

Abstract
Objective
Adolescents living in Israel and the Palestinian authority are exposed to political violence. This review examines psychosocial risk factors for posttraumatic stress disorder (PTSD) organized within an ecological framework.
Method
Relevant articles were identified through PubMed and PsycINFO. Studies measuring risk and/or protective factors for PTSD in the Palestinian and/or Israeli adolescent populations due to conflict exposure from 1990 to present were included.
Results
A total of 20 studies met inclusion criteria. Greater violence exposure, poor economic resources, living in rural compared to urban areas, poor family and peer relations and poor coping skills were associated with PTSD symptoms.
Conclusions
The ecological framework is a useful approach to understanding factors affecting adolescent PTSD. Future research should focus on socio-ecological levels that have received limited attention.
Keywords: adolescence, posttraumatic stress disorder, Arab Israelis, Jewish Israelis, political violence
The violent struggles that have beset Kashmir, Sri Lanka and the Democratic Republic of the Congo are prototypical examples of prolonged conflicts. These conflicts are intense, durable, violent, and involve persistent intergroup confrontations. Civilians repeatedly exposed to violence can experience long-lasting severe mental health consequences that include heightened anxiety, reduced sense of safety, posttraumatic stress symptoms, and a subjective sense of insecurity (Canetti, Hall, Rapaport, & Wayne, 2015; Galea et al., 2002; Lavi & Solomon, 2005; Veling, Hall, & Joosse, 2013).
There is little question that the century old Israeli-Palestinian conflict is one of the deepest and most prolonged conflicts. It is protracted, violent, perceived as zero-sum, and imposes high material and psychological demands on both sides (Bar-Tal, 2000). Political violence has left thousands of casualties and wounded on both the Israeli and Palestinian sides. Violence has occasionally peaked, for example during the First Intifada (1987-1996) and again during the Second Intifada (2000-2004). During this period, the conflict saw its most violent confrontations, resulting in more than 13,000 terrorist attacks throughout Israel (Spilerman & Stecklov, 2013). The political violence that took place during this period had profound psychological effects on adolescents (Pat-Horenczyk et al., 2009).
The most common psychological disorder studied following terrorism is posttraumatic stress disorder (PTSD) (Galea et al., 2002; Hobfoll et al., 2011). The DSM-IV, the nosology used during the Second Intifada period, characterized symptoms of PTSD into three main categories; the first involves ‘reliving’ the event, in which the individual often experiences flashbacks, memories or nightmares. The second category involves avoidance, which is inclusive of feelings of detachment or emotional ‘numbing’ as well as avoiding places, people or thoughts that remind the individual of the event. The third category is arousal, which includes, for example, difficulty concentrating, hyper-vigilance or irritability. These symptoms must last more than one month to qualify for a clinical diagnosis of PTSD (American Psychiatric Association, 2013). Chronic exposure to political violence is different than acute exposure in the nature of its accumulative effects and is associated with increased PTSD (Buka, Stichick, Birdthistle, & Earls, 2001; Nuttman-Shwartz & Shoval-Zuckerman, 2015).
The effect of chronic political violence extends beyond the psychiatric toll and has a detrimental cost to society. Ecological models are useful in identifying these impacts as well as the potentially modifiable risk and protective factors that can be incorporated into intervention strategies for prevention and treatment of PTSD (World Health Organization [WHO], 2013). Glass and McAtee (2006) provide a model that incorporates both social and biological processes within a life-course perspective to shed light on how the social and structural environment plays a role in the development of ill physical and mental health. It is useful to apply this model to adolescent populations exposed to ongoing trauma given its developmental perspective. Specifically, this model outlines multilevel determinants of health situated on the global, macro, mezzo, micro and individual levels. Below we discuss how social ecology is affected by political violence, is involved in normal adolescent development, and how chronic exposure to political violence can disrupt this development.
At an upstream global-level, political violence can erode governments' ability to take coordinated actions to promote public health (Zwi & Ugalde, 1991). At a macro- level, chronic exposure to violence can destroy roads and community infrastructure and weaken economies. For example, political violence can lead to financial consequences caused by elevated rates of hospitalization and healthcare utilization (Deykin et al., 2001; Hidalgo & Davidson, 2000; Kalia, 2002; Zlotnick et al., 1999). At the community level, schools and hospitals can be destroyed, and erosion of social capital can ensue following the decline in local, state and provincial authorities ability to provide aid. At micro-levels, family violence can increase following chronic trauma exposure (Osofsky, 1999). At the individual level, chronic trauma is associated with reduced self-esteem, self-concept, and poor academic attainment among adolescents (Buka et al., 2001; Herrenkohl et al., 2000).
Adolescence is a critical period of physical, cognitive and social development. Chronic exposure to political violence may disrupt normative development and lead to lasting neurocognitive, psychosocial, and psychiatric consequences (Blum, Astone, Decker, & Mouli, 2014). Chronic trauma exposure is disruptive to adolescents' social context, which may affect normative development. One potential pathway is through an influence on parents and parenting practices. Some parents might need help learning how to cope with their child's trauma, as they are likely to experience feelings of guilt and sadness. Some parents might themselves be traumatized, which can affect adolescents' mental health. A recent meta-analysis of 32 studies showed that parents' PTSD symptoms are associated with increased symptoms in children (Morris, Gabert-Quillen, & Delahanty, 2012). Chronic trauma exposure can also affect biological systems and brain development during adolescence, which is a stage of neural plasticity, leading to increased risk-taking behavior and poor coping with emotional stressors (Taylor, 2010). Few studies have explored the effects of traumatic stress in adolescence on behavior, hypothalamic-pituitary-adrenal (HPA) axis function and the relative vulnerability to PTSD in adulthood (Li et al., 2015).
Adolescence is a period of development where the foundations for disease and health are laid for the future. It is a risk-prone period where risk and protective factors should be recognized early in order to provide meaningful direction for programmatic and policy approaches to bolster positive youth and adult development (Giacaman, Shannon, Saab, Arya, & Boyce, 2007).
We chose to study PTSD in adolescents due to significant gaps in the literature about risk and protective factors within the context of ongoing political violence. It is clear that not all who are exposed to chronic violence experience these deleterious outcomes. Therefore, understanding the role of potentially modifiable risk and protective mechanisms for this population is needed, especially within an ecological framework.
The framework allows for both universal as well as cultural elements to be incorporated in our understanding of PTSD, It better contextualizes the disorder vis –à- vis Palestinian and Israeli adolescent populations (Van Rooyen & Nqweni, 2012). Israelis and Palestinians differ in a number of ways, including in terms of the accessibility and availability of financial resources and healthcare services, their behavioral adaptation to stress, and the quality of their social networks and support. We would expect to see different risk and protective factors in these populations based on culture, religion and their accessibility to resources (Al-Krenawi, Graham, & Kanat-Maymon, 2009; Elbedour, Onwuegbuzie, Ghannam, Whitcome, & Hein, 2007; Thabet, Ibraheem, Shivram, Winter, & Vostanis, 2009). Systematically evaluating the variation between populations may lead to insights that could inform interventions uniquely designed to address the needs of each of these populations.
The goal of the current systematic review is to identify the contributions related to the development of posttraumatic symptomology among Palestinian and Israeli adolescents by using a socioecological framework to explore the various risk and protective factors for PTSD at each ecological level. We focus on multi-level systems that develop as a result of prolonged exposure to particular environments such as armed conflict, where social and external factors become internalized, or get ‘under the skin’ (Glass & McAtee, 2006). Our review will enable comparisons of the resources available to each of these groups that may influence the development of PTSD, as well as identify gaps in knowledge regarding potential ecological influences.
