

Abstract
AIM
To evaluate the sensory characteristics of commercial bowel cleansing preparations.
METHODS
Samples of 4 commercially available bowel cleansing preparations, namely polyethylene glycol electrolyte solution (PEG), PEG + ascorbic acid (PEG-Asc), sodium picosulfate (SPS), and oral sodium sulfate (OSS) were prepared according to the manufacturer’s instructions. Descriptive analysis was conducted (n = 14) using a 15-cm line scale with the Compusense at-hand® sensory evaluation software. Acceptability testing (n = 80) was conducted using the 9-point hedonic scale. In addition, a Just-About-Right (JAR) scale was included for the four basic tastes to determine their intensity compatibility with acceptability levels in the products.
RESULTS
Samples were significantly different, in descriptive analysis, for all attributes (P < 0.05) except for sweetness. SPS received the highest ratings for turbidity, viscosity appearance, orange odor and orange flavor; PEG-Asc for citrus odor and citrus flavor; OSS for sweetener taste, sweet aftertaste, bitterness, astringency, mouthcoating, bitter aftertaste and throatburn, and along with PEG-Asc, the highest ratings for saltiness, sourness and adhesiveness. Acceptability results showed significant differences between the various samples (P < 0.05). SPS received significantly higher ratings for overall acceptability, acceptability of taste, odor and mouthfeel (P < 0.05). JAR ratings showed that PEG and PEG-Asc were perceived as slightly too salty; SPS and OSS were slightly too sweet, while SPS, PEG-Asc and OSS were slightly too sour and OSS slightly too bitter. While using small sample volumes was necessary to avoid unwanted purgative effects, acceptability ratings do not reflect the true effect of large volumes intake thus limiting the generalization of the results.
CONCLUSION
Further improvements are needed to enhance the sensory profile and to optimize the acceptability for better compliance with these bowel cleansing solutions.
Keywords: Laxatives, Acceptability, Sensory evaluation, Taste, Preparation, Colonoscopy
Core tip: Bowel preparation is an important quality indicator in colonoscopy. Purgative solutions are generally poorly tolerated and may serve as an impediment to colorectal cancer screening and surveillance. The need for rapid ingestion of these solutions is perceived as a major disadvantage concerning patient adherence as these solutions are often considered unpleasant. To date, no major studies have investigated the sensory properties of bowel cleansing solutions using comprehensive sensory evaluation techniques. This study showed major differences in sensory characteristics and the need for product development to optimize patient acceptability for better compliance with bowel cleansing solutions.
INTRODUCTION
Colonoscopy is the preferred screening method for colorectal cancer (CRC) due to its high diagnostic sensitivity and specificity. An adequate bowel preparation is crucial to perform a good colonoscopy exam. Bowel laxative preparations are generally poorly tolerated, disliked and as a result often serve as an impediment to CRC screening and surveillance. Patients who have had a colonoscopy often consider the bowel preparation as the worst part of their experience, and are, as a result, sometimes reluctant to undergo the procedure again or recommend it to others[1,2]. In addition, patients commonly experience adverse events of the bowel preparation, including bloating, nausea, vomiting and abdominal pain which may lead to interruption or incomplete adherence of the preparation. This may result in suboptimal bowel cleansing leading to incomplete examination, poor visualization of the mucosa, missed colon pathology, and possibly increased procedural complications and cost[3]. Despite the above, inadequate bowel preparation occurs surprisingly often and in as many as 25% of patients[4]. Predictors of an inadequate bowel preparation include medical factors like chronic constipation, use of opioids and tricyclics, diabetes mellitus, and obesity as well as other patient-related factors such as education, health literacy, and motivation[5]. Clearly, adherence with the prescribed laxative regimen including diet is an essential step to an effective bowel preparation. A recent study investigated the burden of the bowel preparation on pre-procedural quality of life by examining 7 variables including hunger, taste, volume, adverse events (AE), and the effect on sleep, social, and work functioning[6]. Except for work and AE, all variables scored negatively by greater than one fifth of patients (range 20.4-34.2). Overall, volume, taste, hunger, and sleep disturbances were considered the worst aspect of the preparation. To date, no major studies have investigated the sensory properties of bowel cleansing solutions using comprehensive sensory evaluation techniques. This may lead to a better understanding of the favorable and unfavorable characteristics of each preparation and provide a framework for comparing commercially available products and guide future development strategies.
MATERIALS AND METHODS
Sample preparation
Four commercial bowel cleansing laxative solutions namely polyethylene glycol electrolyte solution (PEG)-electrolyte + ascorbic acid (PEG-Asc, lime flavor, Moviprep®, Norgine, United Kingdom), PEG-electrolyte (PEG, no flavor, Fortrans® IPSEN, France), sodium picosulfate/magnesium citrate (SPS, orange flavor, Picoprep®, Ferring, Switzerland), and oral sodium sulfate (OSS, exotic fruits flavor, Izinova®, IPSEN, France) were used in the study. Samples were prepared according to manufacturer’s instructions: PEG-Asc, PEG, and SPS powdered samples were dissolved in mineral water; while OSS liquid sample was diluted to volume with mineral water.
