

Abstract
Study Objectives:
We investigated cross-sectional associations of individual-level socioeconomic position (SEP) and neighborhood characteristics (social cohesion, violence, problems, disadvantage) with sleep duration and sleep quality in 5,301 African Americans in the Jackson Heart Study.
Methods:
All measures were self-reported. Sleep duration was assessed as hours of sleep; sleep quality was reported as poor (1) to excellent (5). SEP was measured by categorized years of education and income. Multinomial logistic and linear regression models were fit to examine the associations of SEP and neighborhood characteristics (modeled dichotomously and tertiles) with sleep duration (short vs. normal, long vs. normal) and continuous sleep duration and quality after adjustment for demographics and risk factors.
Results:
The mean sleep duration was 6.4 ± 1.5 hours, 54% had a short (≤ 6 h) sleep duration, 5% reported long (≥ 9 h) sleep duration, and 24% reported fair to poor sleep quality. Lower education was associated with greater odds of long sleep (odds ratio [OR] = 2.19, 95% confidence interval [CI] = 1.42, 3.38) and poorer sleep quality (β = −0.17, 95% CI = −0.27, −0.07) compared to higher education after adjustment for demographics and risk factors. Findings were similar for income. High neighborhood violence was associated with shorter sleep duration (−9.82 minutes, 95% CI = −16.98, −2.66) and poorer sleep quality (β = −0.11, 95% CI = −0.20, 0.00) after adjustment for demographics and risk factors. Results were similar for neighborhood problems. In secondary analyses adjusted for depressive symptoms in a subset of participants, most associations were attenuated and only associations of low SEP with higher odds of long sleep and higher neighborhood violence with poorer sleep quality remained statistically significant.
Conclusions:
Social and environmental characteristics are associated with sleep duration and quality in African Americans. Depressive symptoms may explain at least part of this association.
Citation:
Johnson DA, Lisabeth L, Hickson D, Johnson-Lawrence V, Samdarshi T, Taylor H, Diez Roux AV. The social patterning of sleep in African Americans: associations of socioeconomic position and neighborhood characteristics with sleep in the Jackson Heart Study. SLEEP 2016;39(9):1749–1759.
Keywords: sleep duration, sleep quality, African American, socioeconomic status, neighborhood characteristics, Jackson Heart Study
Significance.
African Americans have poorer sleep quality and lower mean sleep duration compared to other racial groups. Individual-level social and environmental factors may contribute to poor sleep outcomes in this population but yet are understudied. This is the first paper to investigate both individual-level socioeconomic position (SEP) and neighborhood characteristics (individual and census tract-level) with sleep duration and sleep quality in a large sample of African Americans. Our results demonstrated that both SEP and neighborhood violence and problems were associated with poor sleep duration and sleep quality, thus providing insight into the social determinants of sleep in African Americans. Future studies should consider longitudinal analyses to determine the pathways by which individual SEP and neighborhoods influence sleep duration and quality.
INTRODUCTION
Inadequate sleep is a growing public health concern. The National Sleep Foundation suggests that most adults require 7–8 hours of sleep per night.1 Short (< 7 h) or long (≥ 9 h)2 sleep duration and a poor quality of sleep can interrupt the health promoting functions that occur during sleep, which can lead to poor health outcomes.3 Although sleep is essential for physical and emotional well-being,4 data from large nationally representative samples of United States (US) adults indicate that between 28% to 37% of adults sleep 6 hours or fewer, while approximately 8% sleep 9 hours or more.5–7 Data from the same studies also show an alarming 35% to 53% of non-Hispanic African Americans sleep 6 hours or less and approximately 10% sleep 9 hours or more.5–7
Research has shown that short or long sleep and poor sleep quality are risk factors for several health conditions including high blood pressure, diabetes, stroke, obesity, depression, heart disease, and mortality.4,6,8–10 It has been hypothesized that the altered blood pressure profile resulting from insufficient sleep may lead to cardiovascular damage and increased risk for cardiovascular disease (CVD).11 Sleep has also been linked to metabolic disturbances related to CVD.12 Preliminary evidence shows that improving sleep can improve glucose homeostasis and blood pressure.13,14 With at least a third of Americans sleeping 6 hours or less per night,6 explorations of the reasons for this high prevalence of inadequate sleep are warranted in order to develop appropriate interventions to improve sleep and reduce the downstream cardiovascular consequences, particularly among African Americans who have been infrequently studied.
Growing research indicates that African Americans have poorer sleep quality, lower mean sleep duration, and a higher prevalence of sleep-disordered breathing when compared to non-Hispanic whites.15,4,12,16 However, the reasons for this racial disparity remain unclear.17 Low socioeconomic position (SEP) may contribute to poorer sleep outcomes in African Americans through occupational characteristics (such as shift work or long hours), behavioral factors patterned by SEP that may affect sleep (like physical activity or dietary behaviors), or exposures to stressors that may lead to poor sleep.18–20 Several studies have shown shorter sleep and poor quality sleep are associated with lower SEP as indexed by education, family income, poverty, employment status, private insurance, and food security.19,21–25 However, the majority of work examining associations of SEP with sleep has focused on white populations, and associations may differ for African Americans because they may be more vulnerable to the impact of SEP on sleep.21,26 For example, some studies have reported that, in contrast to associations reported in white men and women, among African American men increases in SEP are sometimes associated with adverse health outcomes.26–28 Therefore, studying the associations between SEP and sleep outcomes in African Americans is warranted.
In addition to individual measures of SEP, neighborhood characteristics may also affect sleep outcomes. The effects of light, noise, and traffic, which are often patterned by neighborhood, on sleep outcomes are well established.29–31 Low SEP neighborhoods may also have increased exposure to crime and air pollution that could affect residents' sleep patterns.16,32 The neighborhood social environment (social cohesion, crime, disorder) may affect the initiation or regulation of sleep33–37 through activation of the stress response process and the release of stress hormones that hinder sleep.33 Several studies conducted among pediatric populations have shown that living in a socioeconomically disadvantaged neighborhood is associated with sleep problems, inadequate sleep quality, and a short sleep duration.38–40 Similar evidence linking neighborhood attributes such as neighborhood SEP, social cohesion, disorder, and violence to sleep outcomes is emerging for adult populations16,34,37,41; however, these studies are limited by small sample size, a lack of racial-ethnic diversity, and consideration of single dimensions of the neighborhood environment. Because of the increased exposure of African Americans to adverse neighborhood environments, these factors could contribute to poor sleep outcomes in this population.36
Given the limited data on African Americans and sleep, exploring predictors (at the individual and neighborhood levels) of sleep in this population may inform interventions to improve sleep and related chronic conditions in this population. Using data from the Jackson Heart Study (JHS) we studied the cross-sectional associations of individual-level SEP and neighborhood characteristics (social cohesion, violence, problems, SEP) with sleep duration and sleep quality in African Americans. We hypothesized that low SEP and adverse neighborhood conditions would be associated with both short and long sleep duration and with worse sleep quality.