Method
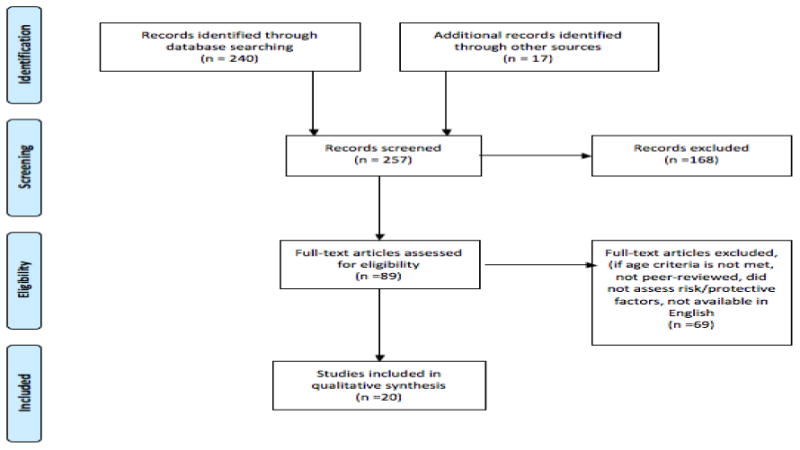
An electronic literature search was conducted using Medline/PubMed, ERIC, and PsycInfo databases. Our team consulted a research librarian to select and define the search terms. Titles and abstracts were retained in an Endnote Library. Search terms were generated using medical subject headings (MeSH for PubMed) and a thesaurus for PsycInfo including: “Adolescent*”, “adolescence” or “youth” or “teen*” and “PTSD”, “posttraumatic stress disorder” or “posttraumatic” or “post-traumatic” or “anxiety disorder*” or “mental disorder*” or “distress” in combination with “Israel” or “Israeli*” or “Jew*” and/or “Palestinian*” or “Arab*” in combination with “war” or “trauma” or “exposure” or “conflict” or “violence” or “terror*” or “political” in combination with “risk factor*” or “protective factor*” or “resilience*” or “factor*” in combination with “prevalence” or “incidence” or “determinant*” or “psychosocial”. The initial search identified 257 articles. Titles and abstracts were reviewed for terms representing psychosocial risk factors of either population due to conflict exposure. One study author (YR) screened the studies titles and abstracts and another author (BJH) reviewed these screened studies. The full text of the remaining articles were reviewed for by authors (YR and BJH), decisions regarding paper omissions were made independently, and discrepancies were discussed. Articles that included adults and adolescents were retained, as long as the adolescent population could be clearly delineated in the paper. In conclusion, a total of 168 were omitted. A total of 89 papers were further assessed for eligibility. Reference lists of articles that were deemed acceptable for inclusion were carefully reviewed to identify additional articles of relevance. Authors of all relevant articles were contacted via electronic mail in order to collect papers that were possibly under review or in press and, therefore, were not yet indexed or available online.
We included articles that were published from the year 1990 to the present year in order to comprehensively evaluate the literature related to the rise in political violence and tensions due to the First and Second Intifada. We referred to violence as the intentional use of physical force or power that results in the high likelihood of injury or psychological harm as defined by the WHO Violence Prevention Alliance (WHO, 2015), and focused this review on political violence exposures that resulted from war and terrorism. We included studies in this review if they (1) specified the adolescent population as being between age 10 and 19 years old (defined by the World Health Organization) (WHO, 2013), (2) examined psychosocial risk and protective factors for PTSD in the Palestinian and/or Israeli populations and (3) assessed either risk or protective factors related to conflict exposure and, (4) were available in the English language. Articles were excluded if they came from book chapters, dissertations, conference proceedings or brief reports, if they did not fit the age criteria, or if they were not available in English (see Figure 1, supplemental materials).
Figure. 1. Electronic databases, search results, number of articles used and reference numbers.
Risk and protective factors were evaluated as they fit within the socioecological model, which is divided into five interconnected levels comprising the global, macro, mezzo, micro and individual levels (Glass & McAtee, 2006) (see Tables 1, 2 and 3). The global-level is comprised of geopolitical, economic and environmental dynamics. The macro-level relates to national and state dynamics. The mezzo-level focuses on work-sites, schools, communities and healthcare. The micro-level focuses on groups, family and social networks. The individual-level focuses on characteristics of the individual related to cognitive development, temperament and personality traits.
Table 1. Nine primary research studies focused on Palestinian adolescents.
| Study | Setting | Sample characteristics | Methods | Significant results | Non-significant results |
|---|---|---|---|---|---|
| Al-Krenawi, J. Graham, 2012 | Gaza and the West Bank | 971 adolescents 42% boys and 57% girls 521 adolescents from the West Bank and 450 from the Gaza strip Ages 14-18 |
Cross-sectional Self-reported Participants were from randomly selected schools from refugee camps, villages and major cities in both Gaza and the West Bank, through the ministries of education Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Greater political violence exposure MEZZO: N/A MICRO: INDIVIDUAL: female sex Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: Higher family economic status INDIVIDUAL: N/A |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: Parents' education INDIVIDUAL: Nationality and religion |
| Dubow et al., 2010 | West Bank (64% of the sample) and Gaza Strip 36% of the sample) | 600 adolescents 200 8 year olds (101 girls and 99 boys), 200 11 year olds (100 girls and 100 boys) and 200 14 year olds (100 girls and 100 boys) |
Longitudinal Representative sample Diagnostic interview and self-reported Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Living in Gaza compared to West Bank; greater political conflict/violence MEZZO: Greater exposure of school conflict/violence MICRO: family conflict/violence INDIVIDUAL: N/A Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: male sex, older age |
GLOBAL: N/A MACRO: N/A MEZZO: community conflict/violence MICRO: parent education and income INDIVIDUAL: no significant interactions between sex or age and ecological level of exposure, or political violence and ecological level of exposure |
| Elbadour et al. 2007 | The Rafah and Kan-Younis Refugee camps in the southern region of the Gaza Strip | 229 adolescents Of the 229 adolescents, 52.8% were boys Ages 15-19 |
Cross-sectional Diagnostic interview and self-reported Randomized sampling using a 2 –stage procedure Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Low levels of seeking guidance and support coping, higher depression and anxiety Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Positive reappraisal coping |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: coping styles of logical analysis, problem solving, cognitive avoidance, acceptance or resignation, and emotional discharge |
| Khamis, 2005 | East Jerusalem and various governorates in the West Bank | 1000 adolescents 52.3% were boys and 47.7% were girls Ages 12-16 |
Cross-sectional Diagnostic interview Stratified random sample in governmental, private and UNRWA schools Questionnaires were administered in an interview format Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: Family ambiance (child's experience of anxiety in the home environment) INDIVIDUAL: male sex, refugee status, and child employment Protective factors: None were reported |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: family economic pressures; harsh discipline INDIVIDUAL: age, child psychological maltreatment |
| Khamis, 2008 | Gaza Strip and the West Bank from cities (41.3%), villages (17.3% and refugee camps (41.3%). | 179 adolescent boys Ages 12- 18 |
Cross-sectional Diagnostic interview and self-reported Questionnaires were administered in an interview format with adolescents at home Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Fatalism and negative coping Protective factors: None were reported |
GLOBAL: N/A MACRO: geographical location MEZZO: N/A MICRO: family economic pressures, parents' education, family income; parental support INDIVIDUAL: age, time since trauma, participating in Intifada, positive coping |
| Khamis, 2012 | Gaza Strip and south Lebanon | 600 adolescents Age 12-16 |
Cross-sectional Diagnostic interview Interview format conducted in the public school system in highly war exposed areas Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: family member injured, home demolished, family economic pressure INDIVIDUAL: depression and anxiety symptoms Protective factors: None were reported |