Descriptive analysis
Descriptive analysis was conducted on the bowel cleansing solutions as described in previous studies[7]. The descriptive panel consisted of 14 judges (12 females and 2 males, age 19-26) recruited from the American University of Beirut. Panelists attended 4 one-hour training sessions during which a 15-cm unstructured line scale descriptive ballot was generated using 19 descriptive sensory attributes, anchor points and reference standards (Table 1). Subjects also attended 3 evaluation sessions over 3 d. All bowel cleansing solutions were prepared on the same day of training/evaluation sessions. Samples were evaluated in triplicates over 3 sessions with 4 samples per session using the Compusense at-hand® (Compusense Inc., Guelph, ON, Canada) sensory evaluation software. Serving sequence was randomized and counterbalanced based on William’s design for 4 treatments as generated by the software.
Table 1.
Terms used in the descriptive analysis of the bowel cleansing laxative solutions
| Attribute | Definition as worded on score sheet | Anchor words (low to high) |
| Appearance | ||
| Turbidity | The level of haze present in sample when holding the sample at eye level1 | Clear to turbid |
| Viscosity | The resistance to flow when swirling the sample in the cup2 | Thin to thick |
| Odor | ||
| Orange | Odor of orange juice3 | Not at all to very |
| Citrus | Odor of lemonade4 | Not at all to very |
| Flavor | ||
| Saltiness | Taste elicited by table salt | Not at all to very |
| Sweetness | Taste elicited by sugar (sucrose) | Not at all to very |
| Sourness | Taste elicited by citric acid | Not at all to very |
| Sweetener | Taste elicited by the sweetener solution5 | Not at all to very |
| Bitterness | Taste elicited by caffeine6 | Not at all to very |
| Orange | Flavor of orange juice3 | Not at all to very |
| Citrus | Flavor of lemonade4 | Not at all to very |
| Mouthfeel | Not at all to very | |
| Adhesiveness | The level of cling to surface of tongue when swirling sample in mouth | Not at all to very |
| Astringency | Dryness and puckering on tongue and palate6 | Not at all to very |
| Mouthcoating | Layer of sample left on palate after swallowing | Not at all to very |
| Aftertaste | Not at all to very | |
| Sweet | Aftertaste elicited by sugar solution | Not at all to very |
| Sour | Aftertaste elicited by citric acid solution | Not at all to very |
| Astringent | Dryness and puckering on tongue and palate after swallowing7 | Not at all to very |
| Bitter | Aftertaste elicited by caffeine solution6 | Not at all to very |
| Throatburn | Burn in throat after swallowing sample7 | Not at all to very |
Mineral water (low level), Rim, bottled at source by Rim Natural Spring Mineral Water SAL - Mount Sannine, Lebanon;
Mineral water, Rim, bottled at source by Rim Natural Spring Mineral Water SAL - Mount Sannine, Lebanon, for low level vs pineapple juice, Tropicana, bottled by société moderne Libanaise pour le commerce SAL, Beirut, Lebanon, for high level;
Orange juice (high level), Mr. Juicy, bottled by société moderne Libanaise pour le commerce SAL, Beirut, Lebanon;
Lemonade (high level), Balkis, Balkis SAL, Beirut, Lebanon;
Sweetener solution (high level), prepared by dissolving 2 tea spoons artificial sweetener (Sweet n low, Dietary foods, Soham Cambs, United Kingdom) in 500 mL mineral water;
Cold tea (high level), prepared by soaking 2 bags of black tea (Lipton, Unilever Mashreq tea company, New Borj El Arab, Alexandria, Egypt) in 500 mL hot mineral water, then cooled down to room temperature;
Baking soda solution (high level), prepared by dissolving 2 tea spoons of baking soda (Arm and Hammer, Harrison Street, Princeton New Jersey, United States) in 500 mL of mineral water.
Hedonic evaluation
An acceptability test was carried out by 80 untrained panelists (49 females and 31 males, age 18-28). Four samples were assessed in one session during which subjects rated overall acceptability, and acceptability of odor, taste and mouthfeel on a 9-point hedonic scale[8] ranging from 1 (dislike extremely) to 9 (like extremely) using the Compusense at-hand® (Compusense Inc., Guelph, ON, Canada) sensory evaluation software. In addition, a Just-About-Right (JAR) scale[8] (-3: too little, 0: just about right, 3: too much) was included for the basic tastes (saltiness, sweetness, sourness, and bitterness) to determine the compatibility of their intensity in the samples with optimum acceptability levels. Moreover, panelists were asked to identify any additional flavor perceived other than the four basic tastes. Serving sequence was randomized and counterbalanced based on William’s design for 4 treatments as generated by the software.
