of hematoma expansion was observed in patients with uHG >4.7 mL/h, particularly in those with a CTA spot sign. No interaction was found between uHG >4.7 mL/h and the CTA spot sign (2-way analysis of variance, p = 0.477), indicating that the effect of uHG and the spot sign on the rate of hematoma expansion does not depend on each other, and therefore its combination increases the effect.
uHG, CTA spot sign, and clinical outcomes.
A total of 157 patients have available 24-hour clinical data and 189 participants were successfully followed up at 90 days, 11 of which were excluded from poor outcome analysis because they had a mRS score greater than 2 at baseline. Early neurologic deterioration occurred in 34 (21.7%) patients, 49 (25.9%) participants had died at 90 days, and 114 (64%) had a poor outcome (mRS score 3–6).
Both uHG and the CTA spot sign were positively related to all clinical outcome parameters (table 3). uHG was independently related to early neurologic deterioration (OR 1.06, 95% CI 1.02–1.10), mortality at 90 days (OR 1.05, 95% CI 1.01–1.10), and poor outcome (OR 1.10, 95% CI 1.02–1.18) in multivariate models adjusted for age, sex, anticoagulant use, baseline NIHSS score, ICH location, and intraventricular extension. uHG >4.7 mL/h improved the ability of baseline ICH volume >10 mL to predict clinical outcomes, including mortality at 90 days and poor outcome, with the exception of somewhat higher sensitivity and predictive values for ICH volume >10 mL in the prediction of early neurologic deterioration (table 4). uHG >4.7 mL/h had lower specificity and positive predictive value (except for poor outcome) but higher sensitivity and negative predictive value than the CTA spot sign in the prediction of clinical outcomes (table 4).
DISCUSSION
The present study demonstrates that uHG is higher in patients with the CTA spot sign and the earlier the patients are scanned, particularly in those without the spot sign. Further, uHG independently predicts significant hematoma expansion, early neurologic deterioration, mortality at 90 days, and poor outcome. This study also reveals that uHG improves the sensitivity, but not the specificity, of the CTA spot sign in the prediction of significant hematoma expansion and clinical outcomes.
ICH expands over time, mainly within the first 6 hours from symptoms onset,10,11 due to continued bleeding and rebleeding.12 Because there are varying velocities of expansion, hematoma growth may be markedly nonlinear and the speed of the hematoma expansion cannot be calculated accurately. The uHG is the average rate of hematoma expansion before baseline CT scan. Therefore, despite uHG being higher in patients scanned earlier in our study, uHG represents an instantaneous rate of growth of the hematoma at the time the CT scan is performed and may act as a surrogate of the speed of hematoma expansion.1
As expected, uHG was greater the earlier the patients were scanned, since by definition the uHG denominator will always be smaller in the early time window. In addition, larger ICH volumes at baseline may occur among patients presenting earlier. Both the numerator and denominator may act synergistically to give larger values of uHG. Although the CTA spot sign and NIHSS score were higher the earlier the patients presented, other baseline characteristics, including ICH volume, were not related to onset to baseline CT time. Therefore, clinical severity does not seem to exert a relevant confounding effect on uHG in our study.
The CTA spot sign is a validated predictor of hematoma expansion in patients with acute ICH and is a marker of active hemorrhage at the site of vessel rupture.2–6 This is why 3 ongoing hemostatic clinical trials stratify patients according to the presence of a CTA spot sign, including Spot Sign Selection of Intracerebral Hemorrhage to Guide Hemostatic Therapy (SPOTLIGHT, NCT01359202), the Spot Sign for Predicting and Treating ICH Growth Study (STOP-IT, NCT00810888), and the Spot Sign and Tranexamic Acid on Preventing ICH Growth–Australasia Trial (STOP-AUST).13 In the present study, patients with the spot sign presented higher uHG than those without. However, the time-dependency of uHG was particularly true in those patients without the spot sign, supporting a different influence of time on hematoma growth depending on the presence of active hemorrhage. On the one hand, the lower influence of time on hematoma growth in patients with the spot sign suggests that, although uHG decreases over time, uHG could decrease more slowly, not decrease, or turn into a faster rate in the presence of active hemorrhage.14,15 On the other hand, the higher influence of time on hematoma growth in patients without the spot sign suggests a rapid decay in the rate of growth in the absence of active hemorrhage. This would argue that time is a major factor in the dynamics of hematoma growth especially for those patients without spot sign. This finding has potential implications for future clinical trials design since a subset of ICH patients without the spot sign could also benefit from hemostatic treatment if treated in the ultraearly time window, for example, within 2 hours from symptoms onset.
Similarly to uHG, a higher rate of hematoma expansion between baseline and follow-up CT scans has been related to poorer outcomes.9 In our study, the rate of hematoma expansion was related to both uHG and the spot sign, without interaction of uHG and the spot sign. Therefore, the combination of uHG and the spot sign increases the effect on the rate of hematoma expansion, reinforcing the hypothesis that the rate of hematoma expansion can turn into a faster rate in the presence of active hemorrhage.
