

Abstract
Background:
Despite recent restrictions being placed on practice in college football, there are little data to correlate such changes with injuries.
Hypothesis:
Football injuries will correlate with a team’s exposure to full-contact practice, total practice, and total games.
Study Design:
Descriptive epidemiological study.
Methods:
All injuries and athlete injury exposures (AE × Min = athletes exposed × activity duration in minutes) were recorded for an intercollegiate football team over 4 consecutive fall seasons. Weekly injuries and injury rates (injuries per athletic injury exposure) were correlated with the weekly exposures to full-contact practices, total practices, formal scrimmages, and games.
Results:
The preseason practice injury rate was over twice the in-season practice injury rate (P < 0.001). For preseason, injury exposures were higher for full-contact practice (P = 0.0166), total practices (P = 0.015), and scrimmages/games (P = 0.034) compared with in-season. Preseason and in-season practice injuries correlated with exposure to full-contact practice combined with scrimmages for preseason (P < 0.008) and full-contact practice combined with games for in-season (P = 0.0325). The game injury rate was over 6 times greater than the practice injury rate (P < 0.0001). Concussions constituted 14.5% of all injuries, and the incidence of concussions correlated with the incidence of all injuries (P = 0.0001). Strength training did not correlate with injuries.
Conclusion:
Decreased exposure to full-contact practice may decrease the incidence of practice injuries and practice concussions. However, the game injury rate was over 6 times greater than the practice injury rate and had an inverse correlation with full-contact practice.
Keywords: football, injuries, injury exposures, concussions
College football has one of the highest injury rates in intercollegiate athletics and accounts for the largest number of physician assessments in college athletics.27,28,45,47 In 1905, with the influence of President Theodore Roosevelt, the rules of football were changed to reduce injuries.12,35,38 This movement to limit injuries led to the creation of the National Collegiate Athletic Association (NCAA).12,35,38 The NCAA has continued to revise the rules of play, including recent restrictions on practice sessions to further reduce injuries.2,14,15,31,37,44
Particularly in response to the concern with concussion, full-contact practice has been limited by 1 conference since 2011, and the NCAA recommended a nationwide limitation in 2014.6,31,34,37,39 While it is intuitive that decreased full-contact practice will decrease practice injuries, there are conflicting data whether subsequent game injuries may be effected.2,15
A potential risk factor for injury in sports is the number of athlete exposures to practices and games, and particularly, the type of practice.3-5,7,13,20,23-26,30 Prior studies have documented injury rates based on preseason versus in-season, practice versus game, and by player position.8,15-18,27,40,41,46 In women’s basketball, rugby, soccer, and Australian football, there have been reports correlating the weekly volume of training to injuries.3,7,9-11,20,23-26,40,42
The purpose of this study was to record the weekly volume of training for a college football team with attention to minutes spent in practice, full-contact practice, strength training, and games and then to correlate these measures of injury exposure to the weekly toll of injuries. The hypothesis was that practice and game injuries would be related to injury exposures.
Methods
The study was approved by the university’s institutional review board. No information identifying specific players was recorded in the study’s database. Over 4 consecutive fall football seasons (2009-2012), the volume of training and injuries were collected for 1 Division I Football Championship Subdivision (FCS) NCAA intercollegiate football team.
Injuries
Injury data were recorded daily by the athletic training staff using a computerized system (SportsWare). All injured players were evaluated by the athletic training staff and a team physician within 1 day of injury. Injuries and the number of days missed from practice and games were recorded when there was at least 1 day of absence from full athletic participation. If an injury would have prevented participation after the end of the season, the time to return to participation was estimated. Injuries were classified as severe when they prevented participation for at least 10 days.
Full-Contact Practice, Total Practice, and Formal Scrimmage/Game Exposures
Formal team activities were recorded daily by the football athletic training staff. For each practice, the number of athletes present and the minutes devoted to each type of practice activity were recorded. Injury exposure was based on the number of athletes present multiplied by the minutes devoted to an activity. This was recorded as athletes exposed (AE) multiplied by the minutes (Min), or AE × Min.
Athlete exposures for preseason scrimmages were analyzed as a game activity. Scrimmages were assigned minutes of exposure based on the number of athletes present and the activity duration.
Strength Training
Strength training was a separate activity from practices or games. These sessions were conducted after a short practice. Strength training sessions lasted up to 60 minutes. Strength training was not considered as an injury exposure activity.