Statistical analysis
Analysis of variance using the GLM procedure of SPSS statistics for windows software (version 23, IBM Corporation, Armonk, NY, United States) was performed. In the statistical model for descriptive analysis, the response variable was the sensory attribute. Factors in the model included sample, panelist, replicate and their two-way interactions. Panelist was considered as random effect and sample and replicate were fixed effects. The sensory acceptability model did not include replicate. Significant means were separated by Tukey’s honestly significant difference (HSD) test. Significance was pre-established at α < 0.05.
RESULTS
Descriptive analysis
The analysis of variance results for the descriptive analysis are summarized in Table 2. As expected the panelist effect was significant for most attributes, with 12 out of the 19 attributes having a significant panelist effect (P < 0.05). Significant differences between samples were obtained for 18 out of the 19 attributes, specifically for turbidity, orange and citrus odors and flavors, saltiness, sourness, bitterness, astringency, sweet, sour, astringent, bitter aftertastes and throatburn (P < 0.001); adhesiveness, mouthcoating (P < 0.01) and viscosity-appearance and sweetener taste (P < 0.05). Replicate effect existed for only viscosity-appearance, citrus odor, sweetness and sweetener tastes (P < 0.05) indicating a high level of reliability. The same was true for sample × replicate interaction which was not significant for all attributes (P > 0.05). However, this was not the case for sample × panelist which was significant for many attributes (P < 0.05) and to a lesser extent for panelist × replicate. Means for the different samples are summarized in Table 3 and in Figure 1, which also include the level of significance for the different attributes. PEG-Asc had significantly higher ratings than other samples for citrus odor and flavor and adhesiveness (P < 0.05), which was not significantly different from OSS. PEG had significantly lower values for bitterness, astringency, sweet, sour and astringent aftertastes (P < 0.05). On the other hand, SPS had significantly higher values for turbidity, viscosity-appearance, orange odor and flavor, sourness and sour aftertaste (P < 0.05) while OSS had significantly higher values for sweetener taste, bitterness, astringency, mouthcoating, bitter, astringent aftertastes and throatburn (P < 0.05).
Table 2.
Significance of effects (F and P-values) for descriptive attributes for the bowel cleansing laxative solutions
| Attributes | Panelist (df = 13) | Sample1 (df = 3) | Replicate (df = 2) | S × P (df = 39) | R × P (df = 26) | S × R (df = 6) |
| Appearance | ||||||
| Turbidity | 5.6d | 9.1d | 3.1 | 1.4 | 1.5 | 0.5 |
| Viscosity | 5.4d | 4.2a | 4.5a | 1.5 | 1.7a | 0.1 |
| Odor | ||||||
| Orange | 2.0 | 15.9d | 0.0 | 2.3b | 0.4 | 1.3 |
| Citrus | 2.0 | 35.0d | 4.7a | 2.1b | 0.6 | 1.3 |
| Flavor | ||||||
| Saltiness | 2.9b | 8.8d | 0.7 | 2.7d | 1.3 | 0.9 |
| Sweetness | 6.3d | 2.8 | 5.3a | 5.7d | 1.2 | 0.8 |
| Sourness | 4.5d | 18.5d | 0.6 | 2.5d | 1.2 | 1.4 |
| Sweetener | 8.4d | 3.7a | 3.5a | 4.7d | 1.6 | 1.6 |
| Bitterness | 2.0 | 8.5d | 0.2 | 4.8d | 1.0 | 0.9 |
| Orange | 1.6 | 10.9d | 0.7 | 6.1d | 1.4 | 0.6 |
| Citrus | 1.3 | 11.4d | 2.3 | 3.7d | 1.2 | 0.7 |
| Mouthfeel | ||||||
| Adhesiveness | 4.8d | 4.3b | 1.3 | 3.9d | 2.0a | 1.4 |
| Astringency | 2.2a | 11.0d | 1.2 | 2.0b | 2.6b | 0.1 |
| Mouthcoating | 3.7d | 4.8b | 0.9 | 2.4d | 1.6 | 0.7 |
| Aftertaste | ||||||
| Sweet | 10.2d | 8.6d | 2.6 | 1.8a | 2.4d | 1.6 |
| Sour | 6.3d | 16.3d | 2.1 | 2.4d | 0.9 | 0.8 |
| Astringent | 1.3 | 9.1d | 2.1 | 2.4d | 2.1b | 0.9 |
| Bitter | 2.0 | 15.2d | 0.3 | 2.2d | 1.5 | 0.7 |
| Throatburn | 3.5b | 7.9d | 0.9 | 1.9b | 1.4 | 0.4 |
Bowel cleansing laxative solutions. P > 0.05 not significant (no superscript) vs
P < 0.05;
P < 0.01;
P < 0.001.
Table 3.