GLOBAL: MACRO: N/A MEZZO: N/A MICRO: family member killed INDIVIDUAL: religiosity, ideology |
| Punamaki et al., 2001 | Gaza | 86 adolescents 44 girls and 42 boys Ages 14 |
Longitudinal Diagnostic interview and self-reported Design excluded baseline measures of study outcome Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: higher exposure to traumatic events MEZZO: N/A MICRO: higher maternal love and caring INDIVIDUAL: N/A Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: higher paternal love and caring INDIVIDUAL: child reporting they would actively respond to violent threat (e.g., confront soldiers) |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: maternal and paternal rejection and hostility INDIVIDUAL: intelligence, creativity, age, sex, stressful life events |
| Qouta et al., 2007 | Gaza | 65 adolescents 52% girls Ages 17 |
Longitudinal prospective study Diagnostic interview Military trauma exposed adolescents from a community-based random sample of 1,082, which was representative of schools in refugee camps, and urban and resettled areas Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: High exposure to military trauma MICRO: N/A INDIVIDUAL: Cognitive capacity and neuroticism Protective factors: None were reported |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: mother's discipline style INDIVIDUAL: sex, intelligence; active coping |
| Thabet et al., 2009 | Gaza Strip | Participants were 412 children from the Gaza Strip Ages 12- 16 |
Cross-sectional Diagnostic interview and self-reported Random sample Gaza traumatic events checklist (GTEC), the SCID (DSM-V) and the Perceived Parenting Support Scale (PPSS) Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: The number of exposures to traumatic events MEZZO: receiving social assistance MICRO: Fathers lower education INDIVIDUAL: N/A Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: Perceived parenting support INDIVIDUAL: N/A |
GLOBAL: N/A MACRO: N/A MEZZO: geographic region MICRO: number of rooms in house; number of siblings; family income, mother's education, parental education INDIVIDUAL: age, sex |
Table 2. Four primary research studies focused on Israeli adolescents.
| Study | Setting | Sample characteristics | Methods | Significant results | Non-significant results |
|---|---|---|---|---|---|
| Chemtob et al., 2011 | Israel | Participants were 2,094 students 52.2% of the participants were girls Ages 12-18 |
Cross-sectional Self-reported Convenience sample drawn from 10 Israeli secondary schools Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: Exposure (being present and injured, or not injured, or supposed to be near where an attack occurred, or being at the site before it took place) MEZZO: N/A MICRO: loved one injured in an attack INDIVIDUAL: boys, functional impairment Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Older age |
None were reported |
| Laufer et al., 2009 | 4 areas of Israel | 2,999 Israeli adolescents 42.2% boys and 57.8% girls Grades 7 to 9 (35.5% were 13 years old, 36.5% were 14 years old, 26.9% were 15 years old and 1% was 16 years old) |
Cross-sectional Self-reported Cluster sampling of Israeli adolescents Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Greater exposure MEZZO: N/A MICRO: N/A INDIVIDUAL: Social extrinsic religiosity, ideological intolerance, and fear Protective factors: None were reported |
None were reported |
| Levine et al., 2008 | Israel | 4,054 Israeli adolescents 1st sample (n=2,999) and 2nd sample (n=1,745) 1st sample- grades 7 to 9 2nd sample- Ages 16 |
Cross-sectional Self-reported Data were pooled from two adolescent samples that responded to the same questionnaires Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Self-reported posttraumatic growth related to greater PTSD; curvilinear relationship suggested the relationship was strongest at mid-point of PTSD severity Protective factors: None were reported |
None were reported |
| Pat-Horenczyk et al., 2007 | Jerusalem | 695 Israeli high school students 315 boys and 380 girls Grades 7 to 12 Ages 12-18 |
Cross-sectional Diagnostic interview Questionnaire study conducted in school setting Outcome: PTSD diagnosis |
Risk Factors: GLOBAL: N/A MACRO: Greater exposure (personal, near-miss) MEZZO: N/A MICRO: N/A INDIVIDUAL: female sex Protective factors: None were reported |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: No significant interactions were found between exposure level and PTSD symptoms No significant interaction found between gender and exposure for the diagnosis of probable PTSD |
Table 3. Seven primary research studies focused on both Palestinian and Israeli adolescents.
| Study | Setting | Sample characteristics | Methods | Significant results | Non-significant results |
|---|---|---|---|---|---|
| Al-Krenawi, Graham, & Kanat-Maymon, 2009 | Ariel, Haifa, Tel Aviv, Gaza cities, villages and refugee camps. Cluster sample of youths | 422 Jewish Israeli adolescents in Ariel, Haifa and Tel Aviv. 450 Palestinian adolescents in Gaza cities, villages and refugee camps Ages 14 -18 |
Cross-sectional Diagnostic interview and self-reported Cluster sampling Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Exposure to political violence MEZZO: role of community is important for a sense of belonging. MICRO: family functioning; peer relationships INDIVIDUAL: general distress, aggression Protective factors: None were reported |
None were reported |
| Dubow et al., 2012 | Israel and Palestine | 600 Palestinian and 901 Israeli (Jewish and Arab) children Ages 8, 11 and 14 |
Longitudinal Diagnostic interview and self-reported Study conducted at three waves, one year apart, using interview method in family home Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Palestinian: ethnic-political violence exposure MEZZO: Palestinian: school violence MICRO: Israeli Arabs: family violence INDIVIDUAL: Palestinian: female sex, previous PTSD, ethnic-political violence exposure Israeli Jews: previous PTSD Israeli Arabs: previous PTSD Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: Israeli Jews: older age |
GLOBAL: N/A MACRO: N/A MEZZO: Palestinian: intra-ethnic community violence Israeli Jews: school and intra-ethnic community violence MICRO: Palestinian: parents education, family violence Israeli Jews: parents education, family, ethnic-political Israeli Arabs: parents education; ethnic violence INDIVIDUAL: Palestinian: age Palestinian: Israeli Jews: sex Israeli Arabs: sex |
| Dubow et al., 2012 | West Bank and Gaza | 901 Israeli and 600 Palestinian youths Approximately 50% boys and 50% girls Ages 8, 11 and 14 |
Longitudinal Diagnostic interview and self-reported Study 3 waves of data collection one year apart, using interview method in family home |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: female sex non-Israeli Arab, exposure to political violence Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: Positive parenting when exposure levels were high INDIVIDUAL: Self-esteem was protective when exposure was high |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: parent education level, parent depression, positive parenting INDIVIDUAL: age, Palestinian versus non-Palestinian; child academic grade, child grade did not moderate exposure |
| Hamama-Raz et al., 2008 | Israel and Palestine | 276 Israeli Palestinian and 1,469 Jewish adolescents 177 were Israeli Palestinian girls and 9 were Israeli Palestinian boys. 909 were Jewish girls and 56 were Jewish boys Ages 16 |
Cross-sectional Self-reported Classroom based questionnaire administration Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: negative life events (Jews only), objective exposure, subjective exposure (Jews only), inability to forgive, being Palestinian Protective factors: None were reported |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: negative life events (Palestinian), subjective exposure (Palestinian), attitudes toward peace, ability to forgive, revenge |
