

Abstract
BACKGROUND
Subjective cognitive and functional limitations are early markers of future dementia and physical disability. Hypertension may increase the risk of dementia; however, the magnitude and significance of subjective limitations in the hypertensive US population are unknown, particularly in African Americans who bear the greatest burden of hypertension. Our objectives were to assess the prevalence and racial disparity of subjective cognitive and functional limitations and their impact on mortality in the hypertensive US population.
METHODS
We analyzed data from the National Health and Nutrition Examination Survey (NHANES) collected between 1999 and 2010 (N = 28,477; 31% with hypertension; 11% African American), which included blood pressure measurement, self-reported cognitive and functional (physical and non-physical) limitations, and all-cause mortality. Complex survey regression models were used.
RESULTS
In the United States, 8% of the hypertensive population reported cognitive and 25% reported functional limitations (vs. 5.7% and 15% respectively in the non-hypertensive population, P < 0.0001). Hypertensive African Americans carried the highest burden of cognitive (11%, P = 0.01) and functional (27%, P = 0.03) limitations compared to non-hypertensive African Americans and to non-African Americans. All-cause mortality was significantly higher in hypertensive individuals who reported cognitive or functional limitations (P < 0.0001 for both) relative to those without either.
CONCLUSIONS
The prevalence of cognitive and functional disability is larger in the US hypertensive population compared to the non-hypertensive population. African Americans with hypertension carry a disproportionate burden of these limitations. Individuals with hypertension who report cognitive or functional symptoms have higher all-cause mortality and query about these symptoms should be part of hypertension evaluation.
Keywords: African American, blood pressure, cognition, disparity, hypertension.
Hypertension may increase the risk of dementia and physical disability.1–3 Many individuals report subjective memory and functional complaints many years prior to the development of dementia and Alzheimer’s disease or further disability.4,5 In the United States, 18.7% of noninstitutionalized individuals report limitations in mental or functional abilities.6 The association between hypertension and these subjective cognitive complaints has not been evaluated.
African Americans disproportionately carry the greatest burden of hypertension in the United States, with a prevalence approaching 47%.7 African Americans have earlier onset of hypertension and greater hypertension-associated morbidity and mortality than any other racial group.8 We hypothesized that the magnitude of cognitive and functional limitations related to hypertension would also be higher in African Americans.
Although hypertension is known to increase all-cause mortality, it is not known if the presence of functional or cognitive limitations further affects mortality. Little attention has been focused on the role of cognitive function or physical symptoms in risk prediction. Since self-reported cognitive and functional disabilities are linked to poor outcomes in healthy adults,9 we propose that they also impact overall mortality in hypertension.
Therefore, our objectives were to estimate the prevalence and trends, measure racial disparity, and investigate the mortality risk of self-reported cognitive and functional limitations in the US hypertensive population over the last decade.
METHODS
Study design
The NHANES is conducted by the National Center for Health Statistics. The complex sampling design included selecting the primary sampling units, households, and individuals within the households. In 1999, NHANES became a continuous survey with a sample close to 5,000 persons each year. NHANES oversampled non-Hispanic Blacks (or African American). NHANES was approved by the National Center for Health Statistics Research Ethical Review Board and this analysis was conducted using de-identified publicly available data.10
Data elements
Each individual was evaluated by a computer-assisted personal interview system (demographic, socioeconomic, dietary and health-related questions) and an examination by trained personnel (medical, dental, physiological measurements, and laboratory tests). For this analysis we included data collected between 1999 and 2010. To examine trends in prevalence we combined the surveys into 3 periods of 4-year blocks each to improve our estimation abilities (1999–2002, 2003–2006, and 2007–2010).
Health data were collected during the interviews. Weight was measured using a digital scale, and height was measured using an electronic stadiometer while standing. Laboratory tests included serum creatinine, fasting lipid, glycosylated hemoglobin, c-reactive protein, and urinary albumin.
Hypertension
Blood pressure was measured by a mercury sphygmomanometer by a trained physician in the right arm, unless there was a contra-indication for using that arm. Participants were asked to sit still for 5 minutes. No clothing was allowed between the skin and the blood pressure cuff. The correct size cuff was used (encircling at least 40% of the upper arm circumference and 80% of its length). Three seated systolic and diastolic blood pressure readings were obtained. Hypertension was defined as having a mean systolic blood pressure of 140 or greater, a DBP of 90mm Hg or greater, or self-reported use of an antihypertensive medication.