As observed in our prior study,1 uHG independently predicted significant hematoma expansion and clinical outcomes. uHG was recently validated as a powerful predictor of poor outcome in a pooled analysis of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) and INTERACT2 studies.16 However, these trials included a subpopulation of ICH patients with elevated systolic blood pressure (150–220 mm Hg) able to be actively treated and admitted to a monitored facility within 6 hours of stroke onset.17,18 These criteria may represent the exclusion of up to 25% of acute ICH patients,19 which may therefore reduce its generalizability to clinical practice. The present observational study improves the generalizability of uHG by validating it in a broader range of ICH patients.
The success of emerging and future interventions aimed at preventing hematoma expansion and subsequent poor outcome, including hemostatic drugs, will likely depend on the accurate selection of patients at risk of hematoma expansion. In the present study, uHG improved the ability of baseline ICH volume to predict all studied outcomes. Conversely, uHG improved the sensitivity and negative predictive value but not the specificity and positive predictive value of the CTA spot sign in the prediction of significant hematoma expansion and clinical outcomes. Therefore, the combination of both uHG and the spot sign could allow better stratification of patients at risk of hematoma expansion and poorest outcomes. uHG could be particularly useful in those scenarios where it is not possible to perform a CTA scan, including those sites that are unable to perform CTA in the hyperacute phase of ICH and those patients with known contraindication to CTA, such as renal failure or allergy to iodinated contrast dye.
The strengths of this study include the heterogeneous patient population, the early assessment of patients after symptoms onset, and the rigorous blinded assessment of ICH volume, the CTA spot sign, and outcome parameters. The study has some limitations, however. First, the time of onset was defined as the time of symptoms onset or the last time seen normal. This may have led to underestimation of uHG in those patients with uncertainty on the exact time from symptoms onset and therefore predictive values of uHG in this study were not as robust as in our prior study.1 Second, we assumed a linear uHG in our analyses but the hematoma expansion rate may be not linear. Third, we used the CTA spot sign as a marker of active hemorrhage,2–6 but the exact pathology of the spot sign is not known and it may not only represent active hemorrhage.5 We compared uHG with single-phase CTA spot sign, while multiphase CTA could improve the sensitivity of the spot sign in the prediction of hematoma expansion.7,20,21 Finally, because our results represent a secondary analysis of an existing dataset, they are exploratory and should be replicated.
uHG is a useful predictor of hematoma expansion and poor clinical outcomes in patients with acute ICH. uHG is higher in patients with active hemorrhage and in patients scanned earlier. The combination of both high uHG and the CTA spot sign is associated with a higher rate of hematoma expansion. These data may help lead to a better selection of patients at risk of hematoma expansion and poorest clinical outcomes in future trials, highlighting the need for very fast treatment in patients with acute ICH.
Supplementary Material
GLOSSARY
- AUC
area under the curve
- CI
confidence interval
- CTA
CT angiography
- ICH
intracerebral hemorrhage
- INTERACT
Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial
- mRS
modified Rankin Scale
- NIHSS
NIH Stroke Scale
- OR
odds ratio
- PREDICT
Predicting Haematoma Growth and Outcome in Intracerebral Haemorrhage Using Contrast Bolus CT
- uHG
ultraearly hematoma growth
Footnotes
Supplemental data at Neurology.org
Contributor Information
Collaborators: PREDICT/Sunnybrook ICH CTA Study Group, Bijoy K. Menon, Jayme Kosior, Suresh Subramaniam, Sara Tymchuk, Dion Fung, Nandavar Shobha, Simerpreet Bal, Sanjith Aaron, Alexander Poppe, Nikolai Steffenhagen, Talip Asil, Pablo Garcia-Bermejo, Francois Moreau, Pawan Ojha, Ana Calleja, Andres Venegas, Mohammed Al-Mekhlafi, Negar Asdaghi, Philip A. Barber, Tim Watson, Shelagh B. Coutts, Eric E. Smith, David Gladstone, Sebastia Remollo, Hjordis Hentschel, Volker Puetz, Betty A. Schwarz, Adam Kobayashi, Tomasz Litwin, Jan Bembenek, Marta Bilik, Grzegorz Chabik, Katarzyna Grabska, Marcin Gluszkiewicz, Julia Jedrzejewska, Anna Piorkowska, Marta Skowronska, Urszula Stepien, Anna Sliwinska, Martine Mainville, Helena Lau, Felix Koyfman, Barbara Voetsch, Nicholas E. Tarlov, Judith Jarrett, Suskalyan Purkayastha, and Hirak Roychowdhury
AUTHOR CONTRIBUTIONS
Dr. Rodriguez-Luna: study coordination. Dr. Rodriguez-Luna and Dr. Molina: study concept or design and statistical analysis. Dr. Rodriguez-Luna, Dr. Coscojuela, Dr. Rubiera, Dr. Hill, Dr. Dowlatshahi, Dr. Tomasello, Dr. Demchuk, and Dr. Molina: analysis or interpretation of data. All authors: acquisition of data and drafting/revising the manuscript.
STUDY FUNDING
The PREDICT study was supported by Canadian Stroke Consortium and NovoNordisk Canada. External support from the Canadian Stroke Consortium and NovoNordisk Canada was received to cover costs of study enrollment.