| Lavi et al., 2005 | Ramallah and Israel | 245 Palestinian and 300 Israeli-Palestinian adolescents 46% of the Israeli Palestinian group and 44% of the Palestinian group were boys 6th to 9th grades. Mean age in Palestinian group was 13.517 and 14.752 in the Israeli Palestinian group |
Cross-sectional Diagnostic interview and self-reported Self-reported questionnaire conducted in summer of 2001 Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: Number of exposures MEZZO: N/A MICRO: N/A INDIVIDUAL: subjective threat perception, global distress, anxiety, depression, anger, dissociation Protective factors: GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: future orientation and attitudes towards peace (Palestinians) |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: future orientation and attitudes towards peace (Jews) |
| Pat-Horenczyk et al., 2009 | Palestinian sample: West Bank. Israeli sample: living in the Jerusalem area | 1,016 Israeli and 1,235 Palestinian adolescents Palestinian sample: 54.7% were girl and 45.3% were boys Israeli sample: 51.6% were girls and 48.4% were boys Palestinian sample: Grades 9-11 aged from 14 to 17 years old Israeli sample: grades 7-12 aged from 12 to 18 years old |
Cross-sectional Diagnostic interview and self-reported Convenience sample using self-report questionnaires conducted in a school setting Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: N/A MEZZO: role of community is important for a sense of belonging MICRO: N/A INDIVIDUAL: Palestinians: coping (adaptive or maladaptive), severe exposures, female sex. Jews: coping (maladaptive) Protective factors: None were reported |
GLOBAL: N/A MACRO: N/AMEZZO: N/A MICRO: N/A INDIVIDUAL: Jews: coping (adaptive), moderate or severe exposures, female sex |
| Schiff et al., 2012 | North of Israel | 1800 Jewish and 2351 Arab 54.4% were Jewish boys and 41.5% were Arab boys 7th to 11th grade students Ages 13 - 17 |
Cross-sectional Self-reported Representative sample using self-report questionnaires conducted in a school setting Outcome: PTSD symptom severity |
Risk Factors: GLOBAL: N/A MACRO: other traumatic exposures, war exposures MEZZO: N/A MICRO: N/A INDIVIDUAL: female sex, being Palestinian, childhood physical abuse Protective factors: None were reported |
GLOBAL: N/A MACRO: N/A MEZZO: N/A MICRO: N/A INDIVIDUAL: grade in school, war exposure was not moderated by other types of trauma exposure, ethnicity did not moderate trauma exposure |
Results
A total of 20 studies (15 cross-sectional and five longitudinal studies) met the inclusion criteria. A total of nine articles analyzed the psychosocial risk factors of PTSD among Palestinian adolescents (see Table 1), four articles assessed the psychosocial risk factors of PTSD among Israeli adolescents (see Table 2), and seven articles assessed the psychosocial risk and protective factors of PTSD in both Palestinian and Israeli adolescents in the same study (see Table 3). All tables are included in the supplemental materials.
The results of the review are presented below, organized by the ecological levels described above, and are presented according to the target populations under study. Unless otherwise specified, results are to be interpreted such that if a certain risk or protective factor is associated with PTSD, it was associated in all studies that included this factor (i.e., no null findings were present), unless specified in the text.
Palestinian population
A total of nine articles analyzed the psychosocial risk factors of PTSD among Palestinian adolescents (see Table 1).
Macro-level
Five studies demonstrated that exposure to political violence was significantly associated with PTSD symptom severity (Al-Krenawi & Graham, 2012; Dubow et al., 2009; Punamäki, Qouta, & El-Sarraj, 2001; Qouta, Punamäki, Montgomery, & El Sarraj, 2007) or PTSD diagnosis (Thabet et al., 2009). Low socioeconomic status also conferred greater risk for PTSD severity (Al-Krenawi & Graham, 2012) and diagnosis (Khamis, 2012) where economic hardship relates to an increase in stress in the family and also greater difficulty in accessing healthcare for treatment due to the limited availability of resources. Other papers studying this population found no significant associations between socioeconomic stressors and PTSD (Khamis, 2005, 2008).
Mezzo-level
One study assessed the higher severity of PTSD among adolescents living in refugee camps compared to those living in urban areas (e.g., towns and villages) (Dubow et al., 2009). Adolescents dwelling in rural versus urban areas had increased PTSD symptom severity (Dubow et al., 2009). If an individual is living in Gaza, or had greater school violence (Dubow et al., 2009), or was receiving social assistance (Thabet et al., 2009), they had greater PTSD symptom severity or likelihood of PTSD diagnosis.
Micro-level
One of the studies revealed that lower parental education was associated with an increased risk for PTSD diagnosis (Thabet et al., 2009). Other studies found non-significant findings between the association of parental education and PTSD (Al-Krenawi & Graham, 2012; Dubow, Boxer, et al., 2012; Khamis, 2008).Three studies examined the importance of school, peer and family relations as protective factors against PTSD symptom severity (Elbedour et al., 2007; Punamäki et al., 2001; Thabet et al., 2009). Three studies showed that school and family violence was associated with greater PTSD symptoms (Al-Krenawi, Graham, & Sehwail, 2007; Dubow et al., 2009; Dubow, Boxer, et al., 2012). One study noted that higher maternal love and caring was associated with PTSD symptom severity (Punamäki et al., 2001) . One study showed that an injury to a family member, having one's home demolished, and economic pressures were associated with PTSD diagnosis (Khamis, 2012).
Individual-level
One study found that religiosity was a protective factor against PTSD symptom severity (Al-Krenawi & Graham, 2012). Three studies focused on sex differences for the severity or development of PTSD where girls demonstrated higher PTSD in two studies (Al-Krenawi & Graham, 2012; Dubow, Boxer, et al., 2012) and boys in another (Khamis, 2005). Three studies found non-significant findings between sex and PTSD symptom severity (Punamäki et al., 2001; Qouta et al., 2007; Thabet et al., 2009). One study examined the association of age and PTSD and concluded that those who are older were more likely to experience PTSD symptoms (Dubow et al., 2009). Three studies found non-significant findings between age and PTSD symptoms (Khamis, 2005, 2008; Punamäki et al., 2001; Thabet et al., 2009). Finally, one study revealed that children who worked had higher rates of PTSD (50%) than those who did not work (32%), since working outside of the home increases the risk of witnessing violence (Khamis, 2005).
Israeli Population
A total of four articles assessed the psychosocial risk factors of PTSD among Israeli adolescents (see Table 2).
Macro-level
Three studies demonstrated that exposure to political violence was associated with the increased risk of PTSD (Chemtob et al., 2011; Laufer & Solomon, 2008; Pat-Horenczyk et al., 2007).
Mezzo-level & Micro-level
No studies were identified that measured mezzo- or micro- level ecological factors in the Israeli adolescent population based on the inclusion/exclusion criteria for this current review.
Individual-level
One study found an association between religiosity and an increase in PTSD symptom severity (Laufer & Solomon, 2008). Contrary to what was found in the Palestinian population, one study demonstrated that age was associated with an increased risk for suicide ideation but protective against partial or full PTSD among the Israeli population (Chemtob et al., 2011). Two studies demonstrated that girls are more likely to receive a PTSD diagnosis than boys (Chemtob et al., 2011; Pat-Horenczyk et al., 2007).
Israeli and Palestinian adolescents in the same study
Seven articles assessed the psychosocial risk and protective factors for PTSD in both Palestinian and Israeli adolescents in the same study (see Table 3).