Athlete Exposures
Athlete exposures to injury, expressed as AE × Min, were calculated weekly for 3 activities: full-contact practice,48 total practice (calisthenics, instructional drills, and full-contact practice), and scrimmages or games. Full-contact practice was included within total practice but was also recorded separately. Preseason scrimmages were evaluated as game activities. To evaluate for a possible cumulative effect of training, athlete exposures were also calculated for the combinations of total practice plus scrimmages or games and full-contact practice plus scrimmages or games.
Data and Statistical Analysis
The practice injury rate for each week was calculated based on practice injuries divided by the total practice athlete exposures for the week. The game injury rate for each week was calculated based on game injuries divided by the game athlete exposures for the same week.
The numbers of injuries, injury rates, and athlete exposures between preseason and in-season were compared using either Student t tests or Wilcoxon rank sum tests. For the Wilcoxon test, significance was assessed using the normal approximation 2-sided P value. The Shapiro-Wilk test was used to test for normality. P values ≤0.05 were reported as significant.
Comparisons of injury rates for successive injuries to the same individual and for injury type were performed using general linear models. The chi-square test was used to analyze the proportion of players with 1 or more injuries in a particular year.
Results
Injury Types and Distribution
The number of injuries per year fluctuated from a low of 54 in 2011 to a high of 85 in 2010 (Table 1). Injuries to the lower extremity were most common, constituting 50% of all injuries. The proportion of injuries to other anatomic areas was 21% for the head/neck, 15% for the upper extremity, and 14% for the trunk/back. Injuries were attributed to contact with another player in 59% of cases, noncontact in 32% of cases, and an unknown mechanism in 9% of cases.
Table 1.
Injuries per year
| Player Injury Incidence | 2009 | 2010 | 2011 | 2012 | % of Total Players |
|---|---|---|---|---|---|
| 1 injury/year | 40 | 42 | 19 | 35 | 36 |
| 2 injuries/year | 13 | 17 | 7 | 12 | 11 |
| 3 injuries/year | 3 | 3 | 7 | 2 | 3 |
| 4 injuries/year | 0 | 0 | 0 | 1 | <1 |
| Total injuries/year | 75 | 85 | 54 | 69 | |
| Total players on roster | 110 | 110 | 110 | 110 |
Injuries were equally distributed between offensive and defensive players. The proportion of injuries was highest in defensive backs (19%), defensive lineman (18%), and offensive lineman (15%).
Overall, 70% of injuries were designated as acute and 30% were recurrent. Recurrence of an acute injury in the same season was observed in less than 2% of cases.
Players With Multiple Injuries in 1 Season
The proportion of players in a given season who sustained at least 1 injury was 50.7% (Table 1). The incidence of a second injury in the same season to a previously injured player was 32.3%. The incidence of a third injury in the same season to a player with 2 prior injuries was 33%. Only 1 player had 4 injuries in a single season.
Practice Injuries
All metrics for injury exposures were significantly greater during preseason than in-season excluding strength training (Table 2 and Figure 1). The increased injury exposures during preseason compared with in-season constituted 43.7% more practice (P < 0.0001) and 77.9% more full-contact practice (P < 0.0001).
Table 2.
Preseason versus in-season injury exposures per weeka
| Injury exposures | Preseasonb | In-season | P |
|---|---|---|---|
| Practice | 54.0 ± 19.4 | 37.8 ± 5.4 | 0.0150 |
| Full-contact practice | 12.5 ± 5.5 | 7.9 ± 2.3 | 0.0166 |
| Game | 10.7 ± 6.2c | 9.1 ± 3.9 | 0.0334 |
| Full-contact practice + game | 25.1 ± 11.1 | 17.1 ± 4.4 | 0.0076 |
| Practice + game | 64.7 ± 19.5 | 46.9 ± 5.0 | 0.0160 |
| Strength training | 13.9 ± 4.9 | 14.2 ± 2.5 | 0.8963 |
| Practice + game + strength training | 78.8 ± 16.6 | 61.0 ± 4.5 | 0.0034 |
Data presented as AE x Min / 1000 ± SD.
Data presented for full weeks of preseason.
Preseason games were formal scrimmages.
Figure 1.