METHODS
The JHS is a large population-based, prospective cohort study designed to examine the etiology of cardiovascular disease in African Americans. The 5,301 participants aged 21 to 95 years were recruited from 3 counties—Hinds, Madison, and Rankin—in the Jackson, Mississippi (MS), metropolitan statistical area (MSA) between September 2000 and March 2004 using 4 approaches.42 First, all the Jackson, MS, living participants in the Atherosclerosis Risk in Community (ARIC) study within the eligible age range were invited to participate in JHS. Jackson ARIC participants were originally sampled from the city of Jackson residents listed in the Mississippi Driver's License and Identification List.42 In total, 31% of the JHS participants were recruited from the ARIC study. Second, participants were recruited through random sampling (17% of the total JHS sample) from a commercially available list (AccuData Integrated Marketing, Fort Myers, FL) of all community residents aged 35–84 years in the tri-county area.43 The third approach recruited volunteers (30% of the total JHS sample) aged 35–84 years through targeted advertisements: radio, newspaper, local churches, and civic/social organizations.43 Volunteers were approximately representative of the Jackson MSA African American population in terms of age, sex, and socioeconomic characteristics.44 Lastly, family members of other JHS participants (22% of the total JHS sample) were recruited from enumerated households to permit future genetic studies.45 Family members were included even if they were under 35 or over 84 years of age. The final study sample has been shown to be geographically representative of the age-eligible African American population in the Jackson MSA.46 The JHS was approved by the institutional review boards of Jackson State University, Tougaloo College, and University of Mississippi Medical Center. All participants provided written informed consent.
Of the 5,301 participants enrolled in the JHS study, 5,244 had data on sleep quality and sleep duration. Of these, 19 were missing information on education leaving 5,225 available for individual-level SEP analyses. The 804 participants with missing information on income were coded as missing and retained in analyses. Analyses based on self-reported neighborhood characteristics were further restricted to 3,260 participants who reported this information. Analyses adjusted for sleep risk factors were further restricted to 4,063 participants for individual-level SEP and 2,550 participants for self-reported neighborhood characteristics due to missing covariate data. A total of 5,215 participants had information on census tract-level neighborhood characteristics and were included in analyses of census tract SEP (n = 4,063 for risk factor adjusted analyses) and in sensitivity analyses pooling survey responses within tracts, as described below.
Sleep Measures
Self-reported sleep measures, including sleep duration and sleep quality were collected at baseline between 2000 and 2004. To assess sleep duration, participants responded to the following question: “During the past month, excluding naps, how many hours of actual sleep did you get at night (or day, if you work at night) on average?” Responses were given in hours and transformed into minutes for analysis. Sleep duration was also categorized into short (≤ 6 h), normal (7 or 8 h), and long (≥ 9 h) sleep.47,48 The analyses included both continuous (in minutes) and categorized (short, normal, and long) measures of sleep duration. Participants also indicated their level of sleep quality by responding to the following question, “During the past month, how would you rate your sleep quality overall?” Responses were reported on a Likert scale, with 1 = excellent, 2 = very good, 3 = good, 4 = fair, 5 = poor; coding was reversed for analysis and further categorized as high (excellent, very good, good) and low (fair, poor).
Individual-level Measures of SEP
Individual-level SEP was measured by education and income. Education was reported at baseline as the years of schooling completed (range = 0–16+ years) and categorized into 4 groups: less than high school, high school, greater than high school (HS) but less than a college degree, and college degree or more. Annual family income was reported at baseline in 11 categories ranging from under $5,000 to $100,000 or more. Income was then further classified into 4 categories: low, lower-middle, upper-middle, and affluent which were based upon income, family size, number of children < 18 years of age, and the United States Census designated poverty level for the year in which the income information was obtained.43 Low income was defined as income below the poverty level. Lower-middle income was defined as income at or above the poverty level but below 2.5 times the poverty level.43 Upper-middle income was defined as income ≥ 2.5 times the poverty level, but below 4 times the poverty level.43 High income was defined as income at ≥ 4 times the poverty level. Participants who did not know their income or refused to respond were classified as “Unknown.” A continuous family income variable was also created by taking the interval midpoint of each family income bracket (e.g., the midpoint for $5,000–$7,999 is $6,500).43 Those who reported total family income of < $5,000 were assigned a value of $2,500 and those with > $100,000 were assigned $112,500 based on the US income distribution.
Neighborhood Measures
JHS participants completed a survey about their neighborhood between 2004 and 2010. Participants were asked questions about their neighborhood defined as the area around where they live, perform routine tasks, such as shopping, going to the park, visiting neighbors, religious or public institutions, or a local business district. Neighborhood social cohesion was measured as the mean of 5 items with 4 response options ranging from strongly disagree (1) to strongly agree (4). The 5 items included this is a close knit neighborhood, people are willing to help their neighbors, people in the neighborhood generally don't get along (reverse coded), people in the neighborhood can be trusted, and people in the neighborhood do not share the same values (reverse coded). Neighborhood violence was measured as the mean of 5 items that assessed the frequency with which acts of violence occurred in the last 6 months (1 = Never to 4 = Often): a fight in the neighborhood in which a weapon was used, a violent argument between neighbors, gang fights, a sexual assault or rape, or a robbery or mugging. Neighborhood problems were measured as the mean of six items (1 = Not really a problem to 4 = Very serious problem) that assessed aspects of the neighborhood (noise, traffic, trash/litter, availability of health foods, parks, lack of parks, and playground).49,50 Scales were identified a priori (based on the literature) and confirmed via principal component analysis (PCA) of all 17 items. Each neighborhood scale had good internal consistency, with Cron-bach α ranging from 0.76–0.80. Main analyses focused on self-reports of neighborhood characteristics. However, in sensitivity analyses we also examined census tract-level neighborhood characteristics created by aggregating responses within a tract over the period 2004–2008 using age and sex adjusted empirical Bayes estimates as described in prior work.49 Briefly, the empirical Bayes estimates were calculated using three-level multilevel models. These estimates adjust for systematic variations in response to perceived neighborhood conditions by age and sex and also improve unreliable estimates for locations with a small number of respondents by shrinking them towards an overall mean. The use of census tract-level estimates avoids same source bias (and may provide a more valid estimate of “true” neighborhood characteristics) but does not capture an individual's subjective perception.
In addition to the survey based scales, we also investigated a neighborhood SEP measure (hence forth referred to as neighborhood disadvantage) developed using data from the 2000 US Census that was based on a score derived from PCA of US census tract-level data.51 The factor score is a sum of standardized proportions for several socioeconomic indicators for adults in the tracts, including the % with a Bachelor degree, % in managerial occupations, median home value, % with a high school (HS) education, median household income, and % of households with income greater than $50,000. Higher factor scores indicated greater neighborhood disadvantage. In order to investigate trends, all neighborhood characteristics were categorized into tertiles. Dichotomous categories were used when the distribution precluded the creation of tertiles (as for neighborhood violence).
Covariates
Participants self-reported age, sex, and marital status which may confound the associations between both individual SEP and neighborhood characteristics with sleep.37 Risk factors for poor sleep outcomes (short sleep, long sleep and shorter sleep duration and lower sleep quality) including body mass index (BMI), hypertension, diabetes, physical activity, and depressive symptoms may confound or mediate the associations between individual SEP, neighborhood characteristics and sleep. For this reason, results are shown before and after adjustment for these covariates. Each of these 5 risk factors was measured by trained study staff. BMI was calculated in kg/m2 using measurements of weight and height while participants wore light clothing and no shoes. Seated blood pressure measurements were obtained after 5 minutes of rest. Two resting blood pressure readings were taken 1 minute apart in the seated position and averaged. Hypertension was defined according to Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VII) criteria as a systolic blood pressure ≥ 140 mm Hg or a diastolic blood pressure ≥ 90 mm Hg, use of antihypertensive medications (self-report and actual) within 2 weeks prior to data collection, or self-reported history of hypertension.52 Diabetes was defined according to American Diabetes Association, 2004 criteria as fasting glucose ≥ 126 mg/dL, confirmed medication inventory or self-reported use of anti-diabetic medications, or self-reported diabetes diagnosis.53 Physical activity was measured using the JHS Physical Activity Measurement instrument, a modified version of the Baecke physical activity survey.54,55 A total physical activity score was calculated based on a summary score of the intensity, frequency, and duration of activities associated with various aspects of life (active living, home life, sport, and work).43
Because depressive symptoms were assessed as part of a follow-up questionnaire and was only available in a subset of participants (n = 3,125), we included depressive symptoms in secondary analyses in this subset only. Depressive symptoms were assessed according to the Centers for Epidemiologic Studies Depression Scale (CES-D). The CES-D is a standardized, 20-item, self-reported instrument that measures the frequency of recently experienced depressive symptoms.56 Participants were asked about their mood over the past week, responding to each item (e.g., “I was bothered by things that usually don't bother me,” “I felt hopeful about the future,” etc.) as to how often they felt “this way.” Item ratings ranged from 0 or “rarely or none of the time,” 1 “some or a little of the time,” 2 “occasionally or a moderate amount of the time,” and 3 “most or all of the time.” Scores range from 0 to 60, with higher scores reflecting greater levels of depressive symptoms while lower scores reflect lower levels of symptoms.