Macro-level
Each of the seven studies found a positive relationship between political violence exposure to and increased risk of PTSD in both populations (Al-Krenawi et al., 2009; Dubow, Boxer, et al., 2012; Dubow, Huesmann, et al., 2012; Hamama-Raz, Solomon, Cohen, & Laufer, 2008; Lavi & Solomon, 2005; Pat-Horenczyk et al., 2009; Schiff et al., 2012).
Mezzo-level
Two of the studies demonstrated the importance of a sense of belonging to the community as an important protective factor (Al-Krenawi et al., 2009; Pat-Horenczyk et al., 2009). One study showed that among Palestinians, greater school violence was related to PTSD symptom severity (Dubow, Boxer, et al., 2012).
Micro-level
Three studies found evidence for the importance of perceived social support from family and peers in school as a protective factor for PTSD among both Palestinian and Israeli adolescents (Al-Krenawi et al., 2009; Dubow, Boxer, et al., 2012; Pat-Horenczyk et al., 2009). One study demonstrated that higher parental education is a protective factor for PTSD for both populations (Al-Krenawi et al., 2009).
Individual-level
One of the studies revealed that older Israeli adolescents are at greater risk for PTSD (Dubow, Boxer, et al., 2012). Four of the studies examined sex differences where girls are more likely to develop PTSD due to exposure to trauma and violence (Dubow, Boxer, et al., 2012; Dubow, Huesmann, et al., 2012; Pat-Horenczyk et al., 2009; Schiff et al., 2012) and all of the seven studies demonstrated that the Palestinian adolescent population as a whole is more prone to the development of PTSD compared to the Israeli adolescent population. Protective factors for PTSD included positive coping strategies measured through qualitative and quantitative data (Pat-Horenczyk et al., 2009).
Discussion
The objective of this systematic review was to examine the risk and protective factors associated with PTSD among Palestinian and Israeli adolescents. We further aimed to compare the two populations in order to identify differences across the socioecological levels. In this discussion, we review the differences found between these two groups and explore implications for intervention.
On a macro-level, the findings of the review indicated, almost universally, that increased exposure to political violence was associated with greater PTSD for both Palestinians and Jewish Israelis. The findings of the studies suggest that Arab-Israelis experience economic inequalities compared to Jewish-Israelis. This is supported by previous research that suggests a higher economic status is associated with fewer mental health and PTSD symptoms (Al-Krenawi & Graham, 2012). This finding further suggests that the development of PTSD is not inevitable, but is a reflection of the social, economic and cultural conditions which have the potential to influence these relationships and can be addressed by public health policy and intervention (Al-Krenawi & Graham, 2012).
On the mezzo-level, it was also noted in the studies, but not directly linked to PTSD, that Palestinians experience marginalization and discriminatory policies (Al-Krenawi & Graham, 2012; Ronen, Abuelaish, Rosenbaum, Agbaria, & Hamama, 2013). For example, Palestinians experience discrimination at checkpoints, and experience fear, stress and humiliation (Qouta et al., 2007). It is notable that these social challenges were not directly examined to understand their influence in the studies we reviewed. It would be worthwhile for future research to explicitly test associations between discrimination and social determinants of mental health within the context of ongoing trauma.
In addition to the risk conferred by political violence, several studies describe the role of micro-level factors, the role of community, school and family violence, and the consequence of increased PTSD. The symptoms of PTSD have the ability to take a toll on other aspects of functioning including cognitive, behavioral social and emotional functioning, including but not limited to academic and cognitive difficulties (Margolin & Gordis, 2004). An adolescent exposed to family and community violence might interpret the world as an unsafe place and that the adolescent is unworthy of protection, leading to negative self-perception and feelings of neglect, which both have negative impacts on academic as well as cognitive performance (Margolin & Gordis, 2004). Lower PTSD in Israeli youth may be due in part to high social support, which leads to more emotional stability in daily life (Pat-Horenczyk et al., 2007). Given the risk factors outlined above, Palestinian adolescents are especially vulnerable to the development of PTSD, but may also be at greater risk for drug use, community and school violence (Schiff et al., 2012). In addition, the youth community in Israel is cohesive and Israeli society as a whole makes a great effort to return to normal as soon as possible after a terrorist attack (Pat-Horenczyk et al., 2007).
On an individual-level, females were particularly vulnerable as nine studies showed that female sex was associated with PTSD. Individual-level risk factors include coping style and lack of help-seeking. Several studies (Al-Krenawi & Graham, 2012; Khamis, 2005, 2008) found that certain protective coping factors might guard adolescents from the impact of war and political violence and the greater the distress, the more frequent and intensive are the attempts to cope (Pat-Horenczyk et al., 2009). Research shows that coping style among the Palestinian and Israeli adolescent population differed in that Palestinians used religion as a coping method whereas Israelis utilized active coping which includes awareness of the stressor and attempts to reduce the negative outcome (Pat-Horenczyk et al., 2009).
Implications for interventions
It is essential for clinicians and researchers to have an understanding of multilevel and dynamic psychological processes in order to tailor a developmentally and culturally appropriate intervention for use among traumatized adolescents (Qouta, Punamäki, Miller, & El-Sarraj, 2008). It is important that resilience-focused interventions are tailored to specific contexts since they may not have similar effects on mental health across different political contexts (Betancourt & Khan, 2008). The results of this review suggest that interventions that focus on strategies of adaptation (which include coping skills, forming positive relationships, community cohesion, and mobilizing social support networks) despite the presence of adversity are important areas to target. Strengthening families and community support for both populations would be beneficial.
There are only a few evidence-based interventions that focus on PTSD in adolescent populations during ongoing violence (Cohen, Mannarino, & Murray, 2011). The limited number of evidence-based interventions is due in part to challenges of assessment of mental health problems with regard to developmental differences of PTSD symptoms and under-identification across childhood and adolescence (Kerig, Fedorowicz, Brown, & Warren, 2000). Many evidence-based interventions focus on addressing behavioral and cognitive problems related to PTSD and focus on emotional awareness and expression, increasing feelings of emotional security, improving parent-child interactions, psycho-education, exposure, and learning specific coping strategies (Cohen et al., 2011). These largely individual-level interventions can be improved by adding elements to strengthen community cohesion, as the results of this review suggests.
To reduce the risk of developing PTSD in adolescent populations in the Palestinian authority and Israel, it is essential for future research to evaluate preventive measures implemented following terror attacks. Reducing the risk of PTSD is important to address as mental disorders are associated with other negative outcomes. These include aggression and a disruption in normal social structures (Al-Krenawi et al., 2009; Al-Krenawi & Graham, 2012; Kaplan et al., 2002; Pat-Horenczyk et al., 2009), and may influence normal social and cognitive development (Al-Krenawi et al., 2007; Al-Krenawi & Graham, 2012; Kaplan et al., 2002).
At the community and family level, preventive interventions are very popular in practice, but have seen little rigorous evaluation (Tol, Song, & Jordans, 2013). Community level interventions should identify concerns related to community safety and emotional distress as well as identify protective resources, one of which includes the importance of social support (Horowitz, McKay, & Marshall, 2005). In addition, school-based interventions provide an effective setting that helps children and adolescents through cognitive behavioral therapy and mind-body techniques (Rolfsnes & Idsoe, 2011) following traumatic events.
