

Abstract
Mammary analogue secretory carcinoma (MASC) is a recently described low-grade malignant tumor of the salivary glands, biologically and morphologically equivalent to secretory breast carcinoma. We give a brief overview of this new entity, including morphological, immunohistochemical, molecular-genetic, clinical, epidemiologic features, differential diagnosis, and outcome results.
Keywords: Salivary gland, carcinoma, mammary analogue, MASC
Definition: Mammary analogue secretory carcinoma (MASC) is a low-grade malignant tumor of salivary glands resembling secretory breast carcinoma, including histopathologic and immunohistochemical features and t(12;15)(p13;q25) translocation with ETV6-NTRK3 gene fusion. Besides the classic form, which accounts for more than 90% of all cases, there are genetic variants and clinically aggressive forms being are reported.
First description: MASC was first described and genetically defined by Alena Skálová et al. [1], who proposed the current term, and documented the similarity between the salivary and the secretory mammary carcinoma, also known as juvenile breast cancer. It has been generally accepted that the salivary gland and the mammary tumor are completely equivalent to each other as shown reproducibly by a number of histopathologic, immunohistochemical, cytogenetic, and molecular genetic features.
Microscopic features and preoperative diagnosis: Tumor typically presents as a well-circumscribed multilobulated mass, subdivided into smaller segments by fibrous septa [2]. Tumor cells have uniform round and vesicular nuclei with central nucleoli and eosinophilic pink vacuolated cytoplasm. These cells are arranged into microcystic, cribriform, tubular, papillary, follicular (thyroid like), or solid nests (Figure 1). Microscopic foci of invasion are often present, but the overall mitotic activity is low. Intraluminal secretions may be seen in the microcystic or tubular structures. Such material is usually mucicarmine, periodic acid-Schiff (PAS), and alcian blue positive. It also stains with antibodies to epithelial membrane antigen (EMA). The unique microscopic features of MASC can be also recognized cytologically by fine-needle aspiration biopsy [3,4].
FIGURE 1.
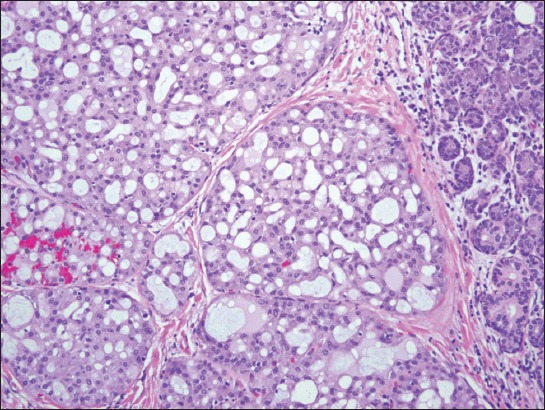
Mammary analogue secretory carcinoma (MASC) is composed of uniform cells with vesicular nuclei, centrally located nucleoli and well-developed eosinophilic cytoplasm. Cells are arranged in a cribriform manner or surround wider spaces that contain secretory material (Hematoxylin and eosin, x220).
Immunohistochemistry: As expected for carcinomas, tumor cells are positive for wide-spectrum cytokeratins (e.g. AE1/AE3, Cam5.2) and low-molecular weight cytokeratins (CK7, CK8, CK19). They are also positive for vimentin, S-100, mammaglobin, GCDFP-15, MUC1, GATA-binding protein 3, adipophilin, α-amylase, DOG-1, SOX-10, and p63 [1,2]. Using these IHC markers Urano et al. found some variations among the tumors and identified 3 histologic subtypes [5].
Genetics: Fluorescent in situ hybridization (FISH) analysis will demonstrate in most instances a t(12;15)(p13;q25) translocation with ETV6-NTRK3 gene fusion, which can be proven by means of molecular biology (e.g. RT-PCR). Cases without classical ETV6 gene rearrangement may harbor alternative gene rearrangements (“ETV6-X fusion”) that may be associated with more aggressive clinical course of the disease [6,7].
Differential diagnosis: Includes acinic cell carcinoma, mucoepidermoid carcinoma, and low-grade cribriform cystadenocarcinoma of the salivary gland.
Clinical course and outcome: MASC is most often found in the parotid glands, but it may occur in other glands including the minor salivary glands. In most instances the diagnosis of MASC carries a good prognosis and the neoplastic disease has an indolent clinical course [1,5,7]. Not all MASC have a good prognosis and a high-grade transformation followed by an accelerated clinical course and poor outcome has also been recorded in three patients [8]. Genetic analysis of tumors may identify tumors of a more aggressive nature [7].
Currently, no specific therapy is available for patients with MASC. Of note, Drilon et al. described a case with the patient with molecularly confirmed MASC that had a dramatic and clinically durable response to the targeted therapy with the pan-Trk inhibitor entrectinib (Ignyta) [9]. This drug has been shown to exhibit a potent in vitro activity against cell lines that contain various NTRK1/2/3 fusions. The patient developed resistance to the drug later in the course of the disease due to the NTRK3 G623R mutation.
