

Case
A healthy 30-year-old man spent a week on safari in Kenya in late February to early March. He received typhoid and yellow fever vaccines prior to his travel, and took atovaquone/proguanil for malaria prophylaxis while there. Three days after his return to the US, a red, papular rash appeared on his chest (Fig. 1), followed by fatigue, chills, sweats, and high fevers. He noticed a swollen lymph node in his left groin and a lesion on the anterior aspect of the left foot that was pustular, swollen, and painful. The rash on his chest spread to his groin, several new enlarged lymph nodes appeared in his neck, and the lesion on his foot progressed to a small eschar (Fig. 2).
Fig. 1.

Scattered erythematous papules on the chest.
Fig. 2.

Eschar on patient’s foot.
Initial labs were unremarkable. A rapid throat swab for Group A Streptococcus was negative as were cultures for Streptococcus Groups A, C, and G, Monospot test, HIV antibody/antigen, malaria and babesia smears, Lyme serology, and gonorrhea and chlamydia PCR. Rickettsial disease panel was positive for Rickettsia typhi IgG but not IgM. Further study resulted R. conorii IgG titer of 1:8192 and R. africae IgG titer of 1:1024.
A punch biopsy of the eschar revealed epidermal and superficial dermal necrosis with focal necrotizing vasculitis with a brisk superficial and deep lymphohistiocytic infiltrate suggestive of a tick-borne illness (Fig. 3, Fig. 4). Biopsy of the rash revealed similar vascular damage. The tissue was submitted to the Center for Disease Control and Prevention and R. africae was confirmed by PCR, supporting a diagnosis of African Tick Bite Fever (ATBF). The patient was treated with 10 days of doxycycline.
Fig. 3.
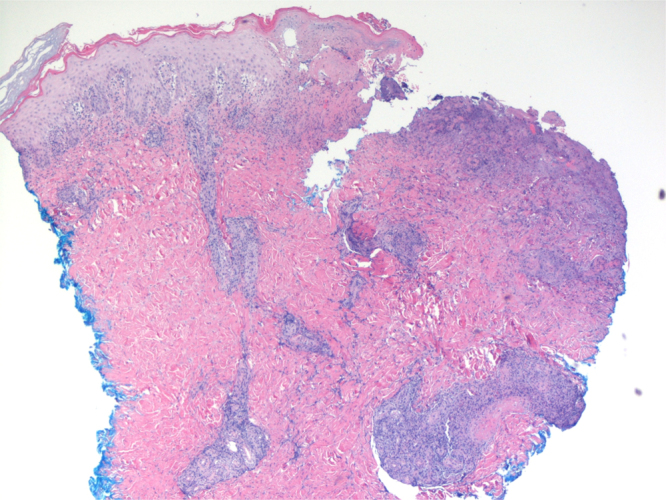
Area of epidermal and superficial dermal necrosis with underlying perivascular inflammation (40×).
Fig. 4.
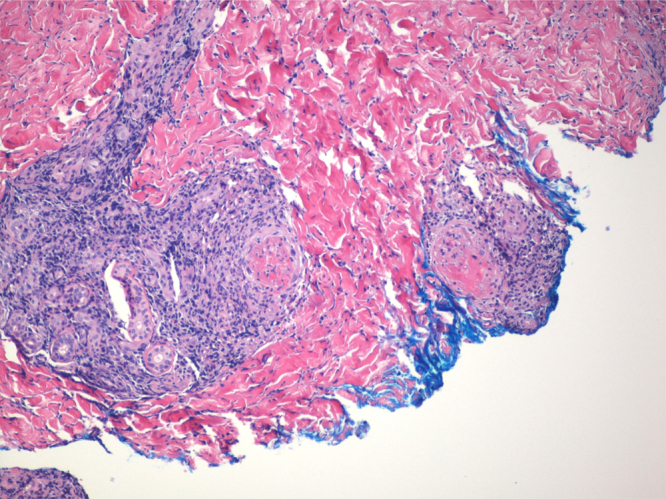
Fibrinoid necrosis of vessels with associated lymphohistiocytic inflammation (100×).
ATBF is a zoonotic disease caused by infection with R. africae and transmitted by Amblyomma ticks in sub-Saharan Africa [1], [2]. Common symptoms include fever, one or more inoculation eschars (tache noire), and regional lymphadenopathy. Rash is frequently absent and complications are uncommon [1], [2], [3]. The eschar can be the site of inoculation and rickettsial multiplication, making it the preferred biopsy site to distinguish ATBF from other rickettsioses due to cross-reactivity by immunofluorescence [1], [4], [5]. As seen in our case, positive rickettsial titers are reliable for infection with rickettsial disease, although unreliable for speciation. R. conorii is an important differential as it is also present in sub-Saharan Africa and cross reactions are common [4]. ATBF is an important diagnosis to consider when encountered with a fever in a traveler returning from sub-Saharan Africa.
Acknowledgements
Special thanks to Naomi Drexler and the Rickettsial Zoonoses Branch at the CDC.
References
- 1.Raoult D., Fournier P.E., Fenollar F., Jensenius M., Prioe T., de Pina J.J. Rickettsia africae, a tick-borne pathogen in travelers to sub-Saharan Africa. N Engl J Med. 2001;344(20):1504–1510. doi: 10.1056/NEJM200105173442003. [DOI] [PubMed] [Google Scholar]
- 2.Bohaty B.R., Hebert A.A. African tick-bite fever after a game-hunting expedition. New Engl J Med. 2015:e14. doi: 10.1056/NEJMicm1312910. [DOI] [PubMed] [Google Scholar]
- 3.Daneman N., Slinger R. Tache noire. Can Med Assoc J. 2008;178(7):p841. doi: 10.1503/cmaj.070102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lepidi H., Fournier P.E., Raoult D. Histologic features and immunodetection of African tick-bite fever eschar. Emerg Infect Dis. 2006;12(9):1332–1337. doi: 10.3201/eid1209.051540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Althaus F., Greub G., Raoult D., Genton B. African tick-bite fever: a new entity in the differential diagnosis of multiple eschars in travelers. Description of five cases imported from South Africa to Switzerland. Int J Infect Dis. 2010;14S:e274–e276. doi: 10.1016/j.ijid.2009.11.021. [DOI] [PubMed] [Google Scholar]