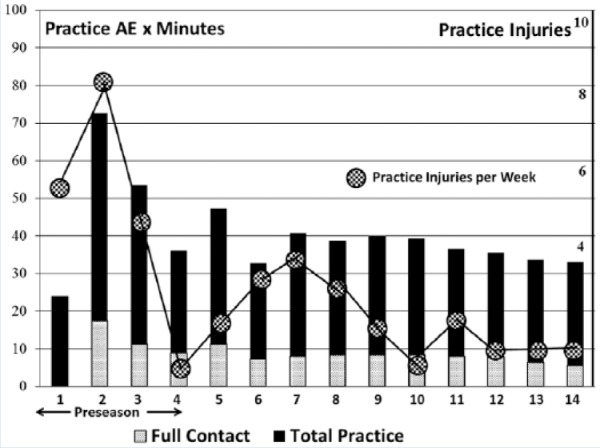
Practice injuries and practice injury exposures. The 4-year mean practice injury exposures (AE × minutes/ 1000) are noted by the bars for each week of the season, with the proportion devoted to full-contact practice shown within the total practice bar. The 4-year mean weekly practice injuries are indicated by the spheres. AE, athletes exposed.
Preseason practice injuries correlated with the full-contact practice + scrimmage injury exposures (P < 0.008) (Table 3 and Figure 1). In-season practice injuries also correlated with full-contact practice + game injury exposures (P = 0.0325) and game injury exposures (P = 0.0276).
Table 3.
Practice injuries with injury exposures (correlation coefficients)
| Injury Exposures | Preseason Practice Injuries | In-season Practice Injuries | ||
|---|---|---|---|---|
| Practice | 0.475 | P = 0.119 | 0.003 | P = 0.984 |
| Full-contact practice | 0.450 | P = 0.142 | 0.065 | P = 0.689 |
| Game | 0.037 | P = 0.909 | 0.348 | P = 0.028 |
| Full-contact practice + game | 0.726 | P = 0.008 | 0.339 | P = 0.033 |
| Practice + game | 0.484 | P = 0.111 | 0.273 | P = 0.088 |
| Strength training | −0.548 | P = 0.065 | −0.104 | P = 0.524 |
| Practice + game + strength training | 0.421 | P = 0.173 | 0.242 | P = 0.132 |
Preseason practice injury rates (practice injuries per practice athlete exposures) correlated with full-contact practice + scrimmage injury exposures (correlation coefficient, 0.701; P = 0.0110). Similarly, in-season practice injury rates correlated with the full-contact practice + game injury exposures (correlation coefficient, 0.429; P < 0.0057) and with game injury exposures (correlation coefficient, 0.476; P < 0.0019).
Game Injuries
Preseason game (scrimmage) injuries did not correlate with measurements of injury exposure (Table 4 and Figure 2). In-season game injuries only correlated with game injury exposures (P = 0.026) (Table 4 and Figure 2).
Table 4.
Scrimmage or game injuries and injury exposures (correlation coefficients)
| Injury Exposures | Preseason Scrimmage Injuries | In-season Game Injuries | ||
|---|---|---|---|---|
| Practice | −0.066 | P = 0.838 | −0.166 | P = 0.307 |
| Full-contact practice | 0.099 | P = 0.760 | −0.135 | P = 0.407 |
| Game | 0.396 | P = 0.202 | 0.351 | P = 0.026 |
| Full-contact practice + gamea | 0.315 | P = 0.318 | 0.231 | P = 0.151 |
| Practice + gamea | 0.059 | P = 0.854 | 0.093 | P = 0.570 |
| Strength training | −0.010 | P = 0.974 | −0.099 | P = 0.544 |
| Practice + gamesa + strength training | 0.077 | P = 0.812 | 0.046 | P = 0.776 |
Scrimmages for preseason.
Figure 2.
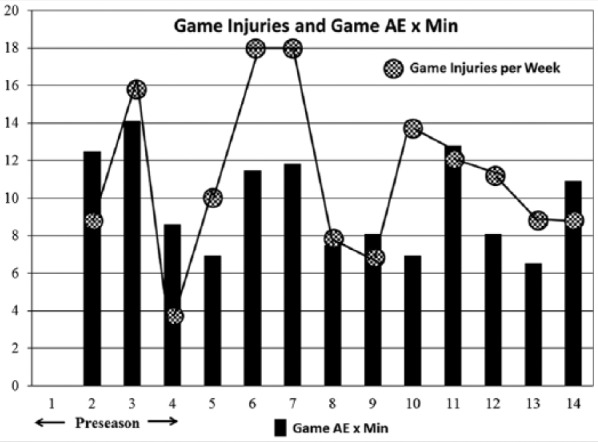
Game injuries and game injury exposures. The 4-year mean weekly game injury exposures (AE × minutes/1000) are noted by the vertical bars for each week of the season. The 4-year mean weekly game injuries are indicated by the spheres. AE, athletes exposed.