Least squares means of descriptive sensory attributes (rated on a 15 cm line scale) for the bowel cleansing laxative solutions
| Attribute |
Bowel cleansing laxative solution |
|||
| PEG-Asc (mean ± SD) | PEG (mean ± SD) | SPS (mean ± SD) | OSS (mean ± SD) | |
| Appearance | ||||
| Turbidity | 3.5 ± 2.3c | 2.9 ± 1.8c | 4.5 ± 2.4a | 2.8 ± 1.6c |
| Viscosity | 4.1 ± 2.7c | 3.5 ± 2.0c | 5.0 ± 2.8a | 3.8 ± 2.3c |
| Odor | ||||
| Orange | 3.1 ± 3.1c | 1.6 ± 0.4e | 5.8 ± 3.4a | 1.9 ± 1.4e |
| Citrus | 7.3 ± 3.7a | 1.5 ± 0.4e | 3.0 ± 2.3c | 2.2 ± 1.8ce |
| Flavor | ||||
| Saltiness | 6.0 ± 3.1a | 5.8 ± 3.2a | 2.8 ± 1.9c | 5.8 ± 3.4a |
| Sweetness | 3.8 ± 2.4 | 3.0 ± 1.9 | 4.1 ± 2.6 | 4.7 ± 3.4 |
| Sourness | 6.6 ± 3.0a | 2.5 ± 1.4c | 6.5 ± 3.2a | 6.9 ± 3.8a |
| Sweetener | 4.7 ± 3.5c | 3.5 ± 2.5e | 4.7 ± 3.4c | 5.6 ± 3.3a |
| Bitterness | 2.9 ± 1.9ce | 2.2 ± 1.7e | 3.2 ± 2.1c | 6.0 ± 4.2a |
| Orange | 3.2 ± 3.3c | 1.8 ± 0.9e | 6.3 ± 4.1a | 2.1 ± 2.0e |
| Citrus | 6.6 ± 3.9a | 1.9 ± 1.3e | 3.2 ± 2.6c | 3.0 ± 3.2ce |
| Mouthfeel | ||||
| Adhesiveness | 5.1 ± 2.6a | 3.7 ± 1.9c | 4.3 ± 2.2c | 5.4 ± 2.6a |
| Astringency | 4.4 ± 2.6c | 2.8 ± 2.0e | 4.5 ± 2.2c | 6.1 ± 3.4a |
| Mouthcoating | 4.7 ± 2.8c | 3.8 ± 2.3c | 4.3 ± 2.5c | 6.0 ± 3.2a |
| Aftertaste | ||||
| Sweet | 4.7 ± 3.2ac | 3.3 ± 2.3e | 4.5 ± 3.3c | 5.5 ± 3.3a |
| Sour | 5.1 ± 2.6a | 2.2 ± 1.4c | 5.9 ± 3.1a | 6.1 ± 3.9a |
| Astringent | 4.0 ± 2.2c | 2.6 ± 1.5e | 4.6 ± 2.6c | 5.9 ± 3.5a |
| Bitter | 2.4 ± 1.4c | 2.2 ± 1.7c | 2.8 ± 1.6c | 5.5 ± 3.7a |
| Throatburn | 3.5 ± 2.5ce | 2.8 ± 2.1e | 4.4 ± 2.8c | 5.7 ± 3.8a |
Means within each row with different superscripts are significantly different (P < 0.05).
Means within each row with different superscripts are significantly different (P < 0.05).
Means within each row with different superscripts are significantly different (P < 0.05).
PEG: Polyethylene glycol; PEG-Asc: PEG + ascorbic acid; SPS: Sodium picosulfate; OSS: Oral sodium sulfate.
Figure 1.
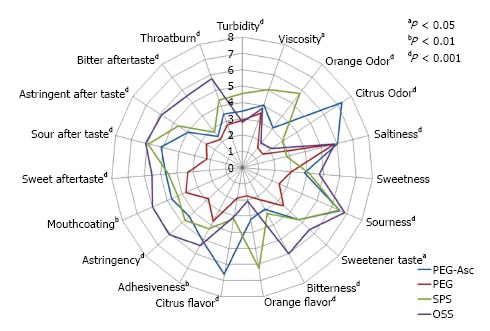
Sensory profiles for the 4 bowel cleansing laxative solutions. Individual attributes are positioned like the spokes of a wheel around a center (zero or not detected) point, with the spokes representing attribute intensity scales, with higher (more intense) values radiating outward. PEG: Polyethylene glycol; PEG-Asc: PEG + ascorbic acid; SPS: Sodium picosulfate; OSS: Oral sodium sulfate.
Hedonic evaluation
Acceptability ratings: The analysis of variance results for the acceptability test are summarized in Table 4. Panelist effect was significant for overall acceptability and the acceptability of mouthfeel (P < 0.001), taste (P < 0.01) but not for odor (P > 0.05). Significant differences between samples existed for overall acceptability and acceptability of taste, mouthfeel (P < 0.001) and odor (P < 0.01). The means of the acceptability variables are summarized in Table 5. SPS was significantly more liked for overall acceptability and the acceptability of taste and mouthfeel (P < 0.05) and although it obtained the highest rating for acceptability of odor, it was not significantly different from PEG-Asc or OSS.