Subjective cognitive limitations
Limitations due to cognitive deficits were assessed by asking the question, “Are you limited in any way because of difficulty remembering or because you experience periods of confusion?” The participant was instructed to answer “yes” or “no.” Those who answered “yes” were considered to have subjective cognitive limitations. To assess the association of subjective cognitive limitations (based on this question) with objective cognitive performance, we used the 1999–2002 survey data, when the digit symbol substitution test was also available on 2,971 participants. Those who reported cognitive disability had significantly (P < 0.0001) lower scores on the digit symbol substitution test (mean: 34 SE: 1.6) compared to those who answered “no” (mean: 48 (0.6)). The weighted correlation between cognitive disability and lower score on the digit symbol substitution test was 87% (P < 0.0001).
Subjective functional limitations
Functional abilities were assessed using standardized questions regarding multiple functional domains: (i) activities of daily living (ADL) [getting in and out of bed/eating/dressing], (ii) instrumental activities of daily living [managing money/doing chores around the house/preparing meals], (iii) general physical activity [lifting/standing/sitting/reaching up/grasping small objects], (iv) mobility [stooping, crouching, or kneeling/walking from one room to another/standing up from an armless straight chair/walking for a quarter of a mile/walking up 10 steps], and (v) social interaction and activities [participating in social activities such as meetings, parties, or visiting friends]. Responses for all functional domain questions included no difficulty, some difficulty, much difficulty, or unable to do. We defined a limitation in 1 domain if the participant reported “much difficulty” or “inability to perform” on at least 1 task within that domain. Functional limitation was defined as having a limitation in at least one of these domains. The correlation between cognitive and functional limitations was 36%.
Mortality linkage data
National Center for Health Statistics performed linkage between NHANES data (1999–2004) and death certificate data available from the National Death Index up to 31 December 2006. Linkage was conducted using a probabilistic approach on eligible participants (13,422 from 1999 to 2004) based on demographics, names, states of birth or residence, and social security numbers.11 Mortality analyses were conducted only on the survey data from 1999 to 2004.
Statistical analysis
We conducted a separate analysis of each limitation domain using analytical procedures (surveyreg or surveylogistic) that accounted for the complex sampling design of NHANES. All analyses were weighted to the 12 years of examination weights (or 6 years for the mortality analyses).11 SEs of parameter estimates were calculated using Taylor series linearization.11 We used the 2000 US population census to calculate age-adjusted prevalence in the United States and the current population surveys for the midpoint at each survey to estimate the population counts with hypertension and disability.12 We calculated the OR of having disability in the hypertensive vs. non-hypertensive population with adjustments for age, gender, race, stroke, education, congestive heart failure/heart disease (coronary artery disease), diabetes mellitus, and body mass index. We calculated the population attributable risk using the adjusted OR: (number of exposed cases/total number of cases) × [(adjusted OR − 1)/adjusted OR).13 We also assessed the association (OR) between race and prevalence of both limitations using surveylogistic with race being the independent variable and adjusted for the same covariates.
We assumed that missing data were not at random, and we accounted for that in all our models by including those with missing data as a separate category as recommended by the NHANES analytical guidelines.11 To assess the prevalence of limitations by race and hypertension, we included the product term (hypertension × race) in our models. A significant P-value for that term indicates a significant difference by race/hypertension status on the corresponding measure. Similarly to assess the impact of gender or age we included a product term in the models.
For the mortality analyses, we fit Cox Proportional Hazard Models adjusted for complex survey design (surveyphreg) to calculate the mortality rates in hypertensive and non-hypertensive participants with and without limitations. Subjects not linked to the death index were censored at the last day for mortality follow-up (December 2006). We conducted 2 survival analyses, first one related to cognitive and the second one related to functional limitations. Survival analyses were adjusted for age, gender, race, systolic blood pressure, education, diabetes mellitus, stroke, body mass index, congestive heart failure, heart disease, and cholesterol. In these analyses we compared the mortality in 4 groups: with and without hypertension/with and without limitations. To assess the impact of race we then included a product term Race × (hypertension/limitation groups) in our models in addition to the other covariates. Finally, we investigated the association between use of antihypertensive medications with each disability in those with hypertension and the prevalence of each disability using surveyreg and antihypertensive medication being the independent variable, and in 3 systolic blood pressure categories (<140, 140–149, and ≥ 150mm Hg). Because of the effect of antihypertensive medications on systolic blood pressure we conducted the latter analyses in those treated and untreated separately.