Game injury rates (game injuries per game athlete exposures) did not correlate with measurements of injury exposure during preseason or in-season. While not statistically significant, there was again a negative or inverse relationship between full-contact practice and the game injury rate for both preseason (P = 0.530) and in-season (P = 0.368).
Practice Versus Game Injury Rates
Overall, 48.8% (138) of injuries occurred during practice and 51.2% (145) occurred during games. The practice injury exposures over 4 years were 2229.4 AE x Min / 1000 and the game injury exposures were 492.49 AE x Min / 1000. Practices contributed 81.9% of injury exposures and resulted in 48.8% of injuries. Games contributed 18.1% of injury exposures and resulted in 51.2% of injuries. The practice injury rate per week was 0.052 injuries per AE x Min/1000 (95% CI, 0.039-0.065). The game injury rate per week was over 6 times greater at 0.317 injuries per AE x Min/1000 (95% CI, 0.254-0.380). The difference in injury rates between practices and games was significant (P < 0.0001).
Severe Injuries and Surgeries
Overall, 49.6% of injuries were classified as severe because they prevented participation for at least 10 days. Practices contributed 50.8% of severe injuries and games contributed 49.2% of severe injuries. There were between 8 and 12 surgeries per year for football-related injuries, with an average of 9.8 per year.
Concussions
Over the 4 years, there were 41 concussions, which constituted 14.5% of all injuries. The number of concussions per year was variable, and there was not a trend over the study (Table 5). The average time lost per concussion was 29.2 days, and this did not demonstrate a trend over the 4 years.
Table 5.
Concussions
| Preseason Practice | In-season Practice | Preseason Scrimmages | In-season Games | Total | |
|---|---|---|---|---|---|
| 2009 | 0 | 0 | 0 | 2 | 2 |
| 2010 | 3 | 1 | 2 | 7 | 13 |
| 2011 | 4 | 1 | 0 | 3 | 8 |
| 2012 | 4 | 6 | 3 | 5 | 18 |
| Total | 11 | 8 | 5 | 17 | 41 |
| Percent of Total | 27 | 20 | 12 | 41 |
Forty-six percent of concussions occurred during practice (Figure 3). There was a significant correlation between the incidence of concussions per week and the incidence of all injuries per week (correlation coefficient, 0.505; P = 0.0001) (Table 6).
Figure 3.
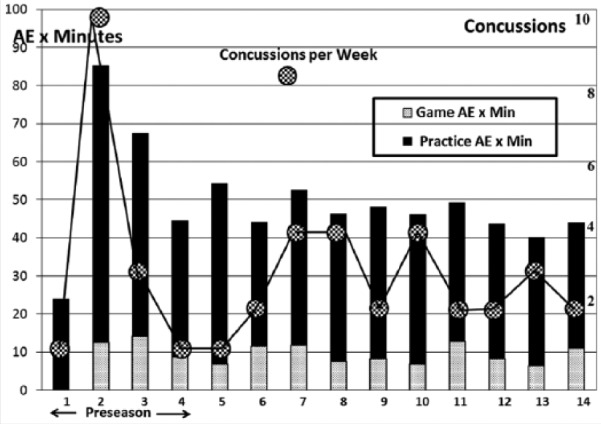
Concussion and injury exposures. The 4-year mean weekly game and practice injury exposures (AE × minutes/1000) are noted by the vertical bars for each week of the season. Total weekly concussions for the 4 years of the study are indicated by the spheres. AE, athletes exposed.
Table 6.