Table 4.
Significance of effects (F and P-values) for acceptability attributes for the bowel cleansing solutions
| Attributes | Panelist (df = 79) | Sample1 (df = 3) |
| Overall Acceptability | 1.8d | 22.3d |
| Odor | 1.3 | 4.2b |
| Taste | 1.6b | 22.2d |
| Mouthfeel | 1.9d | 14.5d |
Bowel cleansing laxative solutions. P > 0.05 not significant (no superscript) vs aP < 0.05;
P < 0.01;
P < 0.001.
Table 5.
Least squares means of acceptability variables (rated using the 9-point hedonic scale) for the bowel cleansing laxative solutions
| Acceptability variable |
Bowel cleansing laxative solution |
|||
| PEG-Asc (mean ± SD) | PEG (mean ± SD) | SPS (mean ± SD) | OSS (mean ± SD) | |
| Overall acceptability | 3.8 ± 2.1c | 3.1 ± 1.6c | 5.5 ± 2.1a | 3.8 ± 2.4c |
| Odor | 5.5 ± 2.1ac | 4.9 ± 0.9c | 5.9 ± 1.8a | 5.5 ± 2.5ac |
| Taste | 3.5 ± 2.1c | 2.9 ± 1.6c | 5.1 ± 2.3a | 3.1 ± 2.2c |
| Mouthfeel | 4.2 ± 1.9c | 3.8 ± 1.7ce | 5.1 ± 2.0a | 3.4 ± 2.0e |
Means within each row with different superscripts are significantly different (P < 0.05).
Means within each row with different superscripts are significantly different (P < 0.05).
Means within each row with different superscripts are significantly different (P < 0.05).
PEG: Polyethylene glycol; PEG-Asc: PEG + ascorbic acid; SPS: Sodium picosulfate; OSS: Oral sodium sulfate.
Just about right ratings and sample flavor: The JAR scale ratings for the different samples on saltiness, sweetness, sourness and bitterness are illustrated in Figure 2. A high percentage of ratings in the -1 to +1 range is indicative of an optimum level of taste intensity to the liking of panelists while a high skew to lower or upper ratings is indicative of low or high intensity with respect to the liking of taste, respectively. SPS seems to be the best sample in terms of percentage of subjects who found it to have the optimal taste to their liking. This applied to all four tastes. PEG seemed to have a tilt for higher percentages of subjects who gave higher ratings for saltiness and sourness and the opposite was true for sweetness while a spread of percentages across all ratings for bitterness. PEG-Asc exhibited the same trends as PEG while OSS had a tilt for higher percentages of subjects who gave higher ratings for sweetness, sourness and bitterness. Table 6 summarizes the percentage of subjects who indicated the presence of a certain flavor in the different samples. It is clear, and expected, that none of the subjects noticed any flavor in the PEG sample. PEG-Asc, which is expected to have a lemon-citrus flavor, had only 28% of the subjects who indicated this flavor, while 60% did not indicate any and smaller percentages were given to other flavors, such as orange, fruity, strawberry, green tea and pomegranate. SPS, which is expected to have an orange flavor, also had 28% who indicated the above flavor, while 56% did not indicate any, 13% indicated lemon and 4% indicated fruity. OSS, which is expected to have tropical/exotic fruits, had 55% who did not indicate any flavor, 13% for strawberry, 10% for medicinal, 9% for bubble gum and smaller percentages for other flavors.
Figure 2.
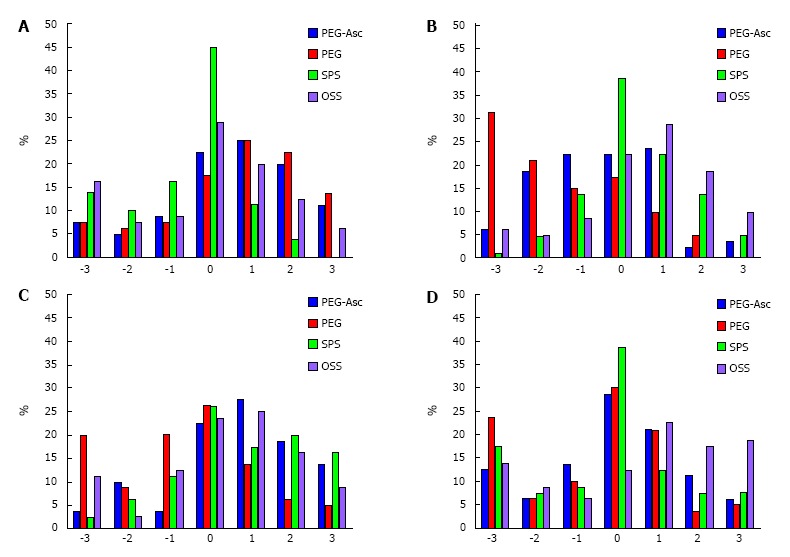
Just-About-Right ratings for saltiness (A), sweetness (B), sourness (C) and bitterness (D) for PEG-Asc (blue), PEG (red), SPS (green) and OSS (violet) samples. -3: Too little; 0: Just about right; 3: Too much; PEG: Polyethylene glycol; PEG-Asc: PEG + ascorbic acid; SPS: Sodium picosulfate; OSS: Oral sodium sulfate.