Statistical Analysis
Descriptive statistics were calculated for demographics and risk factors stratified by categories of sleep duration (short [< 7 h], normal [7–8 h], and [long ≥ 9 h]) and sleep quality (high vs. low). Chi-square and analysis of variance tests were used to compare categorical and continuous variables across categories of sleep duration and sleep quality. Pearson correlations were calculated to examine the correlation between sleep outcome variables.
Multinomial logistic regression was used to examine associations of individual SEP and neighborhood characteristics with categories of sleep duration (short vs. normal, long vs. normal). Linear regression was used to examine associations of individual SEP and neighborhood characteristics with continuous sleep outcomes (sleep duration, sleep quality). Neighborhood models included a random intercept for the census tract. The intraclass correlation coefficient (ICC) was calculated to determine clustering within census tract. Individual education and income as well as each neighborhood characteristic were modeled in separate sequential models as follows: unadjusted, followed by adjustment for age, sex, education, and income (neighborhood models only), and further adjustment for marital status, BMI, physical activity, diabetes, hypertension, and physical activity given the potential for these factors to be on the causal pathway. The continuous exposures (individual education and income, neighborhood social cohesion, violence, problems and neighborhood disadvantage) were standardized for ease of interpretation. Tests for trend of the associations between categories of individual SEP and tertiles of neighborhood characteristics and sleep outcomes were performed. In secondary analyses, we conducted the same sequential modeling approach adding additional adjustment for depressive symptoms among the subset of participants that completed the CES-D.
Finally, for significant main effects, we investigated whether the associations of individual SEP and neighborhood characteristics were modified by sex, as previous research has shown sex to modify associations of individual SEP and neighborhood characteristics with health outcomes (i.e. obesity, self-rated health).57–59 Interaction terms between each continuous exposure variable and sex were included in the fully adjusted models. We tested only the continuous exposures in order to reduce the number of statistical tests performed. All analyses were conducted using SAS software version 9.3 (SAS Institute, Cary, NC).
RESULTS
The study population (n = 5,215) had a mean age of 54.7 years (standard deviation = 12.9) and was 63% female. Mean sleep duration was 6.4 ± 1.5 h; 54% of the population had short sleep duration defined as ≤ 6 h of sleep at night, whereas 5% had long sleep duration (≥ 9 h of sleep at night). Approximately 24% of the study population reported “poor sleep.” There was a moderate correlation between sleep duration and sleep quality, r = 0.45, P < 0.01.
Sleep Duration
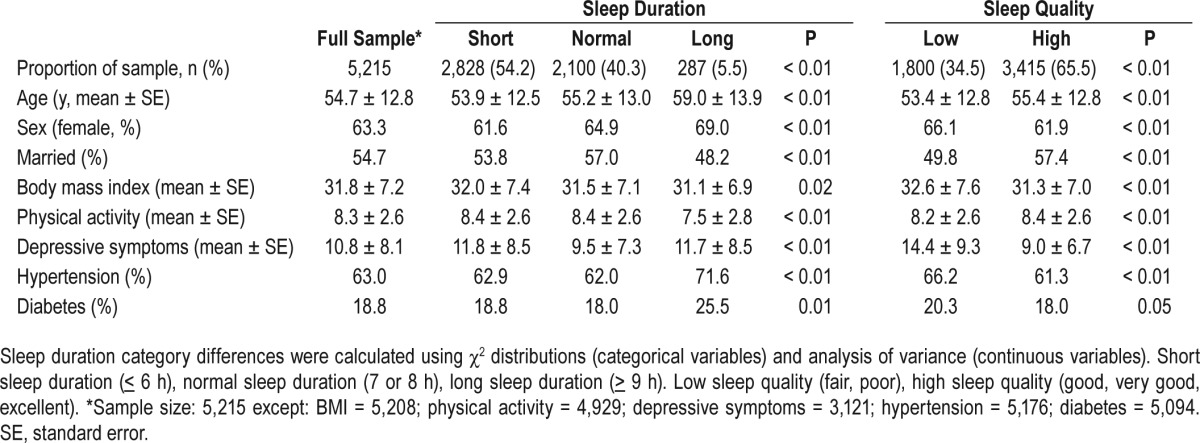
Respondents who reported long sleep were more likely to be older, female, not married, have a lower physical activity score, and a higher prevalence of hypertension and diabetes relative to those in the other sleep categories, P < 0.01 (Table 1). BMI was higher among respondents who reported short sleep compared to those who reported normal and long sleep, P < 0.05 (Table 1).
Table 1.
Sample characteristics by categories of sleep duration and sleep quality, The Jackson Heart Study, 2000–2004.
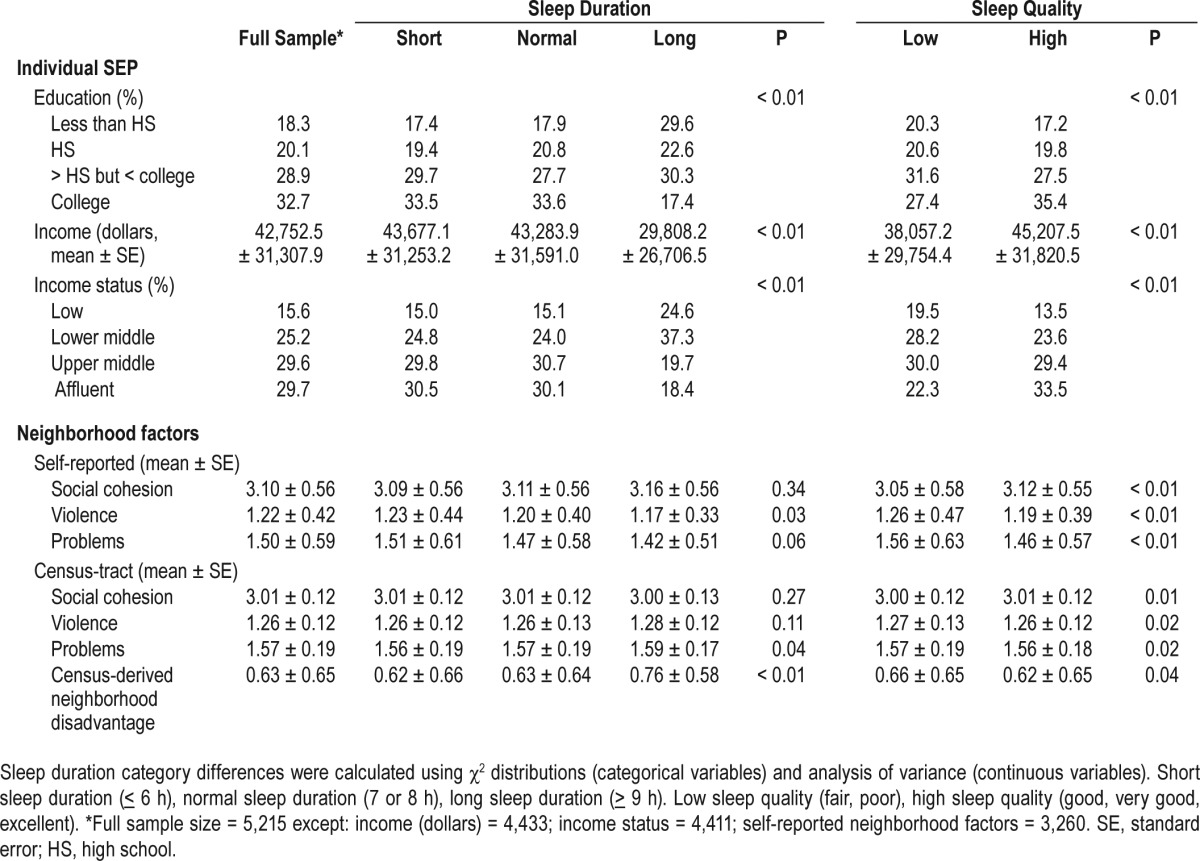
Individuals who reported long sleep were more likely to be of lower education and lower income than those in the other sleep duration categories, P < 0.01; but no important differences in education were observed between short and normal sleepers. Persons in the short sleep category reported higher neighborhood violence relative to those in the other sleep categories, P < 0.05. Mean scores for census-tract level neighborhood problems and neighborhood disadvantage were highest among long sleepers compared to persons in the normal or short sleep categories, P < 0.05. There were no differences in mean self-reported or census-tract level neighborhood social cohesion across sleep duration categories (Table 2).