SAS (Version 9.3, Cary, NC) statistical software was used for all analyses.
RESULTS
Characteristics
A total of 28,477 individuals were included in these analyses (37.5% 20–39 years, 38.9% 40–59 years, 23.6% 60 years or older; 51.2% women, 70.8% non-Hispanic Whites, and 11.1% African American). The prevalence of hypertension was 31% in the combined survey (1999–2010). From 1999–2002 to 2007–2010, hypertension prevalence minimally changed (30.1% in the 1999–2002 and 32% in the 2003–2006 and 2007–2010 surveys, P = 0.22). Basic sample characteristics and their trends are shown in Supplementary Tables 1A and 2A.
Prevalence of subjective limitations in hypertension
Almost a quarter (24%) of the hypertensive US population reported functional and 8% reported cognitive limitations (vs. 15% and 5.7% respectively in the normotensive population, P < 0.0001 for both) as shown in Table 1. These rates translate to 21,202,454 with subjective functional and 6,537,332 with subjective cognitive limitations in the United States.
Table 1.
Age-adjusted prevalence and odds ratio of disability in the hypertensive compared to the non-hypertensive population in the United States (1999–2010)
| Age-adjusted prevalence, % | Unadjusted OR | Adjusted ORa | |||||||
|---|---|---|---|---|---|---|---|---|---|
| NTN | HTN | P | OR | 95% CI | P | OR | 95% CI | P | |
| Cognitive disability | 5.7 (0.2) | 8.1 (0.4) | <0.0001 | 2.59 | (2.29, 2.94) | <0.0001 | 1.42 | (1.19, 1.7) | <0.0001 |
| Functional disability | 15.1 (0.4) | 23.8 (0.7) | <0.0001 | 1.51 | (1.37, 1.67) | <0.0001 | 1.24 | (1.11, 1.38) | 0.0001 |
| Functional domain | |||||||||
| ADL | 3.2 (0.1) | 4.3 (0.3) | 0.0005 | 1.34 | (1.07, 1.68) | 0.01 | 1.0 | (0.77, 1.29) | 0.99 |
| IADL | 6.6 (0.3) | 10.3 (0.4) | <0.0001 | 1.4 | (1.23, 1.59) | <0.0001 | 1.18 | (1.04, 1.33) | 0.01 |
| General physical | 10.4 (0.3) | 17 (0.6) | <0.0001 | 1.65 | (1.48, 1.84) | <0.0001 | 1.25 | (1.12, 1.41) | 0.0001 |
| Mobility | 10.6 (0.3) | 18 (0.6) | <0.0001 | 1.87 | (1.68, 2.09) | <0.0001 | 1.28 | (1.13, 1.45) | 0.0001 |
| Social activity | 5 (0.2) | 7.7 (0.3) | <0.0001 | 1.41 | (1.20, 1.65) | <0.0001 | 1.14 | (0.93, 1.39) | 0.21 |
OR obtained from surveylogisitc with the Wald’s 95% CI form the variance estimated by Taylor linearization method. Italics are the P-values for the comparison between the hypertension and normotension groups.
Abbreviations: ADL, activities of daily living; CI, confidence interval; HTN: hypertension; IADL, Instrumental activities of daily living; NTN, non-hypertension; OR, odds ratio.
aAdjusted for age, gender, race, stroke, education, congestive heart failure/heart disease, diabetes mellitus, and body mass index.
Hypertension was associated with higher risk of subjective cognitive OR = 1.42; 95% confidence interval (CI) [1.19–1.70] and functional (OR = 1.24; 95% CI [1.11–1.38]) limitations, after adjusting for age, gender, race, stroke, education, congestive heart failure /heart disease, diabetes mellitus, and body mass index. This higher risk was significant in all the functional subdomains except for activities of daily living (P = 0.99) and social activity (P = 0.21). The unadjusted and covariate-adjusted ORs of both cognitive and functional disability as well as the functional subdomains are shown in Table 1. After adjusting for covariates, African Americans were more likely to report cognitive limitations: OR = 1.21, 95% CI [1.05–1.40] but not functional limitations: (OR = 1.12, 95% CI [0.99–1.27].