Table 6.
Percentage of participants’ responses to the additional flavor perceived in the different bowel cleansing laxative solutions
| Flavor |
Bowel cleansing laxative solution |
|||
| PEG-Asc | PEG | SPS | OSS | |
| None | 60% | 100% | 56% | 55% |
| Lemon | 28% | 0% | 13% | 1% |
| Orange | 6% | 0% | 28% | 1% |
| Strawberry | 1% | 0% | 0% | 13% |
| Bubble gum | 0% | 0% | 0% | 9% |
| Cherry | 0% | 0% | 0% | 5% |
| Medicinal | 0% | 0% | 0% | 10% |
| Mint | 0% | 0% | 0% | 1% |
| Green tea | 1% | 0% | 0% | 0% |
| Fruity | 3% | 0% | 4% | 4% |
| Pomegranate | 1% | 0% | 0% | 1% |
PEG: Polyethylene glycol; PEG-Asc: PEG + ascorbic acid; SPS: Sodium picosulfate; OSS: Oral sodium sulfate.
DISCUSSION
Our study is the first of its kind to analyze the sensory attributes of commercially available bowel preparations commonly used today in an effort to improve the understanding of patients’ taste preferences and acceptability of these different bowel cleansing solutions. The study describes 19 different sensory attributes, demonstrating a significant difference in 18 of the 19 under five major categories: Appearance, odor, flavor, mouthfeel and aftertaste. Additionally, our results demonstrated a significant difference of overall acceptability, taste, odor and mouthfeel assessment between the four cleansing solutions as rated on a 9-point hedonic scale.
Based on previous sensory descriptive studies[7], this study findings introduce a detailed description of the different sensory attributes that bowel cleansing solutions share. Cleansing solutions can be assessed based on appearance (turbidity and viscosity), odor and flavor (orange and citrus), basic tastes (saltiness, bitterness, sourness, sweetness), mouthfeel and aftertaste, characteristics that have not been fully described during palatability interpretation in the literature[9-14]. Our results demonstrate that characteristics such as orange and citrus odor/flavor and saltiness, sourness and bitterness are strongly noticeable and differentiated when consumed in a low volume, while other attributes such as sweetness are less differentiated. These descriptive analysis sample differences are indicative of the ease of differentiating between samples for panelists due to major differences in the sensory nature of samples. In addition, they can serve as a stepping-stone to create and improve more focused validated instruments aimed at assessing bowel-cleansing solutions. For example, and due to the lack of validated instruments to assess tolerability of bowel cleansing solutions[6], Patel et al[14] proposed the Mayo Clinic Bowel Prep Tolerability Questionnaire that, although comprehensive, only slightly touches on the aspect of taste by asking about the severity of bad taste bother during consumption.
Flavoring of bowel cleansing solutions is one of the techniques used to alter palatability and improve patient tolerability. Orange flavor and odor were significantly more noticeable in SPS compared to the three other solutions while citrus flavor and odor were significantly more noticeable in PEG-Asc compared to the three other solutions (Table 3). When sampled by 80 subjects and scaled on a 9 point hedonic scale, SPS (orange-flavored) was significantly more accepted in terms of overall acceptability, taste and mouthfeel compared to the three other samples. These results might indicate that orange and citrus flavors are more effective in improving palatability compared to other flavors. A recent study investigating the addition of 100% orange juice to 2 L PEG-Asc found that palatability scores were higher (2.36 ± 0.76 vs 1.78 ± 0.88; P = 0.005) when orange juice was added, as was willingness to repeat the same process[9]. This effect was hypothesized to be due to the intense sourness which offsets the bitter taste of PEG solutions, and the fact that orange juice was kept in the mouth for 5 s prior to solution intake[9]. Similarly, the addition of citrus reticulate peel to conventional low dose PEG + bicasodyl demonstrated higher taste acceptability and lower rates of difficulty swallowing when compared to PEG + bicasodyl regimen[10]. Again, citrus peel was required to stay in the mouth in between solution consumption every 10-15 min. A study by Sharara et al[12] investigated the role of sugar free menthol drops used with 4 L split dose PEG regimen. Patients instructed to suck on the candy while drinking the solution had significantly higher palatability score and increased willingness to take the same preparation in the future (92% vs 80%; P = 0.091) compared to PEG without menthol[12]. This regimen was also found to be superior to reduced volume PEG-Asc, in terms of palatability (76% vs 62%; P = 0.03) and willingness to retake the solution compared to low volume PEG-Asc (54% vs 40%; P = 0.047)[13]. Of interest, 1 L of pineapple juice demonstrated no change in patient-rated tolerability when added to 4 L and 2 L PEG respectively and compared to each other as well as PEG[11].