Concussions and injury exposures (correlation coefficients)
| Injury Exposures | Practice Concussions (n = 19) | Game Concussions (n = 21) | ||
|---|---|---|---|---|
| Practice | 0.303 | P = 0.0273 | −0.075 | P = 0.5969 |
| Full-contact practice | 0.512 | P = 0.0001 | 0.066 | P = 0.6398 |
| Game | 0.102 | P = 0.4683 | 0.061 | P = 0.6666 |
| Full-contact practice + gamea | 0.462 | P = 0.0005 | 0.126 | P = 0.3730 |
| Practice + gamea | 0.325 | P = 0.0177 | −0.051 | P = 0.7171 |
| Strength training | −0.205 | P = 0.1417 | 0.040 | P = 0.7764 |
| Practice + gamea + strength training | 0.289 | P = 0.0355 | −0.034 | P = 0.8122 |
Scrimmages for preseason.
Discussion
This study of one NCAA Division I football team recorded injuries and injury exposures weekly to evaluate the incidence of injuries in relation to training activities. Prior studies of football have not made correlations between weekly injuries and weekly injury exposures.1,2,15-19,21,27,33,36,38,40,41,44,46 The hypothesis was that practice type would contribute to injuries.
Injuries were due to contact with another player in 59% of cases, noncontact in 32% of cases, and due to an unidentified mechanism in 9% of cases. Seventy percent of injuries were acute and 30% were recurrent, with less than 2% recurrent in the same season. There are no comparative data for the acuity of injuries.
An average of 50.7 players were injured in any 1 season. Of this group, approximately one-third would have a second injury and approximately one-third of players with 2 injuries would have a third injury. Statistically, there was no trend for 1 injury to predispose a player to a subsequent injury in a given year.
The game injury rate was over 6 times greater than the practice injury rate, similar to other reports.18,21,27,36,41,44
Preseason exposure to full-contact practice and scrimmages significantly correlated with practice injuries (P = 0.008). In-season exposures to full-contact practice and games significantly correlated with practice injuries (P = 0.033). One implication of these findings is that athletes are affected by increased full-contact whether in practice or in games, and it leaves them vulnerable to practice injuries. Strength training did not correlate with practice injuries.
The incidence of concussions in practice correlated with full-contact practice (P = 0.0001). No correlations were identified between concussions occurring in games and injury exposures (Figure 3).
The present study has documented increased practice injuries when exposure to full-contact practice was combined with scrimmages or games. This would suggest that decreasing full-contact practice might decrease practice injuries. Interestingly, the present study also documented a trend for increased game injuries with decreased full-contact practice. These findings underscore the challenge of decreasing injuries by regulating practice type. An intervention may have unforeseen results.
One league and now the entire NCAA has responded to concussions by decreasing full-contact in both preseason and in-season practices.29,31,37,43 In the current study, concussions occurred in the same pattern as all injuries.
The major weakness of the current study is that it is an observational and not an interventional study and included only one college football team. The correlations are post hoc–observed associations and they may not reflect cause-and-effect relationships and may not be generalizable. The strength of the study is its rigorous recording of all injuries and injury exposures.4,22,32
Conclusion
Full-contact practice and scrimmages in preseason (P = 0.008) and full-contact practice and games during inseason (P = .033) contributed to practice injuries. There were no such associations with game injuries. Strength training did not contribute to injuries. Concussions had an injury pattern that was similar to the injury pattern for all injuries.
Acknowledgments
We acknowledge Sarah E. Steiner for her development of the data processing system.
Footnotes
The following authors declared potential conflicts of interest: Mark E. Steiner, MD, is a paid consultant for, and has patents and royalties from, Stryker Orthopedics; Greg Elia, MD, has received fees for participation in review activities from New England Baptist Research Department. The authors acknowledge and thank DonJoy Orthopedics for research funding, which made this project possible.