Epidemiology: The true incidence of MASC is currently unknown due to its rarity and previous misclassification of this tumor type. Luk et al. found 9 MASC in a review of 190 malignant salivary gland tumors (~4.5%), whereas Majewska et al. found 7 MASC out of 183 cases (~4%) in a similar study [10,11]. MASC has a more or less equal distribution between men and women, in most studies showing slight (1.3 to 1.5) male predominance.
DECLARATION OF INTERESTS
The authors declare no conflict of interest.
REFERENCES
- 1.Skálová A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34:599–608. doi: 10.1097/PAS.0b013e3181d9efcc. DOI: 10.1097/PAS.0b013e3181d9efcc . [DOI] [PubMed] [Google Scholar]
- 2.Wenig BM. Atlas of head and neck pathology. 3rd ed. Philadelphia: Elsevier; 2016. [Google Scholar]
- 3.Oza N, Sanghvi K, Shet T, Patil A, Menon S, Ramadwar M, et al. Mammary analogue secretory carcinoma of parotid: is preoperative cytological diagnosis possible? Diagn Cytopathol. 2016. Mar 4, [Epub ahead of print]. http://dx.doi.org/10.1002/dc.23459 . [DOI] [PubMed]
- 4.Jung MJ, Kim SY, Nam SY, Roh JL, Choi SH, Lee JH, et al. Aspiration cytology of mammary analogue secretory carcinoma of the salivary gland. Diagn Cytopathol. 2015;43:287–93. doi: 10.1002/dc.23208. http://dx.doi.org/10.1002/dc.23208 . [DOI] [PubMed] [Google Scholar]
- 5.Urano M, Nagao T, Miyabe S, Ishibashi K, Higuchi K, Kuroda M. Characterization of mammary analogue secretory carcinoma of the salivary gland: discrimination from its mimics by the presence of the ETV6-NTRK3 translocation and novel surrogate markers. Hum Pathol. 2015;46:94–103. doi: 10.1016/j.humpath.2014.09.012. http://dx.doi.org/10.1016/j.humpath.2014.09.012 . [DOI] [PubMed] [Google Scholar]
- 6.Ito Y, Ishibashi K, Masaki A, Fujii K, Fujiyoshi Y, Hattori H, et al. Mammary analogue secretory carcinoma of salivary glands: a clinicopathologic and molecular study including 2 cases harboring ETV6-X fusion. Am J Surg Pathol. 2015;39:602–10. doi: 10.1097/PAS.0000000000000392. http://dx.doi.org/10.1097/PAS.0000000000000392 . [DOI] [PubMed] [Google Scholar]
- 7.Skálová A, Vanecek T, Simpson RH, Laco J, Majewska H, Baneckova M, et al. Mammary analogue secretory carcinoma of salivary glands: molecular analysis of 25 ETV6 gene rearranged tumors with lack of detection of classical ETV6-NTRK3 fusion transcript by standard RT-PCR: report of 4 cases harboring ETV6-X gene fusion. Am J Surg Pathol. 2016;40:3–13. doi: 10.1097/PAS.0000000000000537. http://dx.doi.org/10.1097/PAS.0000000000000537 . [DOI] [PubMed] [Google Scholar]
- 8.Skálová A, Vanecek T, Majewska H, Laco J, Grossmann P, Simpson RH, et al. Mammary analogue secretory carcinoma of salivary glands with high-grade transformation: report of 3 cases with the ETV6-NTRK3 gene fusion and analysis of TP53, β-catenin EGFR and CCND1 genes. Am J Surg Pathol. 2014;38:23–33. doi: 10.1097/PAS.0000000000000088. http://dx.doi.org/10.1097/PAS.0000000000000088 . [DOI] [PubMed] [Google Scholar]
- 9.Drilon A, Li G, Dogan S, Gounder M, Shen R, Arcila M, et al. What hides behind the MASC: clinical response and acquired resistance to entrectinib after ETV6-NTRK3 identification in a mammary analogue secretory carcinoma (MASC) Ann Oncol. 2016. Feb 15, p. mdw042. Epub ahead of print. http://dx.doi.org/10.1093/annonc/mdw042 . [DOI] [PMC free article] [PubMed]
- 10.Luk PP, Selinger CI, Eviston TJ, Lum T, Yu B, O’Toole SA, et al. Mammary analogue secretory carcinoma: an evaluation of its clinicopathological and genetic characteristics. Pathology. 2015;47:659–66. doi: 10.1097/PAT.0000000000000322. http://dx.doi.org/10.1097/PAT.0000000000000322 . [DOI] [PubMed] [Google Scholar]
- 11.Majewska H, Skálová A, Stodulski D, Klimková A, Steiner P, Stankiewicz C, et al. Mammary analogue secretory carcinoma of salivary glands: a new entity associated with ETV6 gene rearrangement. Virchows Arch. 2015;466:245–54. doi: 10.1007/s00428-014-1701-8. http://dx.doi.org/10.1007/s00428-014-1701-8 . [DOI] [PMC free article] [PubMed] [Google Scholar]