One interesting observation is the low percentage of study participants who correctly perceived the flavor of the solutions tested. While SPS was deemed the most acceptable overall -taste-, odor- and mouthfeel-wise-, only 28% of participants picked up on the orange taste, while 56% indicated that the solution had no flavor. Similarly, only 28% of participants detected lemon flavor in PEG-Asc samples while 60% indicated that the solution had no flavor. Similar results were also true for OSS. Only PEG was correctly perceived to have no flavor in 100% of the cases. This could indicate the possibility that higher flavor concentrations or different flavor ingredients are required in order to make the solutions taste and smell closer to the original attributes marketed. Another possibility for the discordance between marketed and perceived taste could be due to the mechanism of flavor introduction and taste alteration. Menthol drops for example were kept in the mouth during solution intake instead of being dissolved in an attempt to flavor the solution itself[12]. Similarly in the citrus study, citrus peel was kept between the tongue and hard palate every 10-15 min in between solution intake and was not swallowed or mixed with the solution[10]. Pineapple juice however was dissolved in the entire solution volume of 2 L and 4 L[11] and could have resulted in a dilution effect, compromising the intensity and palatability. The mechanism of action of the former two interventions could have more effectively affected taste transduction leading to significant improvement in palatability, a possibly crucial observation that can add to future clinical trials and introduce a new and different approach to manufacturers manipulating cleansing solution taste for an improved palatability.
Our study has few limitations. It was conducted at a single center with volunteers as panelists thus limiting the generalizability of the results. The study focuses on taste and palatability assessment, thus using a small sample volume of cleansing solution which does not reflect the true effect of large volume intake in real settings. In a previous study investigating the burden of bowel preparation in patients undergoing colonoscopy, patients reported that volume is considered one of the worst aspects of bowel preparation[6]. Using small volume samples might have masked some taste aversions that would otherwise have occurred with larger or repeated ingestions[6]. However, our use of small volumes was necessary to avoid the unwanted purgative effects that would have invariably occurred. Unlike colonoscopy patients who are required to follow dietary restrictions, panelists in our study had no such additional burden that may impact tolerability and possibly allowing more room for observational error and variation in the ability to differentiate and properly rate the sensory attributes under investigation. Low volume split-dose SPS regimens for example are associated with increased hunger secondary to longer dietary restrictions and modifications[6] that also add to the burden and tolerability of bowel cleansing consumption when taken under realistic measures.
In summary, our study is the first to assess different sensory attributes in regards to bowel cleansing solutions. While previous literature has focused on overall tolerability and willingness to retake solution as a marker for improved palatability, our study introduces taste, odor, flavor and other attributes that interplay in affecting overall tolerability. Sensory evaluation results revealed that SPS (orange flavored) bowel cleansing solution was the most palatable and tolerable by the subjects. The use of a JAR scale and spider plot illustrating the different attributes of each solution is an important visual aid for consumers and physicians, allowing for better customization of a bowel cleansing solution tailored to patients’ personal preference. Shedding light on noticeable attributes other than taste and flavor, as well as different mechanisms of taste alteration could also aid bowel cleansing solution manufacturers in the process of product development and lead to new and better modified bowel cleansing.
ACKNOWLEDGMENTS
The authors would like to thank Hani Chaar (PharmD) and Roy Nassif for technical assistance; Soraya Ghantous and Sara Issa for assistance with subjects’ recruitment.
COMMENTS
Background
Bowel preparation is an important quality indicator in colonoscopy. Patient adherence can be poor given that these solutions are often considered unpleasant.
Research frontiers
Evaluating the sensory characteristics of commercial bowel cleansing preparations is necessary to optimize consumer acceptability for better compliance with pre-colonoscopy procedures.
Innovations and breakthroughs
Sodium picosulfate (SPS, orange flavored) preparation received higher acceptability ratings than other commercial bowel cleansing solutions, with an optimal level of taste acceptability for saltiness, bitterness and sweetness. SPS might be associated with better palatability and tolerability among other solutions.
Applications
Orange flavored bowel cleansing solutions appear to be more palatable and tolerable by panelists than bland or other flavored preparations.
Peer-review
This is an interesting article that presents novel data on the palatability of various bowel preparations.
Footnotes
Institutional review board statement: The study protocol was reviewed and approved by the American University of Beirut Institutional Review Board on June 29, 2015 and the study was registered with clinicaltrial.gov identifier: NCT02642783.
Informed consent statement: All study participants provided written informed consent for descriptive analysis and verbal consent for hedonic evaluation.
Conflict-of-interest statement: The authors declare that there is no conflict of interest.