DISCLOSURE
D. Rodriguez-Luna was supported by the Carlos III Health Institute and the Vall d’Hebron Research Institute. P. Coscojuela, M. Rubiera, and M. Hill report no disclosures relevant to the manuscript. D. Dowlatshahi was supported by a uOttawa Department of Medicine Clinician-Scientist Research Chair and a Heart & Stroke Foundation of Canada New Investigator Award. R. Aviv, Y. Silva, I. Dzialowski, C. Lum, A. Czlonkowska, J. Boulanger, C. Kase, G. Gubitz, R. Bhatia, V. Padma, J. Roy, and A. Tomasello report no disclosures relevant to the manuscript. A. Demchuk was supported by the Heart and Stroke Foundation, the Hotchkiss Brain Institute, and Alberta Innovates Health Solutions. C. Molina reports no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Rodriguez-Luna D, Rubiera M, Ribo M, et al. Ultraearly hematoma growth predicts poor outcome after acute intracerebral hemorrhage. Neurology 2011;77:1599–1604. [DOI] [PubMed] [Google Scholar]
- 2.Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke 2007;38:1257–1262. [DOI] [PubMed] [Google Scholar]
- 3.Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology 2007;68:889–894. [DOI] [PubMed] [Google Scholar]
- 4.Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol 2012;11:307–314. [DOI] [PubMed] [Google Scholar]
- 5.Dowlatshahi D, Wasserman JK, Momoli F, et al. Evolution of computed tomography angiography spot sign is consistent with a site of active hemorrhage in acute intracerebral hemorrhage. Stroke 2014;45:277–280. [DOI] [PubMed] [Google Scholar]
- 6.Brouwers HB, Raffeld MR, van Nieuwenhuizen KM, et al. CT angiography spot sign in intracerebral hemorrhage predicts active bleeding during surgery. Neurology 2014;83:883–889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rodriguez-Luna D, Dowlatshahi D, Aviv RI, et al. Venous phase of computed tomography angiography increases spot sign detection, but intracerebral hemorrhage expansion is greater in spot signs detected in arterial phase. Stroke 2014;45:734–739. [DOI] [PubMed] [Google Scholar]
- 8.Thompson AL, Kosior JC, Gladstone DJ, et al. Defining the CT angiography “spot sign” in primary intracerebral hemorrhage. Can J Neurol Sci 2009;36:456–461. [DOI] [PubMed] [Google Scholar]
- 9.Romero JM, Heit JJ, Delgado Almandoz JE, et al. Spot sign score predicts rapid bleeding in spontaneous intracerebral hemorrhage. Emerg Radiol 2012;19:195–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fujii Y, Tanaka R, Takeuchi S, et al. Hematoma enlargement in spontaneous intracerebral hemorrhage. J Neurosurg 1994;80:51–57. [DOI] [PubMed] [Google Scholar]
- 11.Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke 1996;27:1783–1787. [DOI] [PubMed] [Google Scholar]
- 12.Qureshi AI, Tuhrim S, Broderick JP, et al. Spontaneous intracerebral hemorrhage. N Engl J Med 2001;344:1450–1460. [DOI] [PubMed] [Google Scholar]
- 13.Meretoja A, Churilov L, Campbell BC, et al. The Spot Sign and Tranexamic Acid on Preventing ICH Growth–Australasia Trial (STOP-AUST): protocol of a phase II randomized, placebo-controlled, double-blind, multicenter trial. Int J Stroke 2014;9:519–524. [DOI] [PubMed] [Google Scholar]
- 14.Brouwers HB, Falcone GJ, McNamara KA, et al. CTA spot sign predicts hematoma expansion in patients with delayed presentation after intracerebral hemorrhage. Neurocrit Care 2012;17:421–428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bermejo PG, Garcia JA, Perez-Fernandez S, Arenillas JF. Spot sign and live-imaged dramatic intracerebral hematoma expansion. Neurology 2010;75:834. [DOI] [PubMed] [Google Scholar]
- 16.Sato S, Arima H, Hirakawa Y, et al. The speed of ultraearly hematoma growth in acute intracerebral hemorrhage. Neurology 2014;83:2232–2238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Anderson CS, Huang Y, Wang JG, et al. Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage trial (INTERACT): a randomised pilot trial. Lancet Neurol 2008;7:391–399. [DOI] [PubMed] [Google Scholar]
- 18.Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368:2355–2365. [DOI] [PubMed] [Google Scholar]
- 19.Qureshi AI, Ezzeddine MA, Nasar A, et al. Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Am J Emerg Med 2007;25:32–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tsukabe A, Watanabe Y, Tanaka H, et al. Prevalence and diagnostic performance of computed tomography angiography spot sign for intracerebral hematoma expansion depend on scan timing. Neuroradiology 2014;56:1039–1045. [DOI] [PubMed] [Google Scholar]
- 21.Ciura VA, Brouwers HB, Pizzolato R, et al. Spot sign on 90-second delayed computed tomography angiography improves sensitivity for hematoma expansion and mortality: prospective study. Stroke 2014;45:3293–3297. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.