Preventive measures can include strategies to improve access to healthcare, training programs for parents to increase their support towards their children, building resiliency, building social support networks, encouraging the engagement of adolescents in religious activities, building support communities and training adolescents in positive and effective coping skills (Kimhi, Eshel, Zysberg, & Hantman, 2010). Such programs are focused on psychosocial interventions that address fear and memory consolidation aimed at preventing the development of chronic PTSD (Kearns, Ressler, Zatzick, & Rothbaum, 2012). Future intervention strategies can also include the reconstruction of learn and play facilities to encourage both populations to interact together positively, in the same space, since the level of school and peers plays an essential role in the development of PTSD.
Political violence leads to the destruction of physical infrastructure, devastation of cultural fabric, as well as shifts in identity, and value systems. The erosion of social capital also arises (Hall, Tol, Jordans, Bass, & Jong, 2014). Improvements to social policy include developments in mandated emergency planning in schools as well as other community agencies in order to create a sense of organization and structure (Pine, Costello, & Masten, 2005). In addition, creating tools to effectively manage and contain fear and other symptoms associated with trauma and violence and developing relief operations can also have a beneficial impact on at-risk populations (Pedersen, 2002; Pine et al., 2005). Both populations demonstrated emotional and behavioral problems associated with PTSD due to conflict exposure. This suggests that individual and community treatment are likely to be useful for both the Palestinian and Israeli adolescent population, further highlighting the need for the development of future interventions addressing the mezzo and individual-levels of the ecological framework (Al-Krenawi et al., 2009)
Integrating both mezzo-level factors such as community and micro-level factors such as mobilizing social networks has the potential to contribute to future interventions to reduce the risk of PTSD in these populations. There are limited community-based interventions that are family focused and an attempt to integrate the foundation of family would strengthen support networks (Leventhal & Brooks-Gunn, 2000). Similarly, studies show that the community has direct and moderating associations with health, therefore evaluating the intertwined relationship between built and social environments is vital for future intervention (Matthews & Yang, 2010). For example, neighborhood effects have the potential to influence adolescent well-being and development (Leventhal & Brooks-gunn, 2001). This concept is suggested by Leventhal & Brooks-Gunn via three models. The first, institutional resources, includes the quality and availability of different resources in the community such as quality care and early intervention programs. Similarly, neighborhoods shape the school quality and climate, which has an influence on health outcomes. Second, the model of relationships relates to parental characteristics and support networks as well as the home environment, which includes safety, support, routine and structure as well as cleanliness and space allocation. Finally, the model of norms and collective efficacy relates to the extent of formal and informal community institutions' ability to monitor the behavior of residents in order to maintain public order and establish social connections (Leventhal & Brooks-gunn, 2001). In conclusion, the establishment and modification of developmentally oriented frameworks to study the neighborhoods in which adolescents reside and the effect on adolescent health have important implications for policies and programs that shape adolescent and family well-being (Leventhal & Brooks-gunn, 2001). The implementation of preventive strategies includes re-building the mezzo-level factor of schools, while implementing the larger macro-level factors of security and reintegration. It is also essential to tailor such intervention strategies that are culturally sensitive to both populations.
Strengths and limitations
This study has several strengths and limitations. This review examines a topic that does not have many published articles, therefore it may be limited in its scope of information and findings. Many of the studies were cross-sectional in design, which limits the ability to draw inferences about potential causal relationships. Self-report measures were also common, leaving the findings vulnerable to recall bias. Due to the fact that there are so many differences between the studies with regards to design, measures and context, it is difficult to draw a definitive answer with regard to which population experiences greater suffering. However, the studies collected for this review reveal that the risk of PTSD due to conflict exposure may be greater among the adolescent Palestinian population. This may be due to the civilian and economic inequity experienced by the Palestinian minority which adds to a sense of diminished resources (Somer, Maguen, Or-Chen, & Litz, 2009). Although PTSD is highly co-morbid with other mental conditions such as depression, none of the studies included in this review examined the association between PTSD and other disorders. This an important gap in our understanding of the mental health problems facing adolescents in Israel. The literature on adolescents in other post-conflict settings clearly shows that PTSD is comorbid with other disorders, so at a minimum, comorbidity should be explored in future studies (Khamis, 2008). It is also noteworthy that many studies focused on risk factors and did not measure possible protective mechanisms. Further work is needed to understand factors related to resilience (e.g., Hall et al., 2014).
A research recommendation identified by this review is related to the levels of the social ecological framework that are not well represented. The gap is displayed in the evidence tables where many studies did not discuss factors at certain levels (Qouta et al., 2008). Global (e.g., government policies) levels were absent from the analyses of the papers included in the current review. There is limited knowledge related to the association among the three levels of resilience, which includes individual, community, and national resilience. Furthermore, research on resilience focuses on a single level rather than examining the connections among the different levels. Examining the three levels together significantly predicts an individual's well-being and effective coping with traumatic events (Kimhi, 2014). Although community level factors are identified as important in the Palestinian studies, they are lacking in the Israeli adolescent population. The gap is important to address since community processes influence the development of mental health outcomes (Kimhi et al., 2010). As there is limited knowledge regarding the association among the individual, community and national levels of resilience, further research is needed to create large-scale interventions to prepare populations to deal with traumatic events (Kimhi, 2014). Generally, future research should also investigate the underlying mechanisms that lead to PTSD in greater depth so as to better understand risk and protective factors leading to disorders in situations of ongoing conflict (Thabet et al., 2009).
References
- Al-Krenawi A, Graham JR, Kanat-Maymon Y. Analysis of trauma exposure, symptomatology and functioning in Jewish Israeli and Palestinian adolescents. The British Journal of Psychiatry. 2009;195(5):427–432. doi: 10.1192/bjp.bp.108.050393. [DOI] [PubMed] [Google Scholar]