Table 2.
Individual-level socioeconomic position (SEP) and neighborhood characteristics by categories of sleep duration and sleep quality, The Jackson Heart Study, 2000–2004.
Lower income (low and lower middle) and lower education categories (less than HS, HS/General Educational Development [GED] completers, more than HS but less than bachelor degree) were associated with a higher odds of long sleep compared to high income and college educated adults after age and sex adjustment (Table 3, P for trend < 0.01 for income and education). These associations remained after further adjustment for risk factors (Table 3). Measures of individual SEP were not associated with short sleep or with continuous sleep duration.
Table 3.
Adjusted associations of individual-level socioeconomic position with sleep duration, The Jackson Heart Study, 2000–2004.

Individuals who reported low neighborhood social cohesion had a 36% (odds ratio [OR] = 0.64; 95% CI: 0.41, 0.97) lower odds of long sleep duration relative to those who reported high neighborhood social cohesion after adjustment for age, sex, education, and income. This association was no longer significant after adjustment for risk factors (Table 4). Neighborhood social cohesion was not associated with short sleep or with continuous sleep duration in any model. Persons who reported high neighborhood violence had a 19% (OR = 1.19; 95% CI: 1.01, 1.41) higher odds of short sleep and slept 9.6 minutes (95% CI: −16.52, −2.71) less on average than those who reported lower neighborhood violence after adjustment for age, sex, education, and income (Table 4). Neighborhood violence was not associated with long sleep in any model (Table 4). Individuals in the high category of neighborhood problems slept 10.6 minutes (95% CI: −18.52, −2.64) less than those who reported lower neighborhood problems after adjustment for age, sex, education, and income (P for trend < 0.01). The associations remained after further adjustment for risk factors (Table 4). Neighborhood problems were not associated with odds of short or long sleep duration.
Table 4.
Adjusted associations of neighborhood characteristics with sleep duration, The Jackson Heart Study, 2000–2004.
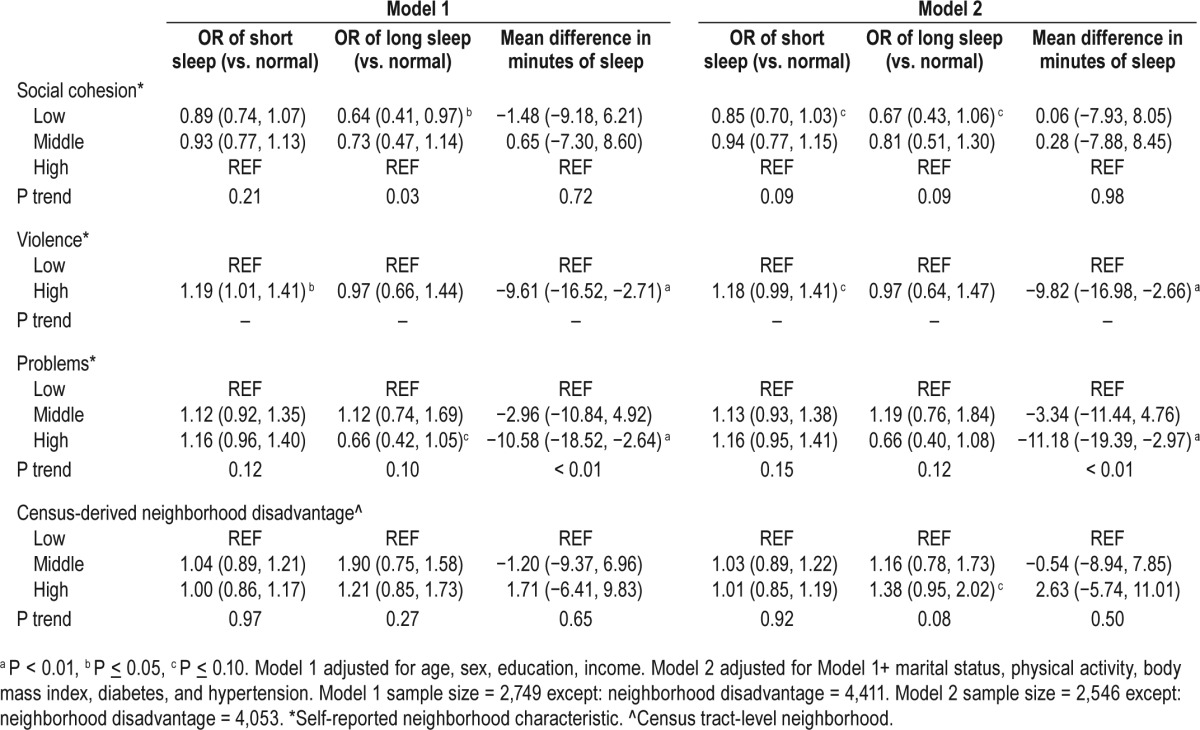
Census-derived neighborhood disadvantage was not significantly associated with any of the sleep outcomes (Table 4).
Sleep Quality
Persons in the low sleep quality group were younger, more likely to be female, not married, had a higher BMI, lower physical activity score, reported more depressive symptoms, and a higher prevalence of hypertension and diabetes compared to those in the high sleep quality group, P < 0.01 (Table 1). They were also more likely to be less educated and to have lower income, reported lower neighborhood social cohesion, higher neighborhood violence, and more neighborhood problems, and lived in neighborhoods with greater disadvantage relative to persons in the high sleep quality group, P < 0.05 (Table 2).