References
- 1. Adickes MS, Sturart MJ. Youth football Injuries. Sports Med. 2004;34:201-207. [DOI] [PubMed] [Google Scholar]
- 2. Albright JP, Powell JW, Martindale AI, et al. Injury patterns in Big Ten Conference football. Am J Sports Med. 2004;32:1394-1404. [DOI] [PubMed] [Google Scholar]
- 3. Anderson L, Triplett-McBride T, Foster C, et al. Impact of training patterns on incidence of illness and injury during a women’s collegiate basketball season. J Strength Cond Res. 2003;17:734-738. [DOI] [PubMed] [Google Scholar]
- 4. Bahr R, Holme I. Risk factors for sports injuries—a methodological approach. Br J Sports Med. 2003;37:384-392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bengtsson H, Ekstrand J. Match injury rates in professional soccer vary with match result, match venue, and type of competition. Am J Sports Med. 2013;41:1505-1510. [DOI] [PubMed] [Google Scholar]
- 6. Booher M, Wisniewski J, Smith B, Sigurdsson A. Comparison of reporting systems to determine concussion incidence in NCAA Division I collegiate football. Clin J Sport Med. 2003;13:93-95. [DOI] [PubMed] [Google Scholar]
- 7. Brink M, Visscher C, Arends S, Zwerver J, Post W, Lemmink K. Monitoring stress and recovery: new insights for the prevention of injuries and illnesses in elite youth soccer players. Br J Sports Med. 2010;44:809-815. [DOI] [PubMed] [Google Scholar]
- 8. Broglio SP, Martini D, Kasper L, Eckner J, Kutcher J. Estimation of head impact exposure in high school football. Am J Sports Med. 2013;41:2877-2884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Brooks JH, Fuller CW, Kemp SP, Reddin DB. A prospective study of injuries and training amongst the England 2003 Rugby World Cup squad. Br J Sports Med. 2005;39:288-293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Brooks JH, Fuller CW, Kemp SP, Reddin DB. Epidemiology of injuries in English professional rugby union: part 1 match injuries. Br J Sports Med. 2005;39:757-766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Brooks JH, Fuller CW, Kemp SP, Reddin DB. Epidemiology of injuries in English professional rugby union: part 2 training injuries. Br J Sports Med. 2005;39:767-775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Camp W. Football: Facts and Figures. New York, NY: Harper & Brothers; 1894. [Google Scholar]
- 13. Chalmers DJ, Samaranayaka A, Gulliver P, McNoe B. Risk factors for injury in rugby union football in New Zealand: a cohort study. Br J Sports Med. 2012;46:95-102. [DOI] [PubMed] [Google Scholar]
- 14. Crisco J, Fiore R, Beckwith J, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45:549-559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dagiau RF, Dillman CJ, Milner EK. Relationship between exposure time and injury in football. Am J Sports Med. 1980;8:257-260. [DOI] [PubMed] [Google Scholar]
- 16. DeLee JC, Farney WC. Incidence of injury in Texas high school football. Am J Sports Med. 1992;20:575-580. [DOI] [PubMed] [Google Scholar]
- 17. Dick R, Agel J, Marshall SW. National Collegiate Athletic Association Injury Surveillance System commentaries: introduction and methods. J Athl Train. 2007;42:173-182. [PMC free article] [PubMed] [Google Scholar]
- 18. Dick R, Ferrara MS, Agel J, et al. Descriptive epidemiology of collegiate men’s football injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:221-233. [PMC free article] [PubMed] [Google Scholar]
- 19. Dragoo JL, Braun HJ, Durham JL, Chen MR, Harris AH. Incidence and risk factors for injuries to the anterior cruciate ligament in National Collegiate Athletic Association football. Am J Sports Med. 2012;40:990-995. [DOI] [PubMed] [Google Scholar]
- 20. Dupont G, Nedelec M, McCall A, McCormack D, Berthoin S, Wisløff U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am J Sports Med. 2010;38:1752-1758. [DOI] [PubMed] [Google Scholar]
- 21. Feeley BT, Kennelly S, Barnes RP, et al. Epidemiology of National Football League training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36:1597-1603. [DOI] [PubMed] [Google Scholar]
- 22. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40:193-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Gabbett TJ. Reductions in pre-season injury exposures reduce training injury rates in rugby league players. Br J Sports Med. 2004;38:743-749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Gabbett TJ. Influence of training and match intensity on injuries in rugby league. J Sports Sci. 2004;22:409-417. [DOI] [PubMed] [Google Scholar]