- Al-Krenawi A, Graham JR, Sehwail MA. Tomorrow's players under occupation: An analysis of the association of political violence with psychological functioning and domestic violence, among Palestinian youth. American Journal of Orthopsychiatry. 2007;77(3):427. doi: 10.1037/0002-9432.77.3.427. [DOI] [PubMed] [Google Scholar]
- Al-Krenawi A, Graham JR. The impact of political violence on psychosocial functioning of individuals and families: The case of Palestinian adolescents. Child and Adolescent Mental Health. 2012;17(1):14–22. doi: 10.1111/j.1475-3588.2011.00600.x. [DOI] [PubMed] [Google Scholar]
- Amercian Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Washington, DC: Author; 2013. [Google Scholar]
- Bar-Tal D. From intractable conflict through conflict resolution to reconciliation: Psychological analysis. Political Psychology. 2000;21(2):351–365. [Google Scholar]
- Betancourt TS, Khan KT. The mental health of children affected by armed conflict: protective processes and pathways to resilience. International Review of Psychiatry. 2008;20(3):317–328. doi: 10.1080/09540260802090363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blum RW, Astone NM, Decker MR, Mouli VC. A conceptual framework for early adolescence: a platform for research. International Journal of Adolescent Medicine and Health. 2014;26(3):321–31. doi: 10.1515/ijamh-2013-0327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buka SL, Stichick TL, Birdthistle I, Earls FJ. Youth exposure to violence: prevalence, risks, and consequences. American Journal of Orthopsychiatry. 2001;71(3):298. doi: 10.1037/0002-9432.71.3.298. [DOI] [PubMed] [Google Scholar]
- Canetti D, Hall BJ, Rapaport C, Wayne C. Exposure to political violence and political extremism. European Psychologist 2015 [Google Scholar]
- Chemtob CM, Pat-Horenczyk R, Madan A, Pitman SR, Wang Y, Doppelt O, Brom D. Israeli adolescents with ongoing exposure to terrorism: Suicidal ideation, posttraumatic stress disorder, and functional impairment. Journal of Traumatic Stress. 2011;24(6):756–759. doi: 10.1002/jts.20708. [DOI] [PubMed] [Google Scholar]
- Cohen JA, Mannarino AP, Murray LK. Trauma-focused CBT for youth who experience ongoing traumas. Child Abuse & Neglect. 2011;35(8):637–646. doi: 10.1016/j.chiabu.2011.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deykin EY, Keane TM, Kaloupek D, Fincke G, Rothendler J, Siegfried M, Creamer K. Posttraumatic stress disorder and the use of health services. Psychosomatic Medicine. 2001;63(5):835–841. doi: 10.1097/00006842-200109000-00018. [DOI] [PubMed] [Google Scholar]
- Dubow EF, Boxer P, Huesmann LR, Landau S, Dvir S, Shikaki K, Ginges J. Cumulative effects of exposure to violence on posttraumatic stress in Palestinian and Israeli youth. Journal of Clinical Child & Adolescent Psychology. 2012;41(6):837–844. doi: 10.1080/15374416.2012.675571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dubow EF, Boxer P, Huesmann LR, Shikaki K, Landau S, Gvirsman SD, Ginges J. Exposure to conflict and violence across contexts: Relations to adjustment among Palestinian children. Journal of Clinical Child & Adolescent Psychology. 2009;39(1):103–116. doi: 10.1080/15374410903401153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dubow EF, Huesmann LR, Boxer P, Landau S, Dvir S, Shikaki K, Ginges J. Exposure to political conflict and violence and posttraumatic stress in Middle East youth: Protective factors. Journal of Clinical Child & Adolescent Psychology. 2012;41(4):402–416. doi: 10.1080/15374416.2012.684274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elbedour S, Onwuegbuzie AJ, Ghannam J, Whitcome JA, Hein FA. Post-traumatic stress disorder, depression, and anxiety among Gaza Strip adolescents in the wake of the second Uprising (Intifada) Child Abuse & Neglect. 2007;31(7):719–729. doi: 10.1016/j.chiabu.2005.09.006. [DOI] [PubMed] [Google Scholar]
- Galea S, Ahern J, Resnick H, Kilpatrick D, Bucuvalas M, Gold J, Vlahov D. Psychological sequelae of the September 11 terrorist attacks in New York City. New England Journal of Medicine. 2002;346(13):982–987. doi: 10.1056/NEJMsa013404. [DOI] [PubMed] [Google Scholar]
- Giacaman R, Shannon HS, Saab H, Arya N, Boyce W. Individual and collective exposure to political violence: Palestinian adolescents coping with conflict. The European Journal of Public Health. 2007;17(4):361–368. doi: 10.1093/eurpub/ckl260. [DOI] [PubMed] [Google Scholar]
- Glass TA, McAtee MJ. Behavioral science at the crossroads in public health: extending horizons, envisioning the future. Social Science & Medicine. 2006;62(7):1650–1671. doi: 10.1016/j.socscimed.2005.08.044. [DOI] [PubMed] [Google Scholar]
- Hall BJ, Tol W, Jordans M, Bass J, Jong J. Understanding resilience in armed conflict: Social resources and mental health of children in Burundi. SocialScience and Medicine. 2014;114:121–128. doi: 10.1016/j.socscimed.2014.05.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamama-Raz Y, Solomon Z, Cohen A, Laufer A. PTSD symptoms, forgiveness, and revenge among Israeli Palestinian and Jewish adolescents. Journal of Traumatic Stress. 2008;21(6):521–529. doi: 10.1002/jts.20376. [DOI] [PubMed] [Google Scholar]
- Herrenkohl TI, Maguin E, Hill KG, Hawkins JD, Abbott RD, Catalano RF. Developmental risk factors for youth violence. Journal of Adolescent Health. 2000;26(3):176–186. doi: 10.1016/s1054-139x(99)00065-8. [DOI] [PubMed] [Google Scholar]
- Hidalgo RB, Davidson JRT. Posttraumatic stress disorder: epidemiology and health-related considerations. Journal of Clinical Psychiatry. 2000 [PubMed] [Google Scholar]
- Hobfoll SE, Canetti D, Hall BJ, Brom D, Palmieri PA, Johnson RJ, Galea S. Are community studies of psychological trauma's impact accurate? A study among Jews and Palestinians. Psychological Assessment. 2011;23(3):599. doi: 10.1037/a0022817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horowitz K, McKay M, Marshall R. Community violence and urban families: experiences, effects, and directions for intervention. American Journal of Orthopsychiatry. 2005 doi: 10.1037/0002-9432.75.3.356. [DOI] [PubMed] [Google Scholar]
- Kalia M. Assessing the economic impact of stress—The modern day hidden epidemic. Metabolism. 2002;51(6):49–53. doi: 10.1053/meta.2002.33193. [DOI] [PubMed] [Google Scholar]
- Kaplan Z, Weiser M, Reichenberg A, Rabinowitz J, Caspi A, Bodner E, Zohar J. Motivation to serve in the military influences vulnerability to future posttraumatic stress disorder. Psychiatry Research. 2002;109(1):45–49. doi: 10.1016/s0165-1781(01)00365-1. [DOI] [PubMed] [Google Scholar]
- Kearns MC, Ressler KJ, Zatzick D, Rothbaum BO. Early interventions for PTSD: a review. Depression and Anxiety. 2012;29(10):833–842. doi: 10.1002/da.21997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerig PK, Fedorowicz AE, Brown CA, Warren M. Assessment and intervention for PTSD in children exposed to violence. Journal of Aggression, Maltreatment & Trauma. 2000;3(1):161–184. [Google Scholar]
- Khamis V. Post-traumatic stress disorder among school age Palestinian children. Child Abuse & Neglect. 2005;29(1):81–95. doi: 10.1016/j.chiabu.2004.06.013. [DOI] [PubMed] [Google Scholar]
- Khamis V. Post-traumatic stress and psychiatric disorders in Palestinian adolescents following intifada-related injuries. Social Science & Medicine. 2008;67:1199–1207. [Google Scholar]
- Khamis V. Impact of war, religiosity and ideology on PTSD and psychiatric disorders in adolescents from Gaza Strip and South Lebanon. Social Science & Medicine. 2012;74(12):2005–2011. doi: 10.1016/j.socscimed.2012.02.025. [DOI] [PubMed] [Google Scholar]
