

Summary:
Anthracosis is defined as black, dense pigments in tissues, usually carbon deposits. We, as surgeons, have to make decisions during surgery to the best of our knowledge and based on what the literature provides us. We present the case of a 30-year-old female patient who underwent abdominoplasty. During surgery, bilateral inguinal pigmented and enlarged lymph nodes were seen. Biopsy of the nodes was done to rule out any malignancy. The results showed tattoo pigments on all lymph nodes. We present this case as tattoo pigment migration, which has been rarely described.
We have come to know anthracosis as mainly a pulmonary disease secondary to long-term exposure to carbon. But if we search for an adequate definition, anthracosis refers to a black, dense pigment in tissues.1
CASE REPORT
We present a 30-year-old female patient with abdominal flaccidity wanting correction. During physical examination, a Matarasso class III abdominal flaccidity was found (Figs. 1 and 2). She was scheduled for an abdominoplasty. During dissection of the abdominal dermal flap, various enlarged lymph nodes were found on both inguinal areas. They were 3–4 cm in diameter and had a dark black coloration inside them. They were resected and subjected to pathological analysis to rule out any malignant disease (eg, vulvar neoplasia or a distant melanoma; Figs. 3 and 4). After analysis by the department of pathology, the probability of malignancy was discarded.
Fig. 1.

Anterior view of the patient. The tattoos are noticed on the lower extremities.
Fig. 2.