- 25. Gabbett T, Domrow N. Relationships between injury exposures, injury, and fitness in sub-elite collision sport athletes. J Sports Sci. 2007;25:1507-1519. [DOI] [PubMed] [Google Scholar]
- 26. Gabbett T, Jenkins D. Relationship between injury exposures and injury in professional rugby league players. J Sci Med Sports. 2011;14:204-209. [DOI] [PubMed] [Google Scholar]
- 27. Hagel BE, Fick GH, Meeuwisse WH. Injury risk in men’s Canada West University football. Am J Epidemiol. 2003;157:825-833. [DOI] [PubMed] [Google Scholar]
- 28. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42:311-319. [PMC free article] [PubMed] [Google Scholar]
- 29. Kerr ZY, Yeargin S, Valovich McLeod TC, et al. Comprehensive coach education and practice contact restriction guidelines result in lower injury rates in youth American football. Orthop J Sports Med. 2015;3:2325967115594578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Killen N, Gabbett T, Jenkins D. Injury exposures and incidence of injury during preseason in professional rugby league players. J Strength Cond Res. 2010;24:2079-2084. [DOI] [PubMed] [Google Scholar]
- 31. Kim J, Skorton D. Report Regarding the Ivy League Review of Concussions in Football. Princeton, NJ: The Council of Ivy League President; 2011. [Google Scholar]
- 32. King D, Gabbett T, Gissane C, Hodgson L. Epidemiological studies of injuries in rugby league: suggestion for definitions, data collection and reporting methods. J Sci Med Sport. 2009;12:12-19. [DOI] [PubMed] [Google Scholar]
- 33. Meyers MC. Incidence, mechanisms, and severity of game-related college football injuries on fieldturf versus natural grass. Am J Sports Med. 2010;38:687-697. [DOI] [PubMed] [Google Scholar]
- 34. Mihalik J, Bell D, Marshall S, Guskiewicz K. Measurement of head impacts in collegiate football players: an investigation of positional and event-type differences. Neurosurgery. 2007;61:1229-1235. [DOI] [PubMed] [Google Scholar]
- 35. Miller J. The Big Scrum. New York, NY: HarperCollins; 2011. [Google Scholar]
- 36. NCAA Datalys Center. Football injuries, data from the 2004/05–2008/09 seasons. http://www.datalyscenter.org/2c35cffbe2_sites/datalyscenter.org/files/NCAA_Football_Injury_WEB_1_.pdf. Accessed August 8, 2015.
- 37. NCAA Sports Science Institute. New guidelines aim to improve student-athlete safety. http://www.ncaa.org/about/resources/media-center/news/new-guidelines-aim-improve-student-athlete-safety. Accessed August 8, 2015.
- 38. Nichols E, Richardson F. Football injuries of the Harvard football squad for three years under the revised rules. Boston Med Surg J. 1909;2:33-38. [DOI] [PubMed] [Google Scholar]
- 39. Pop Warner Football. Rule changes regarding practice and concussion prevention. http://www.popwarner.com/About_Us/Pop_Warner_News/Rule_Changes_Regarding_Practice___Concussion_Prevention_s1_p3977.htm. Accessed August 8, 2015.
- 40. Prager BI, Fitton WL, Cahill BR, Olson GH. High school football injuries: a prospective study and pitfalls of data collection. Am J Sports Med. 1989;17:681-685. [DOI] [PubMed] [Google Scholar]
- 41. Ramirez M, Schaffer K, Shen H, Kashani S, Kraus JF. Injuries to high school football athletes in California. Am J Sports Med. 2006;34:1147-1158. [DOI] [PubMed] [Google Scholar]
- 42. Rogalski B, Dawson B, Heasman J, Gabbett T. Training and game loads and injury risk in elite Australian footballers. J Sci Med Sports. 2013;16:499-503. [DOI] [PubMed] [Google Scholar]
- 43. Rowson S, Duma S, Greenwald R. Can helmet design reduce the risk of concussion in football. J Neurosurg. 2014;120:919-922. [DOI] [PubMed] [Google Scholar]
- 44. Shankar PR, Fields SK, Collins CL, Dick RW, Comstock D. Epidemiology of high school and collegiate football injuries in the United States, 2005-2006. Am J Sports Med. 2007;35:1295-1303. [DOI] [PubMed] [Google Scholar]
- 45. Steiner ME, Quigley DB, Wang F, Balint C, Boland AL. Team physicians in college athletics. Am J Sports Med. 2005;33:1545-1551. [DOI] [PubMed] [Google Scholar]
- 46. Thompson N, Halpern B, Curl WW, et al. High school football injuries: evaluation. Am J Sports Med. 1987;15:117-124. Erratum in: Am J Sports Med 1987;15: 257. [DOI] [PubMed] [Google Scholar]
- 47. Thorndike A., Jr Athletic Injuries: Prevention, Diagnosis and Treatment. Philadelphia, PA: Lea & Febiger; 1938:20-49. [Google Scholar]
- 48. USA Football. Heads up football. http://usafootball.com/headsup. Accessed August 8, 2015.