Secular trends in hypertension
Although there was a slight decline in the prevalence of subjective functional limitation from 1999–2002 to 2003–2006, overall, from 1999–2002 to 2007–2010 there was an increase in subjective functional limitations in the hypertensive population to a greater extent than in the normotensive population (P-value for the difference in trends = 0.003) as shown in Figure 1. A similar difference in trend was observed in subjective cognitive limitations, but it was not statistically significant (P = 0.31). In both cases, there was a slight decrease from 2003–2006 to 2007–2010 in the prevalence of both subjective limitations. During each survey period, the prevalence of disability was higher in hypertensive relative to non-hypertensive individuals (all P < 0.001).
Figure 1.

Trends in age-adjusted prevalence of cognitive and functional disability (including the 5 subdomains) over the survey periods from 1999–2002 to 2007–2010. Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living. All P-values for non-hypertension vs. hypertension <0.001. P-values for the difference in trends over 3 study period by hypertension status: cognitive disability = 0.31, functional disability = 0.003 (subdomains: ADL = 0.46, IADL = 0.01, general physical = 0.13, mobility = 0.29, social = 0.04). Weighted prevalence rates are age-adjusted to the 2000 US population.
Racial differences in hypertension
African Americans with hypertension had the highest age-adjusted prevalence of subjective cognitive (African Americans with hypertension: 11% and without hypertension: 7%; Whites with hypertension: 7% and without hypertension: 5%; Mexican Americans with hypertension: 8% and without hypertension: 8%; P = 0.01) and functional (African Americans with hypertension: 27% and without hypertension: 17%; Whites with hypertension:23% and without hypertension: 14%; Mexican Americans with hypertension: 22% and without hypertension: 17; P = 0.03) limitations compared to other racial groups with and without hypertension and to African Americans without hypertension as shown in Figure 3. However in all racial groups, hypertensive individuals had higher prevalence of subjective limitations as shown in Figure 3.
Figure 3.

Age-adjusted prevalence of cognitive and functional disability (including the 5 subdomains) by hypertension status in the 3 racial groups (1999–2010). Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living; MA, Mexican Americans. All P-values for non-hypertension vs. hypertension <0.0001 except for cognitive and functional limitations and its subdomains in MA and ADL limitations in all racial groups. P-value for the higher prevalence in African Americans by hypertension status (race × hypertension) was significant for cognitive (P = 0.03), functional (P = 0.01), IADL (P = 0.006), and lower extremity (P = 0.005) limitations. Weighted prevalence rates are age-adjusted to the 2000 US population.
Mortality risk in hypertension and subjective cognitive or functional limitations
Of the 13,422 participants with mortality data, 1,050 died in the period of examination to 31 December 2006 (mean follow-up = 56.4 months, range 0–92). Relative to those with neither hypertension nor subjective cognitive and functional limitations, functional [hazard ratio = 3.6, 95% CI (2.5,5.1)] and cognitive [hazard ratio = 2.6, 95% CI(1.9,3.5)] disabilities were associated with higher mortality risk in hypertension after adjusting for demographics, body mass index, educational level, blood pressure, diabetes mellitus, stroke, congestive heart failure, and cholesterol level. Kaplan–Meier curves are shown in Figure 2. Age-adjusted mortality rates were highest in those who had hypertension and had self-reported functional limitation (10.9 per 100 person-years) or cognitive limitations (12.5 per 100 person-years) relative to those without hypertension or without limitations. These results are shown in Table 2. The impact of the combination of hypertension and physical or cognitive limitations on mortality was also greatest in African Americans (P-values for the impact of race on the hypertension/limitation (race × hypertension/limitation) were 0.0002 for functional limitation and 0.0002 for cognitive limitations after adjusting for the same covariates). Being hypertensive and African American with functional limitations hazard ratio = 1.8, 95% CI (1.3, 2.5) or cognitive limitations hazard ratio = 2.1, 95% CI (1.2, 3.8) were associated with higher mortality relative to the rest of the NHANES sample.
Figure 2.