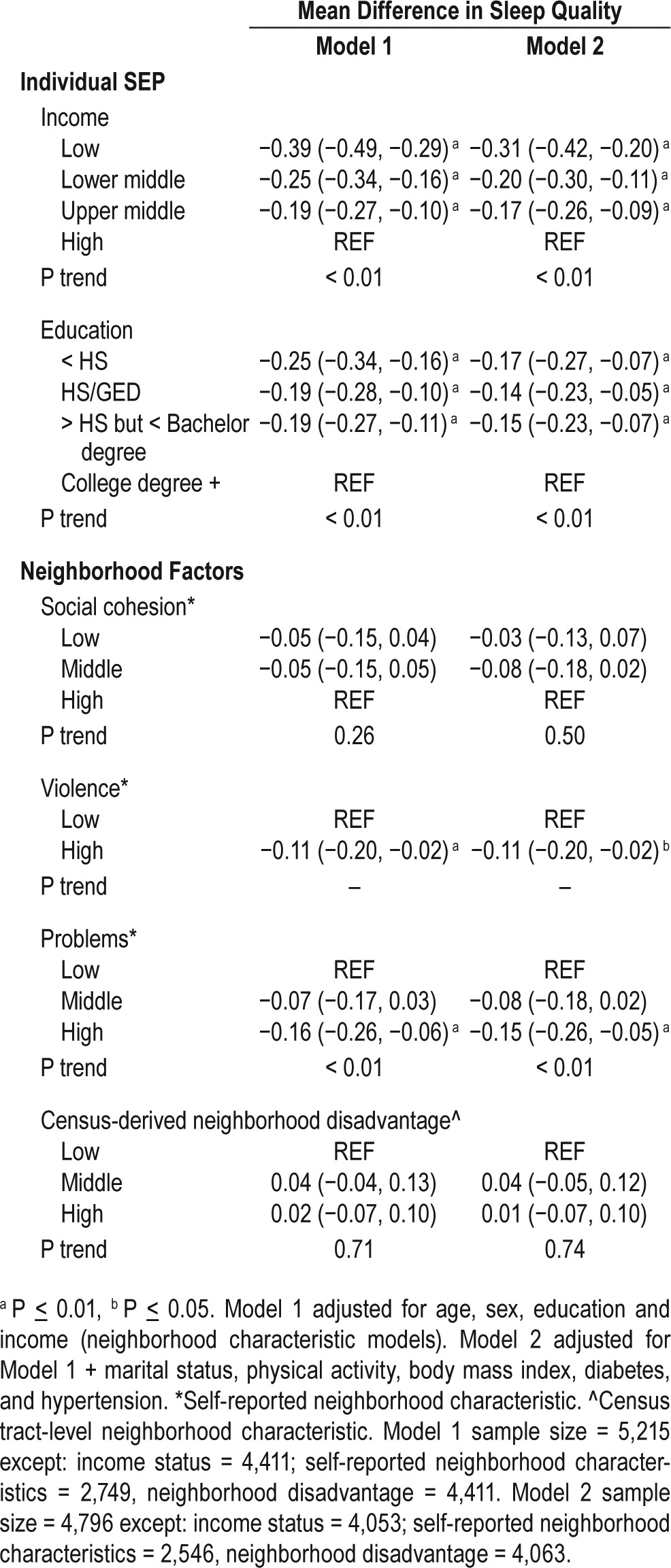
Lower income and lower education were associated with poorer sleep quality in a graded fashion (Table 5, P for trend < 0.01) after adjustment for age and sex. The associations remained after further adjustment for risk factors (Table 5). Individuals who reported more neighborhood violence and neighborhood problems had poorer sleep quality compared to those in the low categories of these factors after adjusting for age, sex, education, and income, although the trend was only statistically significant for neighborhood problems (P < 0.01). These associations remained after further adjustment for risk factors. Neighborhood social cohesion and census-derived disadvantage were not associated with sleep quality in any model (Table 5).
Table 5.
Adjusted associations of individual-level socioeconomic position, neighborhood characteristics with sleep quality, The Jackson Heart Study, 2000–2004.
Effect Modification
The association of neighborhood violence with sleep duration was modified by sex, P ≤ 0.05, such that the association of high neighborhood violence with higher odds of short sleep was observed in males but not females (OR of short sleep for high vs. low neighborhood violence category: OR = 1.44; 95% CI: 1.08, 1.93 in men and OR = 1.02; 95% CI: 0.82, 1.28 in women). Similarly, higher neighborhood violence was associated with shorter continuous sleep duration in males but not in females (mean difference: −9.2 min; 95% CI: −14.33, −4.12 in men and −0.71 minutes; 95% CI: −5.48, 4.06 in women). Sex also modified the association of individual level education with sleep quality, P = 0.05. Among females, higher education was associated with better sleep quality (0.08 units of sleep quality [95% CI: 0.05, 0.12]), compared to the null association observed for males (0.03 units of sleep quality [95% CI: −0.02, 0.08]). Tests for effect modification by sex revealed no statistically significant differences in associations of neighborhood problems, social cohesion, or census-derived disadvantage and individual-level SEP with sleep duration or sleep quality.
Secondary Analysis among JHS Participants with CES-D Data
Consistent with the primary analysis, lower income (low and lower middle) and lower education categories (less than HS, HS/GED completers, more than HS but less than bachelor degree) were associated with a higher odds of long sleep compared to high income and college educated adults after adjustment for demographics and risk factors in the subset of the population with CES-D data. After further adjustment for depressive symptoms, the associations were attenuated but remained statistically significant (Table S3 in the supplemental material). In fully adjusted models lower education was also associated with a lower odds of short sleep and a longer sleep duration compared to those with a college degree or higher (Table S3).
Neighborhood social cohesion was not associated with odds of long sleep in the subsample. Similar to the primary analysis, individuals reporting high neighborhood violence slept 9.9 min (95% CI −18.7, −1.03) less on average compared to those reporting low neighborhood violence after adjustment for demographics and risk factors (Table S4 in the supplemental material). After adjustment for depressive symptoms, this association was attenuated and no longer significant. Contrary to the primary analysis, neighborhood problems were not associated with sleep duration after adjustment for demographics and risk factors.
Associations of individual SEP and neighborhood characteristics (except neighborhood problems) with sleep quality were similar to the primary analysis after adjustment for demographics and socioeconomic status (Table S5 in the supplemental material). However, with further adjustment for depressive symptoms, individual SEP was no longer associated with sleep quality, but the association with neighborhood violence persisted (Table S5).
Sensitivity Analysis
The use of aggregate census tract-level measures of survey responses for social cohesion, violence, and problems resulted in generally weaker associations: no associations were observed between census tract-level neighborhood violence and short sleep or sleep quality or between census tract-level neighborhood problems and continuous sleep or sleep quality (Tables S1 and S2 in the supplemental material).
DISCUSSION
We found that lower individual SEP was associated with higher odds of long sleep and poorer sleep quality after adjusting for demographics and sleep risk factors. Neighborhood characteristics were also associated with sleep duration and quality. Specifically, higher neighborhood violence and more neighborhood problems were generally associated with shorter sleep duration and poorer sleep quality, after adjustment for demographics, individual SEP and risk factors. This study is the first to investigate individual SEP and specific features of the neighborhood environment (individual and census tract-level) with sleep duration and quality within a large population of African Americans. The findings have potential implications for the health of African Americans given both short and long sleep are associated with mortality and cardiovascular outcomes.60
Although associations between lower SEP (income and education) and sleep (duration and quality) have been documented in non-Hispanic white populations,21–24,61,62 our study confirmed this finding in a large population of African Americans. There may be specific correlates of SEP that are driving the observed associations with poor sleep. For example, persons with lower SEP are more likely to work long hours, multiple jobs, and shift work; these conditions are also associated with poorer sleep quality.63,64 Other factors including psychosocial factors such as depressive symptoms may also partially explain the association.65 Researchers have shown that low SEP is associated with depressive symptoms, particularly among African Americans.66 In secondary analyses in a subset of JHS participants with available data on depressive symptoms we found that depressive symptoms did not fully explain associations of low SEP with long sleep but did explain associations of low SEP with poorer reported sleep quality. Our results are therefore consistent with a mediating role of depressive symptoms on the associations of low SEP with poorer sleep quality.