Lateral view of the patient is displayed.
Fig. 3.
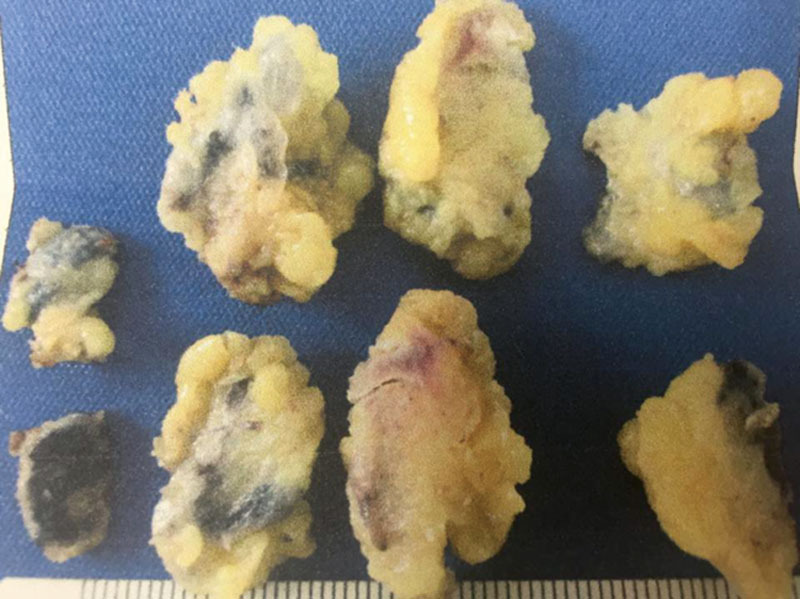
Macroscopic view of lymph nodes showing black pigmentation.
Fig. 4.
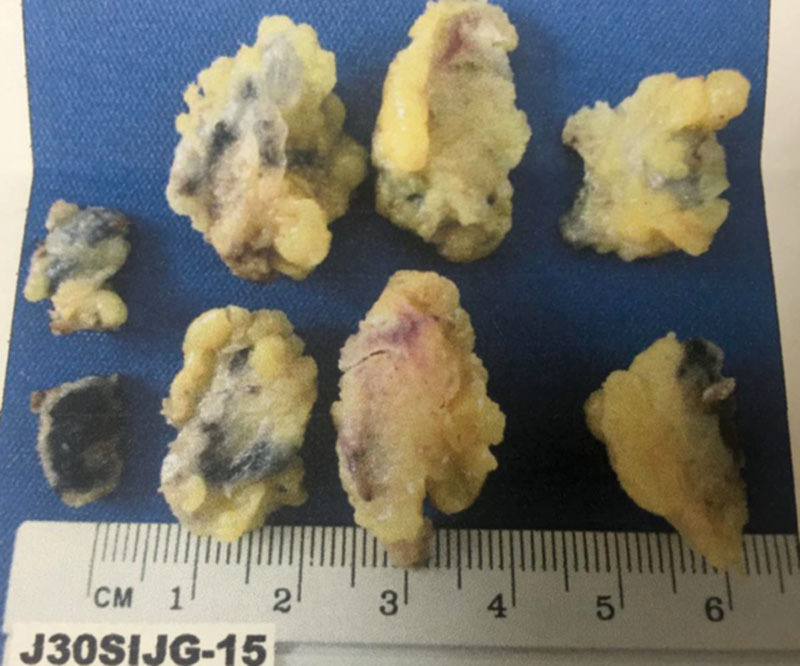
Macroscopic view of black pigmented lymph nodes varying from 2 to 3 cm in diameter.
DISCUSSION
Tattooing has become more popular with the passage of time. It is estimated that in the United States, 14% of all the population has at least 1 tattoo.2
Initially, ink particles were found within large phagosomes in the cytoplasm of both keratinocytes and phagocytic cells, including fibroblasts, macrophages, and mast cells. Tattoo particles were initially dispersed diffusely as fine granules in the upper dermis. In both amateur and professional tattoos, the depth of the pigment ink varies greatly, with a greater variability in size, shape, and location noted in amateur tattoos. Regardless of the diverse origins of tattoo pigments, the light microscopic and electron microscopic appearance of all pigments is similar, except for color.3
Tattoo ink is remarkably nonreactive histologically, despite the frequent use of different pigments of unknown purity and unknown identity by tattoo artists. Amateur tattoo inks consist of simple carbon particles, originating from burnt wood, cotton, plastic, or paper, or from a variety of inks, including India ink, pen ink, and vegetable matter. Although a rare occurence, red (mercury), yellow (cadmium), green (chromium), and blue (cobalt) tattoo pigments have elicited a persistent, localized allergic or photoallergic dermatitis and, more infrequently, systemic reactions. Interestingly, the colors (red and yellow) most commonly involved in allergic reactions often spontaneously disappear from a tattoo without clinical signs of a reaction.3
Tattoo pigment granules are composed of 3 kinds of loosely packed particles, ranging from 2 to 400 nm in diameter. The most common particle size is 40 nm, a particle size of 2 to 4 nm is less common (slightly more electron dense), and a particle size of 400 nm is the least common (high electron density with a crystalline structure). A study of freshly implanted eyeliner tattoo ink revealed a particle size of 0.1 to 1.0 μm in the extracellular matrix, although the average particle size in the pigment vial was 0.25 μm before implantation.4
Tail tattoo pigment, which is inert and nonpolarizable, can sometimes be found as aggregates of scattered brown/black material in the lymph nodes adjacent to the tattoo. Regional lymph node draining sites should always be inspected for the presence of exogenous pigments, the parent compound, or its metabolite, since it can sometimes localize in specific tissues in the body.
Any lymph node that is enlarged or with color changes should be examined. Beavis et al described the case of a 32-year-old woman with a vulvar squamous cell carcinoma and enlarged lymph nodes caused by tattoo pigment migration. And for that, they concluded that tattoo pigments should be considered in any patient with lymphadenopathy and regional tattoo.4 Kurle et al5 studied a patient with melanoma and pigmented lymph nodes. They state that clinical differentiation between tattoo pigments and metastatic disease within lymph nodes is not possible. Histological confirmation of an enlarged, pigmented lymph node is therefore essential before radical surgery is performed. Hence, data on accumulation of tattoo pigments within enlarged and pigmented lymph nodes need to be included into the differential diagnosis, and the documentation of decorative tattoos is important during skin-cancer screening and during the follow-up of melanoma patients.5
CONCLUSION
Although pigmented inguinal lymph nodes are not commonly seen in the plastic and reconstructive surgical patients, knowledge of their treatment should always be in mind. Because macroscopic differentiation between malignant and nonmalignant pathology cannot be done, dissection and pathology evaluation is recommended. Also, a good physical evaluation should always be done on surgical patients. We must always remember that patient safety comes first.
PATIENT CONSENT
The patient provided written consent for the use of her image.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Anthracosis. (n.d.) Segen's Medical Dictionary. 2011. Available at http://medical-dictionary.thefreedictionary.com/anthracosis. Accessed June 17, 2016. [Google Scholar]
- 2. http://tattooconnection.net/blog/statistics/. Accessed January 11, 2015.
- 3.Wu D, Linsmeier Kilmer S, Goldman MP. Tattoo lasers. Available at: http://www.ehow.com/how_8309305_reference-emedicine-articles.html. Accessed April 26, 2016. [Google Scholar]
- 4.Beavis A, Amneus M, Aoyama C, et al. Tattoo pigment lymphadenopathy mimicking metastasis in vulvar cancer. Obstet Gynecol. 2012;120:442–444. doi: 10.1097/AOG.0b013e3182583be2. [DOI] [PubMed] [Google Scholar]
- 5.Kürle S, Schulte KW, Homey B. [Accumulation of tattoo pigment in sentinel lymph nodes]. Hautarzt. 2009;60:781–783. doi: 10.1007/s00105-009-1843-9. [DOI] [PubMed] [Google Scholar]