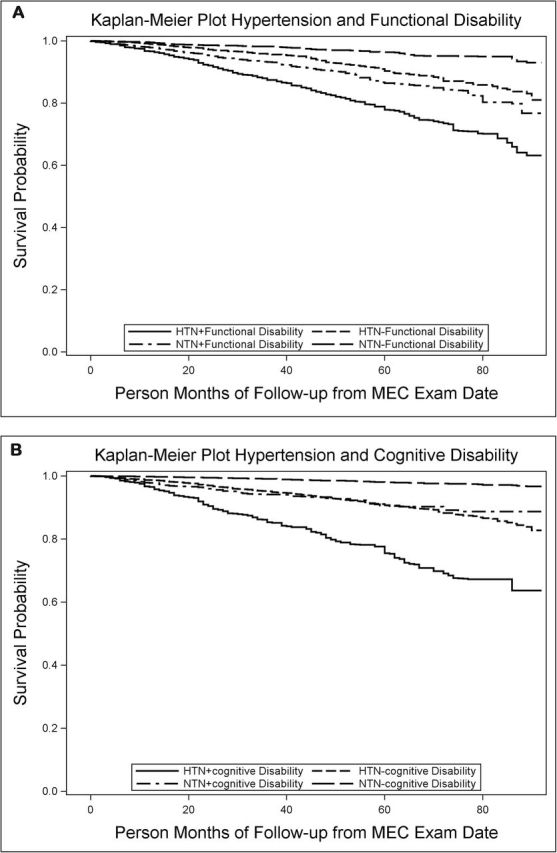
Kaplan–Meier curves for mortality rates by hypertension and cognitive disability (A) and functional (B) status (1999–2004 survey with survival data through 31 December 2006).
Table 2.
Mortality rates (per 100 person-years) and Cox proportional hazard ratios associated with the presence or absence of hypertension and disability in the United States (1999–2004)
| Mortality ratea | SE | Unadjusted HR and 95% CI | Adjustedb HR and 95% CI | P-value | ||||
|---|---|---|---|---|---|---|---|---|
| Functional disability | ||||||||
| No hypertension, no disability | 2.1 | 0.5 | 1.0 | — | 1.0 | — | ||
| No hypertension, with disability | 6.1 | 0.5 | 3.6 | (2.6, 5) | <0.0001 | 3.7 | (2.7, 5.1) | <0.0001 |
| Hypertension, no disability | 5.1 | 1.6 | 2.6 | (1.8, 3.7) | <0.0001 | 1.7 | (1.1, 2.6) | 0.01 |
| Hypertension, with disability | 10.9 | 2.7 | 6.5 | (4.9, 8.7) | <0.0001 | 3.6 | (2.5, 5.2) | <0.0001 |
| Cognitive disability | ||||||||
| No hypertension, no disability | 3.3 | 0.3 | 1.0 | — | — | 1.0 | — | — |
| No hypertension, with disability | 8.4 | 1 | 4.8 | (4.2, 5.9) | <0.0001 | 2.5 | (1.8, 3.4) | <0.0001 |
| Hypertension, no disability | 5.9 | 0.54 | 5 | (4.2, 5.9) | <0.0001 | 1.6 | (1.2, 2.1) | 0.0005 |
| Hypertension,with disability | 12.5 | 1.8 | 14.4 | (11.1, 18.7) | <0.0001 | 2.6 | (1.8, 3.5) | <0.0001 |
Italics are the P-values for the comparison between the hypertension and normotension groups.
a P-value for the difference between the 4 groups is <0.0001 for both cognitive and functional disability.
bAdjusted for age, gender, race, systolic blood pressure, diabetes, stroke, BMI, CHF, cholesterol, and educational level.
Impact of age and sex on disability in hypertension
Although subjective functional and cognitive limitations were higher with advancing age, the prevalence of both was similar between the hypertensive and the non-hypertensive individuals aged 75 years or older. (Figure 4A) Hypertensive participants had higher prevalence than non-hypertensive participants in both sexes, and both hypertensive and non-hypertensive women had higher limitation prevalence than men as shown in Figure 4B.
Figure 4.