Interestingly, our results show low SEP is associated with higher odds of long sleep and poorer sleep quality. Research has shown that long sleep increases the risk of obesity, diabetes, stroke, heart disease, and mortality.9,67,68 Long sleep duration may also represent poor sleep quality,69 which may explain our findings.
We also found that higher neighborhood violence and problems were associated with shorter sleep duration and poorer quality after adjustment for individual SEP. Our study moved beyond the frequently studied physical environment factors, such as noise and traffic,29–31 and showed that multiple social features of the neighborhood may be important predictors of sleep outcomes within African Americans. Our results were largely consistent with emerging evidence from a few studies that have shown that aspects of the social environment are associated with sleep.34,37,41,70 Researchers have hypothesized that inadequate or prolonged sleep durations may result from life/ psychosocial stressors (working night shifts, multiple jobs)71 or depression that inhibit falling asleep or maintaining sleep among residents of disadvantaged and urban neighborhoods.16
In our secondary analysis we found that the associations of neighborhood violence with sleep duration and sleep quality were attenuated but associations with quality remained statistically significant after further adjustment for depressive symptoms. Neighborhood problems were not associated with sleep duration or quality before or after adjustment for depressive symptoms in the subsample. Depression may partially explain the association between some aspects of the neighborhood environment and sleep duration and/or quality. It is also possible that individuals that are depressed or live in poorer neighborhood conditions may report poorer sleep and poorer outcomes. Future research should consider the mediating effects of psychosocial stressors in longitudinal studies of neighborhoods and sleep.
Our data allowed us to contrast associations observed using individual reports of neighborhood problems and violence (main analyses reported) to associations observed when survey measures were aggregated across tracts. In general, associations using census tract-level measures were attenuated compared to those observed using self-reported measures. Our results suggest that individual perceptions of the environment may influence sleep more than “objective” measures which are more closely approximated by aggregating the perceptions for multiple respondents. This finding is consistent with other studies that have shown self-reported neighborhood characteristics to influence sleep.70,72 However, in the current study, the neighborhood survey scores were pooled across a 5-year period, possibly introducing important measurement error which could also have contributed to weaker associations using these measures.
In an exploratory analysis we found that neighborhood violence was associated with sleep duration in men but not women. Prior studies have not shown sex to modify the associations between neighborhood social factors and sleep duration, although power to test effect modification was limited.37 Other research has shown that African American men are more likely to be affected by neighborhood violence than others.73 In contrast to the neighborhood measures, we found that education was associated with better sleep quality among females but not males. This finding is consistent with prior research showing higher education is associated with increased sleep efficiency among women.65 Further studies are needed to determine whether these effect modification results are replicable, and if so what the drivers might be.
There are several limitations of our study. Although we measured two sleep outcomes, sleep duration and sleep quality, these are subjective sleep measures, which may correlate poorly with objective measures of sleep.74 Research has shown that sleep duration is often underreported, and this could have resulted in biased estimates.75 Additionally, our measure of sleep duration reflects nocturnal sleep excluding naps which may contribute to total sleep time. Sleep disorders (sleep apnea), shift work, or other psychosocial factors (anxiety or PTSD) may confound the associations investigated in this study. The use of self-reported neighborhood characteristics may introduce same-source bias.
Our study was cross-sectional in design, limiting causal inference. Specifically, it is difficult to determine if the exposure to low SEP or adverse neighborhood conditions preceded poor sleep, and data on how long participants lived in the neighborhood were not available. Residual confounding is possible if there were unmeasured covariates at the individual and/or neighborhood level that were not accounted for in the statistical models. Lastly, our study population was a representative of African Americans in Jackson, Mississippi, and may not be representative of the broader African American population.
In conclusion, our study provides insight into determinants of sleep among African Americans, a group at increased risk for a variety of health conditions linked to poor sleep. Individual SEP as well as specific features of the neighborhood were associated both sleep duration and sleep quality. These findings suggest social and environmental characteristics may contribute to adverse sleep outcomes in African Americans. Future studies should consider longitudinal analyses to determine the pathways by which individual SEP and neighborhoods influence sleep duration and quality.
DISCLOSURE STATEMENT
This was not an industry supported study. This research was supported in part by the Michigan Center for Integrative Approaches to Health Disparities (P60MD002249) funded by the National Institute on Minority Health and Health Disparities; The National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number R01HL071759 and R01HL110068; and the Robert Wood Johnson Foundation Health & Society Scholars program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Jackson Heart Study is supported by contracts HHSN268201300046C, HHSN268201300047C, HHSN268201300048C, HHSN268201300049C, HHSN268201300050C from the National Heart, Lung, and Blood Institute and the National Institute on Minority Health and Health Disparities. The authors have indicated no financial conflicts of interest.
REFERENCES
- 1.National Sleep Foundation. How Much Sleep Do We Really Need? Accessed Sept 3, 2015. Available from: http://www.sleepfoundation.org/article/how-sleep-works/how-much-sleep-do-we-really-need.
- 2.Kronholm E, Sallinen M, Suutama T, Sulkava R, Era P, Partonen T. Self-reported sleep duration and cognitive functioning in the general population. J Sleep Res. 2009;18:436–46. doi: 10.1111/j.1365-2869.2009.00765.x. [DOI] [PubMed] [Google Scholar]
- 3.Colten HR, Altevogt BM, editors. Washington, DC: National Academies Press; 2006. Sleep disorders and sleep deprivation: an unmet public health problem. [PubMed] [Google Scholar]
- 4.National Heart Lung and Blood Institute. Why Is Sleep Important. [Accessed Sept 3, 2015]. Available from: http://www.nhlbi.nih.gov/health/health-topics/topics/sdd/why.html.
- 5.Krueger PM, Friedman EM. Sleep duration in the United States: a cross-sectional population-based study. Am J Epidemiol. 2009;169:1052–63. doi: 10.1093/aje/kwp023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention. Effect of short sleep duration on daily activites-United States, 2005-2009. MMWR Morbid Mortal Wkly Rep. 2011;60:239–42. [PubMed] [Google Scholar]
- 7.Centers for Disease Control and Prevention. Unhealthy sleep-related behaviors --- 12 States, 2009. MMWR Morb Mortal Wkly Rep. 2011;60:233–8. [PubMed] [Google Scholar]
- 8.Chien KL, Chen PC, Hsu HC, et al. Habitual sleep duration and insomnia and the risk of cardiovascular events and all-cause death: report from a community-based cohort. Sleep. 2010;33:177–84. doi: 10.1093/sleep/33.2.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Qureshi AI, Giles WH, Croft JB, Bliwise DL. Habitual sleep patterns and risk for stroke and coronary heart disease: a 10-year follow-up from NHANES I. Neurology. 1997;48:904–11. doi: 10.1212/wnl.48.4.904. [DOI] [PubMed] [Google Scholar]
- 10.Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34:1487–92. doi: 10.5665/sleep.1382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lanfranchi PA, Pennestri M-H, Fradette L, Dumont M, Morin CM, Montplaisir J. Nighttime blood pressure in normotensive subjects with chronic insomnia: implications for cardiovascular risk. Sleep. 2009;32:760–6. doi: 10.1093/sleep/32.6.760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hall MH, Okun ML, Sowers M, et al. Sleep is associated with the metabolic syndrome in a multi-ethnic cohort of midlife women: the SWAN Sleep Study. Sleep. 2012;35:783–90. doi: 10.5665/sleep.1874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Knutson KL. Impact of sleep and sleep loss on glucose homeostasis and appetite regulation. Sleep Med Clin. 2007;2:187–97. doi: 10.1016/j.jsmc.2007.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Silverberg DS, Iaina A, Oksenberg A. Treating obstructive sleep apnea improves essential hypertension and quality of life. Am Fam Physician. 2002;65:229–36. [PubMed] [Google Scholar]
- 15.Chen X, Wang R, Zee P, et al. Racial/ethnic differences in sleep disturbances: the Multi-Ethnic Study of Atherosclerosis (MESA) Sleep. 2015;38:877–88. doi: 10.5665/sleep.4732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hale L, Do DP. Racial differences in self-reports of sleep duration in a population-based study. Sleep. 2007;30:1096–103. doi: 10.1093/sleep/30.9.1096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Durrence HH, Lichstein KL. The sleep of African Americans: a comparative review. Behav Sleep Med. 2006;4:29–44. doi: 10.1207/s15402010bsm0401_3. [DOI] [PubMed] [Google Scholar]
- 18.National Sleep Foundation. Shift work and sleep. [Accessed Sept 3, 2015]. Available from: http://www.sleepfoundation.org/article/sleep-topics/shift-work-and-sleep.
