

In treating superior laryngeal neuralgia (SLN), superior laryngeal nerve blocks (SLNBs) can provide immediate relief of persistent pain. Although SLNB was effective, the procedure can increase the risks due to the proximity to the carotid artery, external vein, and other vessels. To avoid complications such as advertent intravascular injection, local anesthetic toxicity from intravascular absorption, and intratracheal injection, we successfully blocked the superior laryngeal nerve under ultrasound guidance in three patients suffering from SLN. The written informed consent before treatment was obtained for each patient participating in this study.
A 58-year-old male was admitted to our hospital; he had a complaint of a fish bone that had stuck to his throat 6 months ago, and the bone was immediately removed (case 1). Subsequently, he experienced paroxysmal burning and stabbing pain in his left throat. Pain was associated with deep inspiration and coughing. Tenderness over the left thyrohyoid membrane was elicited by light pressure. Neurological examination was negative. The left SLNBs under ultrasound guidance using 3 ml of 2% lidocaine were done for four times, which was completed for every 2 days. The patient experienced no pain when we followed up 6 months following the procedures.
A 70-year-old female who developed left-side SLN for 2 years was admitted to our hospital (case 2). She had had a cough for a week just before the onset of the neuralgia. She experienced paroxysmal stabbing pain in the left side of the throat, triggered by swallowing and aspiration. There was tenderness to pressure over the left thyrohyoid membrane. Neurological examination was negative, and 10 trials of SLNB were done. Although the paroxysms occurred once a year for a few months after the last block therapy, she was able to deal with the pain with carbamazepine alone.
A 57-year-old male with complaints of right-side throat pain for the previous 5 months was admitted to our hospital (case 3). He had a history of severe smoking for about 20 years. The paroxysmal stabbing pain occurred almost every day. Neurological examination was negative. After 10 trials of SLNB, pain was alleviated. He remained asymptomatic for about 1 year after the last SLNB.
A portable ultrasound machine, Venue 50, (GE Healthcare, Chalfont St. Giles, UK) was brought to the operating room, with the patient lying in the supine position with head turned away from the affected side and a pillow placed under the patient's neck. After preparation of the skin with antiseptic solution, ultrasound examination is performed using a high-resolution linear array transducer. The transducer is applied transversely to the middle aspect of the neck to obtain a short axis view of the thyrohyoid membrane. One can easily identify the thyroid cartilage and the common carotid artery. The superior laryngeal nerve is usually found medial to the artery between the hyoid bone and thyroid cartilage, and a block needle is inserted in the plane of the ultrasound beam in a medial to lateral orientation. It is often easy to visualize the needle. The needle was inserted with 35° to the skin and the depth was approximately 2 cm. When the needle located medial to the common carotid artery, with no blood or air of the aspirated, the test dose of 2 ml of 2% lidocaine was injected [Figure 1]. The procedure is completed for every 2 days until the pain disappeared.
Figure 1.
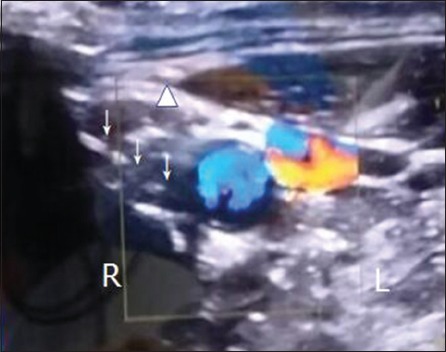
Transverse sonographic view of the patient's neck at the level of the thyrohyoid membrane. An in-plane method was used to block the superior laryngeal nerve. Arrow indicates the entry of the needle from the 10 o’clock direction. Triangle indicates the thyrohyoid membrane, blue indicates the carotid artery, and red indicates the external carotid vein. L: Left, R: Right.
The superior laryngeal nerve arises from the vagus nerve. It runs inferiorly and anteriorly behind the carotid artery to pass the lateral extent of the hyoid bone.[1] It divides into internal and external branches. The internal branch passes immediately inferior to the greater horn of the hyoid bone and approaches the thyrohyoid membrane accompanied by the superior laryngeal artery, a branch of the superior thyroid artery. The superior laryngeal nerve is so located that any regional inflammation or further local trauma,[2] aggravated by normal laryngeal movements, can produce localized neuritis at the thyrohyoid membrane and cause the throat pain. Aydin et al.[3] described a case of SLN after acute laryngitis and treatment with a single injection of a local anesthetic. The patient received a single nerve block near the right hypothyroid membrane and the symptoms decreased dramatically in a few minutes. He had no pain for 1 year following the procedure. Neuropathic pain is derived from abnormal afferent inputs caused by axonal damage, myelin disruption, and inflammatory processes. Local anesthetics can interrupt or alleviate pain and have been shown to suppress ectopic neural discharges from nerve fibers. It was posited that SLNB may be useful in the diagnosis and treatment of SLN.[4]
Ultrasound has been used to image the human body for over half a century. The images can be acquired in “real time,” thus providing instantaneous visual guidance for many interventional procedures including those for regional anesthesia and pain management.[5]
In these three cases, the use of ultrasound made it possible to perform SLNB in patients suffering from SLN. All of the three patients recovered from SLB without any complications. These cases illustrate a potential clinical application for ultrasound assistance in pain management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Qiang Shi
REFERENCES
- 1.Furlan JC. Anatomical study applied to anesthetic block technique of the superior laryngeal nerve. Acta Anaesthesiol Scand. 2002;46:199–202. doi: 10.1034/j.1399-6576.2002.460214.x. doi: 10.1034/j.1399-6576.2002.460214.x. [DOI] [PubMed] [Google Scholar]
- 2.Bruyn GW. Superior laryngeal neuralgia. Cephalalgia. 1983;3:235–40. doi: 10.1046/j.1468-2982.1983.0304235.x. doi: 10.1046/j.1468-2982.1983.0304235.x. [DOI] [PubMed] [Google Scholar]
- 3.Aydin O, Ozturk M, Anik Y. Superior laryngeal neuralgia after acute laryngitis and treatment with a single injection of a local anesthetic. Arch Otolaryngol Head Neck Surg. 2007;133:934–5. doi: 10.1001/archotol.133.9.934. doi: 10.1001/archotol.133.9.934. [DOI] [PubMed] [Google Scholar]
- 4.Takahashi Sato K, Suzuki M, Izuha A, Hayashi S, Isosu T, Murakawa M. Two cases of idiopathic superior laryngeal neuralgia treated by superior laryngeal nerve block with a high concentration of lidocaine. J Clin Anesth. 2007;19:237–8. doi: 10.1016/j.jclinane.2006.09.003. doi: 10.1016/j.jclinane.2006.09.003. [DOI] [PubMed] [Google Scholar]
- 5.Singh M, Chin KJ, Chan VW, Wong DT, Prasad GA, Yu E. Use of sonography for airway assessment: An observational study. J Ultrasound Med. 2010;29:79–85. doi: 10.7863/jum.2010.29.1.79. [DOI] [PubMed] [Google Scholar]