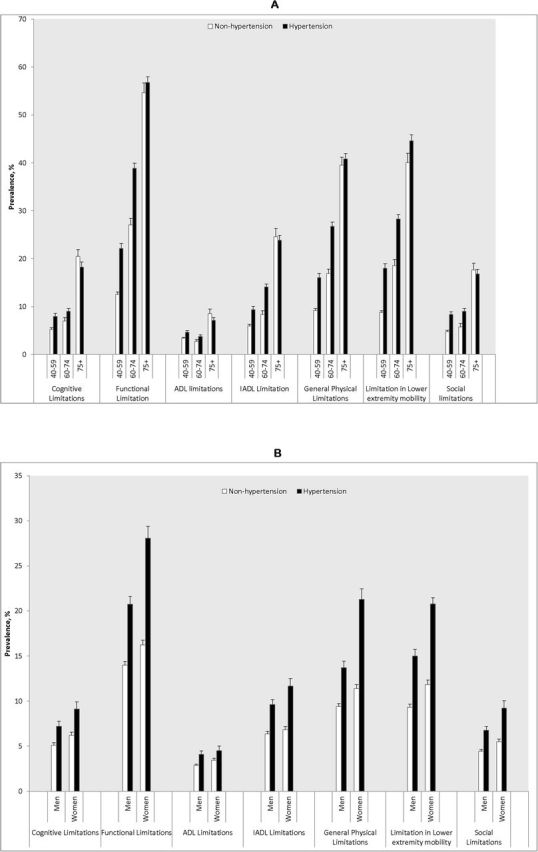
Age-specific and age-adjusted prevalence of cognitive and functional disability (including the 5 functional subdomains) by hypertension status in the 3 age groups (A) and in men and women (B). Abbreviations: ADL: activities of daily living; IADL, instrumental activities of daily living. P-values for non-hypertension vs. hypertension <0.0001 for cognitive and functional limitations in all age groups except for those 75 years or older; and in both genders except for ADL in men (P = 0.003) and women (P = 0.06).
Impact of treatment and systolic blood pressure levels in hypertension
In those with hypertension, there was no association between reporting use of antihypertensive medication and cognitive (covariate-adjusted OR = 0.97, 95% CI (0.79, 1.19), P = 0.7) or functional (covariate-adjusted OR = 0.90, 95% CI (0.78, 1.04), P = 0.16) disability. There was higher age-adjusted prevalence of functional disability with higher systolic blood pressure in untreated hypertension (<140mm Hg: 9%, 140–149mm Hg: 18%, ≥150mm Hg: 24%, P < 0.0001) and treated hypertension (<140mm Hg = 23%, 140–149mm Hg: 24%, and ≥150mm Hg: 24%, P = 0.0005). However, there was no significant association with cognitive disability (untreated: <140mm Hg: 6%, 140–149mm Hg: 6%, ≥150mm Hg: 10%, P = 0.18; treated: <140mm Hg = 10%, 140–149mm Hg: 5%, and ≥150mm Hg: 6%).
DISCUSSION
Our analyses show that hypertension is associated with greater burden of subjective cognitive and functional limitations in the US population. This burden has increased over the last decade despite relatively constant hypertension prevalence.
It is well established that African Americans have more prevalent and more fulminant forms of hypertension.8 Our study is the first to report from a population perspective that African Americans with hypertension may carry a disproportionate burden of cognitive and functional disability relative to non-hypertensive African Americans or non-African Americans. They also have disproportionate mortality burden from the combination of hypertension and functional or cognitive limitations. As such, our findings highlight the clinical relevance of self-reported cognitive and functional limitations. African Americans are more likely to suffer from cognitive deficits and dementia as well as physical disability14,15 and have worse hypertension-related complications.16,17
Subjective cognitive impairment has been recently recognized as a potential indicator for future cognitive decline and dementia.9 Our study also suggests that subjective cognitive limitations are linked to all-cause mortality in hypertension. Taken together, our study reinforces the need for evaluating and monitoring those with subjective cognitive symptoms especially in those who have concomitant hypertension.
We1 and others18 have reported the increased risk of functional disability in hypertension. Our analysis shows that the prevalence of self-reported limitations in cognition or physical functioning in the United States has increased over the last decade to a larger extent in the hypertensive population compared to the rest of the adult US population. This suggests that despite the stabilization of hypertension prevalence and improvement in hypertension detection and control in the last decade, the number of hypertensive people with disability has continued to increase.19 Considering these findings, there is a dimension of the effects of hypertension on the population that has been largely ignored, namely cognition and functional abilities. This has extensive implications for society and large-scale health economics in this country.
The clinical significance of our findings is that those with hypertension and self-reported disability in the cognitive or functional domains are at increased mortality risk. Both hypertension without disability and disability without hypertension were associated with increased mortality. Within the hypertension group, reporting either disability increases all-cause mortality. Screening and identifying persons with self-reported cognitive or functional limitations using brief questions such as those used in NHANES may offer information about the future risk of death. Those individuals can be risk stratified and may be candidates for clinical trials or interventions to ameliorate these limitations. They should be monitored closely for future complications as their mortality risk is high.