- Kimhi S. Levels of resilience: Associations among individual, community, and national resilience. Journal of Health Psychology. 2014:1–7. doi: 10.1177/1359105314524009. [DOI] [PubMed] [Google Scholar]
- Kimhi S, Eshel Y, Zysberg L, Hantman S. Postwar winners and losers in the long run: determinants of war related stress symptoms and posttraumatic growth. Community Mental Health Journal. 2010;46(1):10–19. doi: 10.1007/s10597-009-9183-x. [DOI] [PubMed] [Google Scholar]
- Laufer A, Solomon Z. Gender differences in PTSD in Israeli youth exposed to terror attacks. Journal of Interpersonal Violence. 2008;24(6):959–976. doi: 10.1177/0886260508319367. [DOI] [PubMed] [Google Scholar]
- Lavi T, Solomon Z. Palestinian youth of the Intifada: PTSD and future orientation. Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44(11):1176–1183. doi: 10.1097/01.chi.0000177325.47629.4c. [DOI] [PubMed] [Google Scholar]
- Leventhal T, Brooks-Gunn J. The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychological Bulletin. 2000;126(2):309–337. doi: 10.1037/0033-2909.126.2.309. [DOI] [PubMed] [Google Scholar]
- Leventhal T, Brooks-gunn J. Changing neighborhoods and child well-being: Understanding how children may be affected in the coming century. Advances in Life Course Research. 2001;6:263–301. [Google Scholar]
- Li C, Liu Y, Yin S, Lu C, Liu D, Jiang H, Pan F. Long-term effects of early adolescent stress: dysregulation of hypothalamic-pituitary-adrenal axis and central corticotropin releasing factor receptor 1 expression in adult male rats. Behavioural Brain Research. 2015;288:39–49. doi: 10.1016/j.bbr.2015.04.007. [DOI] [PubMed] [Google Scholar]
- Margolin G, Gordis EB. Children's exposure to violence in the family and community. Current Directions in Psychological Science. 2004;13(4):152–155. [Google Scholar]
- Matthews Sa, Yang TC. Exploring the role of the built and social neighborhood environment in moderating stress and health. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine. 2010;39(2):170–83. doi: 10.1007/s12160-010-9175-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris A, Gabert-Quillen C, Delahanty D. The association between parent PTSD/depression symptoms and child PTSD symptoms: A meta-analysis. Journal of Pediatric Psychology. 2012;37(10):1076–1088. doi: 10.1093/jpepsy/jss091. [DOI] [PubMed] [Google Scholar]
- Nuttman-Shwartz O, Shoval-Zuckerman Y. Continuous Traumatic Situations in the Face of Ongoing Political Violence: The Relationship Between CTS and PTSD. Trauma, Violence & Abuse. 2015 doi: 10.1177/1524838015585316. [DOI] [PubMed] [Google Scholar]
- Osofsky JD. The impact of violence on children. The Future of Children. 1999;3(9):33–49. [PubMed] [Google Scholar]
- Pat-Horenczyk R, Abramovitz R, Peled O, Brom D, Daie A, Chemtob CM. Adolescent exposure to recurrent terrorism in Israel: posttraumatic distress and functional impairment. American Journal of Orthopsychiatry. 2007;77(1):76. doi: 10.1037/0002-9432.77.1.76. [DOI] [PubMed] [Google Scholar]
- Pat-Horenczyk R, Qasrawi R, Lesack R, Haj-Yahia M, Peled O, Shaheen M, Abdeen Z. Posttraumatic symptoms, functional impairment, and coping among adolescents on both Sides of the Israeli–Palestinian conflict: A cross-cultural approach. Applied Psychology. 2009;58(4):688–708. [Google Scholar]
- Pedersen D. Political violence, ethnic conflict, and contemporary wars: Broad implications for health and well-being. Social Science and Medicine. 2002;55:175–190. doi: 10.1016/s0277-9536(01)00261-1. [DOI] [PubMed] [Google Scholar]
- Pine DS, Costello J, Masten A. Trauma, proximity, and developmental psychopathology: the effects of war and terrorism on children. Neuropsychopharmacology. 2005;30(10):1781–1792. doi: 10.1038/sj.npp.1300814. [DOI] [PubMed] [Google Scholar]
- Punamäki RL, Qouta S, El-Sarraj E. Resiliency factors predicting psychological adjustment after political violence among Palestinian children. International Journal of Behavioral Development. 2001;25(3):256–267. [Google Scholar]
- Qouta S, Punamäki R, Miller T, El-Sarraj E. Does war beget child aggression? Military violence, gender, age and aggressive behavior in two Palestinian samples. Aggressive Behavior. 2008;34(3):231–244. doi: 10.1002/ab.20236. [DOI] [PubMed] [Google Scholar]
- Qouta S, Punamäki RL, Montgomery E, El Sarraj E. Predictors of psychological distress and positive resources among Palestinian adolescents: Trauma, child, and mothering characteristics. Child Abuse & Neglect. 2007;31:699–717. doi: 10.1016/j.chiabu.2005.07.007. [DOI] [PubMed] [Google Scholar]
- Rolfsnes ES, Idsoe T. School-based intervention programs for PTSD symptoms: A review and meta-analysis. Journal of Traumatic Stress. 2011;24:155–165. doi: 10.1002/jts.20622. [DOI] [PubMed] [Google Scholar]
- Ronen T, Abuelaish I, Rosenbaum M, Agbaria Q, Hamama L. Predictors of aggression among Palestinians in Israel and Gaza: Happiness, need to belong, and self-control. Children and Youth Services Review. 2013;35(1):47–55. [Google Scholar]
- Schiff M, Pat-Horenczyk R, Benbenishty R, Brom D, Baum N, Astor RA. High school students' posttraumatic symptoms, substance abuse and involvement in violence in the aftermath of war. Social Science & Medicine. 2012;75(7):1321–1328. doi: 10.1016/j.socscimed.2012.05.010. [DOI] [PubMed] [Google Scholar]
- Somer E, Maguen S, Or-Chen K, Litz BT. Managing terror: differences between Jews and Arabs in Israel. International Journal of Psychology: Journal International de Psychologie. 2009;44(2):138–46. doi: 10.1080/00207590701609076. [DOI] [PubMed] [Google Scholar]
- Spilerman S, Stecklov G. The dislocations of terror: Assessments of risk during the Second Intifada. Social Science Research. 2013;42(3):926–41. doi: 10.1016/j.ssresearch.2012.12.013. [DOI] [PubMed] [Google Scholar]
- Taylor S. Posttraumatic Stress Disorder. In: McKay D, Abramowitz JS, Taylor S, editors. Cognitive–behavioral therapy for refractory cases: Turning failure into success. Washington, DC: American Psychological Association; 2010. pp. 139–153. [Google Scholar]
- Thabet AA, Ibraheem AN, Shivram R, Winter EA, Vostanis P. Parenting support and PTSD in children of a war zone. International Journal of Social Psychiatry. 2009;55(3):226–237. doi: 10.1177/0020764008096100. [DOI] [PubMed] [Google Scholar]
- Tol WA, Song S, Jordans MJD. Annual Research Review: Resilience and mental health in children and adolescents living in areas of armed conflict–a systematic review of findings in low-and middle-income countries. Journal of Child Psychology and Psychiatry. 2013;54(4):445–460. doi: 10.1111/jcpp.12053. [DOI] [PubMed] [Google Scholar]
- Van Rooyen K, Nqweni ZC. Culture and posttraumatic stress disorder (PTSD): A proposed conceptual framework. South African Journal of Psychology. 2012;42(1):51–60. [Google Scholar]
- Veling W, Hall BJ, Joosse P. The association between posttraumatic stress symptoms and functional impairment during ongoing conflict in the Democratic Republic of Congo. Journal of Anxiety Disorders. 2013;27(2):225–230. doi: 10.1016/j.janxdis.2013.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Adolescent Health. 2013 Retrieved from http://www.who.int/topics/adolescent_health/en/
- World Health Organization. Violence Prevention Alliance. 2015 Retrieved from http://www.who.int/violenceprevention/en/
- Zlotnick C, Warshaw M, Shea MT, Allsworth J, Pearlstein T, Keller MB. Chronicity in posttraumatic stress disorder (PTSD) and predictors of course of PTSD in patients with anxiety disorders. Journal of Traumatic Stress. 1999;12(1):89–100. doi: 10.1023/A:1024746316245. [DOI] [PubMed] [Google Scholar]
- Zwi A, Ugalde A. Political violence in the third world: a public health issue. Health Policy and Planning. 1991;6(3):203–217. [Google Scholar]