- 19.Moore PJ, Adler NE, Williams DR, Jackson JS. Socioeconomic status and health: the role of sleep. Psychosom Med. 2002;64:337–44. doi: 10.1097/00006842-200203000-00018. [DOI] [PubMed] [Google Scholar]
- 20.Dahlgren A, Kecklund G, Åkerstedt T. Different levels of work-related stress and the effects on sleep, fatigue and cortisol. Scand J Work Environ Health. 2005;31:277–85. doi: 10.5271/sjweh.883. [DOI] [PubMed] [Google Scholar]
- 21.Patel NP, Grandner MA, Xie D, Branas CC, Gooneratne N. “Sleep disparity” in the population: poor sleep quality is strongly associated with poverty and ethnicity. BMC Public Health. 2010;10:475. doi: 10.1186/1471-2458-10-475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Grandner MA, Petrov MER, Rattanaumpawan P, Jackson N, Platt A, Patel NP. Sleep symptoms, race/ethnicity, and socioeconomic position. J Clin Sleep Med. 2013;9:897–905. doi: 10.5664/jcsm.2990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Grandner MA, Patel NP, Gehrman PR, Xie D, Sha D, Weaver T, Gooneratne N. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Med. 2010;11:470–8. doi: 10.1016/j.sleep.2009.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gellis LA, Lichstein KL, Scarinci IC, Durrence HH, Taylor DJ, Bush AJ, Riedel BW. Socioeconomic status and insomnia. J Abnorm Psychol. 2005;114:111–8. doi: 10.1037/0021-843X.114.1.111. [DOI] [PubMed] [Google Scholar]
- 25.Fülöp T, Hickson D, Wyatt SB, et al. Sleep-disordered breathing symptoms among African-Americans in the Jackson Heart Study. Sleep Med. 2012;13:1039–49. doi: 10.1016/j.sleep.2012.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Williams DR, Mohammed SA, Leavell J, Collins C. Race, socioeconomic status, and health: complexities, ongoing challenges, and research opportunities. Ann N Y Acad Sci. 2010;1186:69–101. doi: 10.1111/j.1749-6632.2009.05339.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Knox SS, Jacobs DR, Chesney MA, Raczynski J, McCreath H. Psychosocial factors and plasma lipids in black and white young adults: the Coronary Artery Risk Development in Young Adults Study data. Psychosom Med. 1996;58:365–73. doi: 10.1097/00006842-199607000-00009. [DOI] [PubMed] [Google Scholar]
- 28.Williams DR. The health of men: structured inequalities and opportunities. Am J Public Health. 2003;93:724–31. doi: 10.2105/ajph.93.5.724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Muzet A. Environmental noise, sleep and health. Sleep Med Rev. 2007;11:135–42. doi: 10.1016/j.smrv.2006.09.001. [DOI] [PubMed] [Google Scholar]
- 30.Pirrera S, De Valck E, Cluydts R. Nocturnal road traffic noise: a review on its assessment and consequences on sleep and health. Environ Int. 2010;36:492–8. doi: 10.1016/j.envint.2010.03.007. [DOI] [PubMed] [Google Scholar]
- 31.Nivison ME, Endresen IM. An analysis of relationships among environmental noise, annoyance and sensitivity to noise, and the consequences for health and sleep. J Behav Med. 1993;16:257–76. doi: 10.1007/BF00844759. [DOI] [PubMed] [Google Scholar]
- 32.Zanobetti A, Redline S, Schwartz J, et al. Associations of PM10 with sleep and sleep-disordered breathing in adults from seven U.S. urban areas. Am J Respir Crit Care Med. 2010;182:819–25. doi: 10.1164/rccm.200912-1797OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hale L, Hill TD, Burdette AM. Does sleep quality mediate the association between neighborhood disorder and self-rated physical health? Prev Med. 2010;51:275–8. doi: 10.1016/j.ypmed.2010.06.017. [DOI] [PubMed] [Google Scholar]
- 34.Hale L, Hill TD, Friedman E, et al. Perceived neighborhood quality, sleep quality, and health status: evidence from the Survey of the Health of Wisconsin. Soc Sci Med. 2013;79:16–22. doi: 10.1016/j.socscimed.2012.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Johnson SL, Solomon BS, Shields WC, McDonald EM, McKenzie LB, Gielen AC. Neighborhood violence and its association with mothers' health: assessing the relative importance of perceived safety and exposure to violence. J Urban Health. 2009;86:538–50. doi: 10.1007/s11524-009-9345-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gamaldo AA, McNeely JM, Shah MT, Evans MK, Zonderman AB. Racial differences in self-reports of short sleep duration in an urban-dwelling environment. J Gerontol B Psychol Sci Soc Sci. 2015;70:568–75. doi: 10.1093/geronb/gbt117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Desantis AS, Diez Roux AV, Moore K, Baron KG, Mujahid MS, Nieto FJ. Associations of neighborhood characteristics with sleep timing and quality: the multi-ethnic study of atherosclerosis. Sleep. 2013;36:1543–51. doi: 10.5665/sleep.3054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Spilsbury JC, Storfer-Isser A, Kirchner HL, et al. Neighborhood disadvantage as a risk factor for pediatric obstructive sleep apnea. J Pediatr. 2006;149:342–7. doi: 10.1016/j.jpeds.2006.04.061. [DOI] [PubMed] [Google Scholar]
- 39.Brouillette RT, Horwood L, Constantin E, Brown K, Ross NA. Childhood sleep apnea and neighborhood disadvantage. J Pediatr. 2011;158:789–95.e1. doi: 10.1016/j.jpeds.2010.10.036. [DOI] [PubMed] [Google Scholar]
- 40.Singh GK, Kenney MK. Rising prevalence and neighborhood, social, and behavioral determinants of sleep problems in US children and adolescents, 2003-2012. Sleep Disord. 2013;2013:394320. doi: 10.1155/2013/394320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hill TD, Burdette AM, Hale L. Neighborhood disorder, sleep quality, and psychological distress: testing a model of structural amplification. Heal Place. 2009;15:1006–13. doi: 10.1016/j.healthplace.2009.04.001. [DOI] [PubMed] [Google Scholar]
- 42.Taylor HA, Wilson JG, Jones DW, et al. Toward resolution of cardiovascular health disparities in African Americans: design and methods of the Jackson Heart Study. Ethn Dis. 2005;15 S6–S4–17. [PubMed] [Google Scholar]
- 43.Gebreab SY, Diez-Roux AV, Hickson D, et al. The contribution of stress to the social patterning of clinical and subclinical CVD risk factors in African Americans: the Jackson Heart Study. Soc Sci Med. 2012;75:1697–707. doi: 10.1016/j.socscimed.2012.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Wyatt SB, Diekelmann N, Henderson F, et al. A community-driven model of research participation: the Jackson Heart Study participant recruitment and retention study. Ethn Dis. 2003;13:438–55. [PubMed] [Google Scholar]
- 45.Fuqua SR, Wyatt SB, Andrew ME, et al. Recruiting African-American research participation in the Jackson Heart Study: methods, response rates, and sample description. Ethn Dis. 2005;15 S6–S18–29. [PubMed] [Google Scholar]