Hypertension is associated with white matter hyperintensities in the brain,20 cerebral hypoperfusion,21 neurovascular inflammation,22 and decreased balance and gait speed.23 These may offer pathophysiological explanations of our findings.
Our study suggests that disability is also a significant problem in middle age hypertensive individuals. Most disability studies have focused on older adults. We observed that although disability was significantly higher in those 75 years or older; it is not different between normotensive and hypertensive individuals. These results may be related to the competing risk phenomenon or to survival bias. They also highlight the need to address cognitive and physical limitations in hypertension in midlife.
A major strength of this study is that it includes a large representative sample of the US population and includes mortality follow-up data. This is the first study to provide a snap-shot of the magnitude of disability in the hypertensive population. A limitation of our study is the self-reported nature of limitations in NHANES. This is particularly relevant in those who may have subjective cognitive impairment. Self-report is a common method to assess disability and is the main method of obtaining information in the clinical setting. Self-rated health status is an independent predictor of morbidity and mortality.24,25 Another limitation is that blood pressure was measured at a single event, which may lead to an error in the estimation of hypertension prevalence. Another limitation is the use of a single question to assess cognitive limitations. The validity of this single question is supported by the strong correlation between self-reported cognitive limitations and digit symbol substitution test performance. Finally, the potential for residual confounding that we failed to include or was not assessed in NHANES is another limitation.
Hypertension is associated with greater subjective cognitive and functional disability in the US population, which in turn is associated with greater mortality. Hypertensive African Americans carry the largest burden of both types of disability. Despite improvement in hypertension treatment and control over the last decade, the number of hypertensive individuals reporting limitations has increased. Targeted interventions in hypertension to decrease this high disability burden are a public health priority especially in African Americans.
SUPPLEMENTARY MATERIAL
Supplementary materials are available at American Journal of Hypertension (http://ajh.oxfordjournals.org).
DISCLOSURE
The authors declared no conflict of interest.
Supplementary Material
ACKNOWLEDGMENTS
I.H. was funded by the National Institute of Aging (R01AG042127). W.W. was funded by NIA (K01AG042498). W.J.M. was funded by NIH (UL1TR000130). A.L. and F.C.G. were funded by the Emory Alzheimer’s Disease Research Center (P50 AG025688).
REFERENCES
- 1. Hajjar I, Lackland DT, Cupples LA, Lipsitz LA. Association between concurrent and remote blood pressure and disability in older adults. Hypertension 2007; 50:1026–1032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Köhler S, Baars MA, Spauwen P, Schievink S, Verhey FR, van Boxtel MJ. Temporal evolution of cognitive changes in incident hypertension: prospective cohort study across the adult age span. Hypertension 2014; 63:245–251. [DOI] [PubMed] [Google Scholar]
- 3. Faraco G, Iadecola C. Hypertension: a harbinger of stroke and dementia. Hypertension 2013; 62:810–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Mitchell AJ, Beaumont H, Ferguson D, Yadegarfar M, Stubbs B. Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: meta-analysis. Acta Psychiatr Scand 2014; 130:439–451. [DOI] [PubMed] [Google Scholar]
- 5. Jessen F, Wiese B, Bachmann C, Eifflaender-Gorfer S, Haller F, Kölsch H, Luck T, Mösch E, van den Bussche H, Wagner M, Wollny A, Zimmermann T, Pentzek M, Riedel-Heller SG, Romberg HP, Weyerer S, Kaduszkiewicz H, Maier W, Bickel H; German Study on Aging, Cognition and Dementia in Primary Care Patients Study Group. Prediction of dementia by subjective memory impairment: effects of severity and temporal association with cognitive impairment. Arch Gen Psychiatry 2010; 67:414–422. [DOI] [PubMed] [Google Scholar]
- 6. Brault M. Americans with Disabilities: 2010. Current Population Reports. U.S. Department of Commerce Economics and Statistics Administration; US Census Bureau, 2012, pp. 70–131. [Google Scholar]