Data sharing statement: No additional data available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Unsolicited manuscript
Specialty type: Gastroenterology and hepatology
Country of origin: Lebanon
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): 0
Grade C (Good): C, C
Grade D (Fair): 0
Grade E (Poor): 0
Peer-review started: January 18, 2016
First decision: February 22, 2016
Article in press: May 9, 2016
P- Reviewer: Belsey J, Sakin YS S- Editor: Gong ZM L- Editor: A E- Editor: Lu YJ
References
- 1.Burke CA, Church JM. Enhancing the quality of colonoscopy: the importance of bowel purgatives. Gastrointest Endosc. 2007;66:565–573. doi: 10.1016/j.gie.2007.03.1084. [DOI] [PubMed] [Google Scholar]
- 2.Dykes C, Cash BD. Key safety issues of bowel preparations for colonoscopy and importance of adequate hydration. Gastroenterol Nurs. 2008;31:30–35; quiz 36-37. doi: 10.1097/01.SGA.0000310933.54551.ca. [DOI] [PubMed] [Google Scholar]
- 3.Johnson DA, Barkun AN, Cohen LB, Dominitz JA, Kaltenbach T, Martel M, Robertson DJ, Richard Boland C, Giardello FM, Lieberman DA, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2014;109:1528–1545. doi: 10.1038/ajg.2014.272. [DOI] [PubMed] [Google Scholar]
- 4.Sharara AI, Abou Mrad RR. The modern bowel preparation in colonoscopy. Gastroenterol Clin North Am. 2013;42:577–598. doi: 10.1016/j.gtc.2013.05.010. [DOI] [PubMed] [Google Scholar]
- 5.Rex DK. Bowel preparation for colonoscopy: entering an era of increased expectations for efficacy. Clin Gastroenterol Hepatol. 2014;12:458–462. doi: 10.1016/j.cgh.2013.11.003. [DOI] [PubMed] [Google Scholar]
- 6.Sharara AI, El Reda ZD, Harb AH, Abou Fadel CG, Sarkis FS, Chalhoub JM, Mrad RA. The burden of bowel preparations in patients undergoing elective colonoscopy. United Eur Gastroent. 2016;4:314–318. doi: 10.1177/2050640615594550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Srour N, Daroub H, Toufeili I, Olabi A. Developing a carob-based milk beverage using different varieties of carob pods and two roasting treatments and assessing their effect on quality characteristics. J Sci Food Agric. 2016;96:3047–3057. doi: 10.1002/jsfa.7476. [DOI] [PubMed] [Google Scholar]
- 8.Lawless HT, Heymann H. 2nd ed. Berlin: Springer Science and Business Media; 2010. Sensory evaluation of food: principles and practices; pp. 325–344. [Google Scholar]
- 9.Choi HS, Shim CS, Kim GW, Kim JS, Lee SY, Sung IK, Park HS, Kim JH. Orange juice intake reduces patient discomfort and is effective for bowel cleansing with polyethylene glycol during bowel preparation. Dis Colon Rectum. 2014;57:1220–1227. doi: 10.1097/DCR.0000000000000195. [DOI] [PubMed] [Google Scholar]
- 10.Lan HC, Liang Y, Hsu HC, Shu JH, Su CW, Hung HH, Hou MC, Lin HC, Lee SD, Wang YJ. Citrus reticulata peel improves patient tolerance of low-volume polyethylene glycol for colonoscopy preparation. J Chin Med Assoc. 2012;75:442–448. doi: 10.1016/j.jcma.2012.06.022. [DOI] [PubMed] [Google Scholar]
- 11.Altınbas A, Aktas B, Yılmaz B, Ekiz F, Deveci M, Basar O, Simsek Z, Coban S, Tuna Y, Uyar MF, et al. Adding pineapple juice to a polyethylene glycol-based bowel cleansing regime improved the quality of colon cleaning. Ann Nutr Metab. 2013;63:83–87. doi: 10.1159/000354094. [DOI] [PubMed] [Google Scholar]
- 12.Sharara AI, El-Halabi MM, Abou Fadel CG, Sarkis FS. Sugar-free menthol candy drops improve the palatability and bowel cleansing effect of polyethylene glycol electrolyte solution. Gastrointest Endosc. 2013;78:886–891. doi: 10.1016/j.gie.2013.05.015. [DOI] [PubMed] [Google Scholar]
- 13.Sharara AI, Harb AH, Sarkis FS, Chalhoub JM, Badreddine R, Mourad FH, Othman M, Masri O. Split-dose menthol-enhanced PEG vs PEG-ascorbic acid for colonoscopy preparation. World J Gastroenterol. 2015;21:1938–1944. doi: 10.3748/wjg.v21.i6.1938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Patel M, Staggs E, Thomas CS, Lukens F, Wallace M, Almansa C. Development and validation of the Mayo Clinic Bowel Prep Tolerability Questionnaire. Dig Liver Dis. 2014;46:808–812. doi: 10.1016/j.dld.2014.05.020. [DOI] [PubMed] [Google Scholar]