- 46.Hickson DA, Waller LA, Gebreab SY, et al. Geographic representation of the jackson heart study cohort to the African-American population in Jackson, Mississippi. Am J Epidemiol. 2011;173:110–7. doi: 10.1093/aje/kwq317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Grandner MA, Patel NP, Gehrman PR, Perlis ML, Pack AI. Problems associated with short sleep: bridging the gap between laboratory and epidemiological studies. Sleep Med Rev. 2010;14:239–47. doi: 10.1016/j.smrv.2009.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Grandner MA, Drummond SP. Who are the long sleepers? Towards an understanding of the mortality relationship. Sleep Med Rev. 2007;11:341–60. doi: 10.1016/j.smrv.2007.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mujahid MS, Diez Roux A V, Morenoff JD, Raghunathan T. Assessing the measurement properties of neighborhood scales: from psychometrics to ecometrics. Am J Epidemiol. 2007;165:858–67. doi: 10.1093/aje/kwm040. [DOI] [PubMed] [Google Scholar]
- 50.Mujahid MS, Diez Roux AV, Morenoff JD, et al. Neighborhood characteristics and hypertension. Epidemiology. 2008;19:590–8. doi: 10.1097/EDE.0b013e3181772cb2. [DOI] [PubMed] [Google Scholar]
- 51.Diez Roux AV, Merkin SS, Arnett D, et al. Neighborhood of residence and incidence of coronary heart disease. N Engl J Med. 2001;345:99–106. doi: 10.1056/NEJM200107123450205. [DOI] [PubMed] [Google Scholar]
- 52.Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–52. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 53.American Diabetes Association. Screening for type 2 diabetes. Diabetes Care. 2004;27(suppl 1):s11–4. doi: 10.2337/diacare.27.2007.s11. [DOI] [PubMed] [Google Scholar]
- 54.Baecke JA, Burema J, Frijters JE. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982;36:936–42. doi: 10.1093/ajcn/36.5.936. [DOI] [PubMed] [Google Scholar]
- 55.Dubbert PM, Carithers T, Ainsworth BE, Taylor HA, Wilson G, Wyatt SB. Physical activity assessment methods in the Jackson Heart Study. Ethn Dis. 2005;15:S56–61. [PubMed] [Google Scholar]
- 56.Zimmerman M, Posternak MA, Chelminski I. Using a self-report depression scale to identify remission in depressed outpatients. Am J Psychiatry. 2004;161:1911–3. doi: 10.1176/ajp.161.10.1911. [DOI] [PubMed] [Google Scholar]
- 57.Leal C, Bean K, Thomas F, Chaix B. Multicollinearity in associations between multiple environmental features and body weight and abdominal fat: using matching techniques to assess whether the associations are separable. Am J Epidemiol. 2012;175:1152–62. doi: 10.1093/aje/kwr434. [DOI] [PubMed] [Google Scholar]
- 58.Kavanagh AM, Bentley R, Turrell G, Broom DH, Subramanian SV. Does gender modify associations between self rated health and the social and economic characteristics of local environments? J Epidemiol Community Health. 2006;60:490–5. doi: 10.1136/jech.2005.043562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Wardle J, Waller J, Jarvis MJ. Sex differences in the association of socioeconomic status with obesity. Am J Public Health. 2002;92:1299–304. doi: 10.2105/ajph.92.8.1299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Krueger PM, Friedman EM. Sleep duration in the United States: a cross-sectional population-based study. Am J Epidemiol. 2009;169:1052–63. doi: 10.1093/aje/kwp023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Moore PJ, Adler NE, Williams DR, Jackson JS. Socioeconomic status and health: the role of sleep. Psychosom Med. 2002;64:337–44. doi: 10.1097/00006842-200203000-00018. [DOI] [PubMed] [Google Scholar]
- 62.Hall M, Bromberger J, Matthews K. Socioeconomic status as a correlate of sleep in African-American and Caucasian women. Ann N Y Acad Sci. 1999;896:427–30. doi: 10.1111/j.1749-6632.1999.tb08161.x. [DOI] [PubMed] [Google Scholar]
- 63.Kimmel J, Smith Conway K. Who moonlights and why? Evidence from the SIPP. Ind Relat. 2001;40:89–120. [Google Scholar]
- 64.Sekine M, Chandola T, Martikainen P, Marmot M, Kagamimori S. Work and family characteristics as determinants of socioeconomic and sex inequalities in sleep: the Japanese Civil Servants Study. Sleep. 2006;29:206–16. doi: 10.1093/sleep/29.2.206. [DOI] [PubMed] [Google Scholar]
- 65.Friedman EM, Love GD, Rosenkranz MA, et al. Socioeconomic status predicts objective and subjective sleep quality in aging women. Psychosom Med. 2007;69:682–91. doi: 10.1097/PSY.0b013e31814ceada. [DOI] [PubMed] [Google Scholar]
- 66.Henderson C, Diez Roux AV, Jacobs DR, Kiefe CI, West D, Williams DR. Neighbourhood characteristics, individual level socioeconomic factors, and depressive symptoms in young adults: the CARDIA study. J Epidemiol Community Health. 2005;59:322–8. doi: 10.1136/jech.2003.018846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Patel SR, Malhotra A, Gottlieb DJ, White DP, Hu FB. Correlates of long sleep duration. Sleep. 2006;29:881–9. doi: 10.1093/sleep/29.7.881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch Intern Med. 2005;165:863–7. doi: 10.1001/archinte.165.8.863. [DOI] [PubMed] [Google Scholar]
- 69.Gildner TE, Liebert MA, Kowal P, Chatterji S, Snodgrass JJ. Associations between sleep duration, sleep quality, and cognitive test performance among older adults from six middle income countries: Results from the Study on Global Ageing and Adult Health (SAGE) J Clin Sleep Med. 2014;10:613–21. doi: 10.5664/jcsm.3782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Johnson DA, Brown DL, Morgenstern LB, Meurer WJ, Lisabeth LD. The association of neighborhood characteristics with sleep duration and daytime sleepiness. Sleep Health. 2015;1:148–55. doi: 10.1016/j.sleh.2015.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Johnson DA, Lisabeth L, Lewis TT, et al. The contribution of psychosocial stressors to sleep among African Americans in the Jackson Heart Study. Sleep. 2016;39:1411–9. doi: 10.5665/sleep.5974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Hill TD, Trinh HN, Wen M, Hale L. Perceived neighborhood safety and sleep quality: a global analysis of six countries. Sleep Med. 2016;18:56–60. doi: 10.1016/j.sleep.2014.12.003. [DOI] [PubMed] [Google Scholar]
- 73.Reed E, Silverman JG, Welles SL, Santana MC, Missmer SA, Raj A. Associations between perceptions and involvement in neighborhood violence and intimate partner violence perpetration among urban, African American men. J Community Health. 2009;34:328–35. doi: 10.1007/s10900-009-9161-9. [DOI] [PubMed] [Google Scholar]
- 74.Baker FC, Maloney S, Driver HS. A comparison of subjective estimates of sleep with objective polysomnographic data in healthy men and women. J Psychosom Res. 1999;47:335–41. doi: 10.1016/s0022-3999(99)00017-3. [DOI] [PubMed] [Google Scholar]
- 75.Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ. Sleep duration: how well do self-reports reflect objective measures? The CARDIA Sleep Study. Epidemiology. 2008;19:838–45. doi: 10.1097/EDE.0b013e318187a7b0. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.