- 7. Sheats N, Lin Y, Zhao W, Cheek DE, Lackland DT, Egan BM. Prevalence, treatment, and control of hypertension among African Americans and Caucasians at primary care sites for medically under-served patients. Ethn Dis 2005; 15:25–32. [PubMed] [Google Scholar]
- 8. Flack JM. The epidemiology of hypertension and related conditions in the African-American population. J Natl Med Assoc 1995; 87:606–609. [PMC free article] [PubMed] [Google Scholar]
- 9. Reisberg B, Shulman MB, Torossian C, Leng L, Zhu W. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement 2010; 6:11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. NCHS. National Health and Nutrition Examination Survey Data. Centers for Disease Control and Prevention. National Center for Health Statistics (NCHS): Hyattsville, MD, 2013. [Google Scholar]
- 11. Johnson C, Paulose-Ram R, Ogden CL. National Health and Nutrition Examination Survey: analytic guidelines, 1999–2010. Vital Health Stat 2013; 2:7–13. [PubMed] [Google Scholar]
- 12. Klein RJ, Schoenborn CA. Age Adjustment Using the 2000 Projected US Population: Healthy People 2010Statistical Note, Centers for Disease Control and Prevention, DHHS, 2001. [PubMed] [Google Scholar]
- 13. Rothman KJ Greenland S and Lash TL. Modern epidemiology, 3rd ed. Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA; 2008. [Google Scholar]
- 14. Fuller-Thomson E, Nuru-Jeter A, Minkler M, Guralnik JM. Black-White disparities in disability among older Americans: further untangling the role of race and socioeconomic status. J Aging Health 2009; 21:677–698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Demirovic J, Prineas R, Loewenstein D, Bean J, Duara R, Sevush S, Szapocznik J. Prevalence of dementia in three ethnic groups: the South Florida program on aging and health. Ann Epidemiol 2003; 13:472–478. [DOI] [PubMed] [Google Scholar]
- 16. Batson B, Belletti D, Wogen J. Effect of African American race on hypertension management: a real-world observational study among 28 US physician practices. Ethn Dis 2010; 20:409–415. [PubMed] [Google Scholar]
- 17. Post WS, Hill MN, Dennison CR, Weiss JL, Gerstenblith G, Blumenthal RS. High prevalence of target organ damage in young, African American inner-city men with hypertension. J Clin Hypertens (Greenwich) 2003; 5:24–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Pinsky JL, Branch LG, Jette AM, Haynes SG, Feinleib M, Cornoni-Huntley JC, Bailey KR. Framingham Disability Study: relationship of disability to cardiovascular risk factors among persons free of diagnosed cardiovascular disease. Am J Epidemiol 1985; 122:644–656. [DOI] [PubMed] [Google Scholar]
- 19. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010; 303:2043–2050. [DOI] [PubMed] [Google Scholar]
- 20. van Dijk EJ, Breteler MM, Schmidt R, Berger K, Nilsson LG, Oudkerk M, Pajak A, Sans S, de Ridder M, Dufouil C, Fuhrer R, Giampaoli S, Launer LJ, Hofman A; CASCADE Consortium. The association between blood pressure, hypertension, and cerebral white matter lesions: cardiovascular determinants of dementia study. Hypertension 2004; 44:625–630. [DOI] [PubMed] [Google Scholar]
- 21. Muller M, van der Graaf Y, Visseren FL, Mali WP, Geerlings MI; SMART Study Group. Hypertension and longitudinal changes in cerebral blood flow: the SMART-MR study. Ann Neurol 2012; 71:825–833. [DOI] [PubMed] [Google Scholar]
- 22. Morillas P, de Andrade H, Castillo J, Quiles J, Bertomeu-González V, Cordero A, Tarazón E, Roselló E, Portolés M, Rivera M, Bertomeu-Martínez V. Inflammation and apoptosis in hypertension. Relevance of the extent of target organ damage. Rev Esp Cardiol (Engl Ed) 2012; 65:819–825. [DOI] [PubMed] [Google Scholar]
- 23. Hausdorff JM, Herman T, Baltadjieva R, Gurevich T, Giladi N. Balance and gait in older adults with systemic hypertension. Am J Cardiol 2003; 91:643–645. [DOI] [PubMed] [Google Scholar]
- 24. Centers for Disease C and Prevention. Racial/ethnic disparities in self-rated health status among adults with and without disabilities--United States, 2004–2006. MMWR 2008; 57:1069–1073. [PubMed] [Google Scholar]
- 25. Lee SJ, Moody-Ayers SY, Landefeld CS, Walter LC, Lindquist K, Segal MR, Covinsky KE. The relationship between self-rated health and mortality in older black and white Americans. J Am Geriatr Soc 2007; 55:1624–1629. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.