

Abstract
Context:
Ameloblastoma is the second most common odontogenic tumor after odontoma which occurs exclusively in the jaws and very rarely in the sinonasal cavities.
Aims:
The aim of the study was to determine the demographic and histopathological variations of ameloblastoma in Eastern Indian population by retrospectively comparing and evaluating diagnosed cases of ameloblastoma using different parameters.
Materials and Methods:
Histopathologically diagnosed cases of ameloblastoma retrieved from past records of the Department of Oral Pathology were selected for the study. Totally, 148 cases were isolated from record of previous 7 years. The patients were divided according to (a) gender, (b) age group, (c) site of the lesion and (d) histopathological types. The findings of this study were compared with those available in literature.
Statistical Analysis Used:
This is a retrospective study, mean and standard deviation was calculated.
Results:
Among 148 patients, 88 (59.45%) were male and 60 (40.55%) were female. A maximum number of cases (101 of 148) of ameloblastoma were found in the second to fourth decades of life. Mandiblular posterior region was commonly involved (48.6%). Solid/multicystic variety was found in 63.1% followed by unicystic with 21.5%. We found one case each of extraosseous and desmoplastic ameloblastoma. It was difficult for panel of experienced oral pathologists to pinpoint the exact type in 15 (10%) cases, this was due to mixture of follicular and plexiform variety with equal presence of both types of architecture, without predominance of any variety in particular.
Conclusions:
These data may serve as baseline information on occurrence of various histopathological types of ameloblastoma in Eastern Indian population and helps comparing it with other similar studies conducted in different geographic population.
Key Words: Ameloblastoma, demography, histological types
INTRODUCTION
The term odontogenic tumor describes variety of lesions varying from from hamartomatous or benign tissue proliferation to malignant neoplasm with metastatic potential.[1] Odontogenic tumors are lesions derived from epithelial, ectomesenchymal and/or mesenchymal elements that still are, or have been, part of the tooth forming apparatus. These tumors are found exclusively within maxillofacial skeleton (intraosseous/centrally located) or in the soft tissue (gingiva) overlying tooth-bearing areas or alveolar mucosa in edentulous regions (extraosseous or peripherally located). Etiology of benign and malignant odontogenic tumors is unknown. A majority of odontogenic tumors seem to arise de novo, without an apparent causative factor.[2]
Ameloblastoma is one of the most commonly occurring odontogenic tumors of jaws. It represents one percent of all tumors of head and neck region.[3] Robinson defined ameloblastoma as “unicystic, nonfunctional, intermittent in growth, anatomically benign and clinically persistent tumor.” It may arise from residual epithelium of tooth germ, odontogenic cysts or enamel organ.[3] The theory of an odontogenic origin for ameloblastoma is supported by the occurrence of tumor in the tooth-bearing areas.[4] WHO (2005) classified ameloblastoma into (a) solid/multicystic, (b) unicystic, (c) extraosseous/peripheral and (d) desmoplastic. There are two basic histopathologic patterns in solid/multicystic ameloblastoma: (1) follicular and (2) plexiform. Other microscopic patterns of ameloblastoma include acanthomatous, basal cell-like and granular cell. These patterns can be uniform or mixed. In different parts of the world, the distribution of ameloblastoma varies to a certain extent.[5] The study was aimed to find such differences in distribution using different demographic parameters of this tumor in Eastern Indian population and to compare the findings of this study with those available in similar literature.
SUBJECTS AND METHODS
A total of 148 histopathologically diagnosed cases of ameloblastoma were retrieved for detailed analysis from the Department of Oral Pathology after obtaining the institutional ethical committee clearance. The data of the patients reported between April 2007 and April 2014 were included. Patients' details were analyzed considering gender, age-group, site of lesion and histological types of ameloblastoma. Multiple sections were prepared in 15 cases in which determination of the exact type of ameloblastoma was difficult. Only hematoxylin and eosin stained sections were used to diagnose all the cases in this study. Radiographic findings available in records were considered to determine site and extent of the lesion.
RESULTS
A total of 148 cases of ameloblastoma of the oral cavity and the jaws were considered from the Department of Oral Pathology.
Gender distribution
Of the 148 cases, 88 patients were males and 60 were females indicating a male: female ratio of 1.5:1 [Table 1].
Table 1.
Gender distribution

Age-group distribution
Age-group distribution for 148 cases of ameloblastoma is summarized in Table 2. The age of occurrence for ameloblastoma of both jaws ranged from 6 to 75 years with a mean age of 32.75 years.
Table 2.
Age-group distribution

Site of the lesion
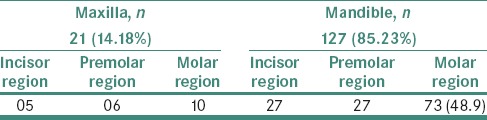
The distribution of ameloblastoma in different anatomical regions is presented in Table 3. Of 148 cases, 21 (14%) cases of ameloblastoma crossed the midline.
Table 3.
Anatomical distribution
Histopathological type
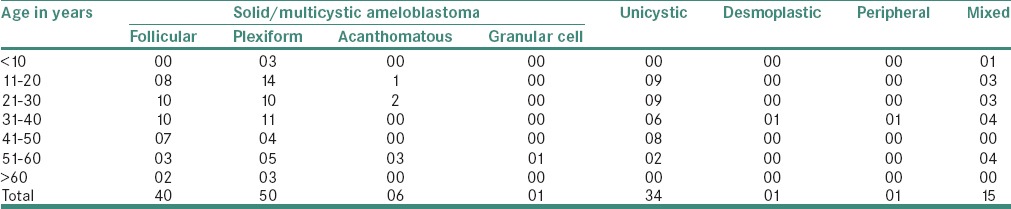
Among histopathological types, solid/multicystic was most common with 97 (65.1%) cases. Thirty-four (22.97) cases were of unicystic variety. One case each were of extraosseous and desmoplastic type. Among solid/multicystic, plexiform pattern was most frequent with 50 (33.78%) cases followed by follicular with 40 (27.02%) cases. A total of 15 (10%) cases were showing almost equal distribution of plexiform and follicular patterns. Three deeper serial sections from each block were prepared in these 15 (10%) cases. However, it was difficult to specify the exact histopathological type by panel of experienced oral pathologist in these cases due to divergence of opinions. These 15 cases were not included in the solid/multicystic type and grouped them separately as mixed variety of ameloblastoma [Table 4].
Table 4.
Histopathological subtypes
DISCUSSION
Ameloblastoma has been known for about 190 years. During different periods, it has been known by different terms. Gorlin identifies Cusack as the first person to identify “Ameloblastoma” in 1827. Falkson gave a detailed description in 1879. Malassez (1885) introduced the term “Adamantine epithelioma” while Derjinsky (1890) introduced the term “Adamantinoma”. Ivy and Churchill, in 1930, encouraged the use of the term “Ameloblastoma” which is the preferred terminology till date.[6]
In the present study, 59.45% of patients were male and 40.55% of patients were females. This data was comparable to Reichart et al. study,[7] in which 53% were males and 47% were females. These findings in the present study were similar to previous studies of Krishnapillai and Angadi, Sriram and Shetty in Indian population.[8,9] The average age of the patient at the time of initial diagnosis was 32.5 years, which is similar to that in the Chinese population in whom tumors were presented at the mean age of 32.4 years.[10] Reichart et al. in their biological profile of 3,677 cases found the average age of 35.9 years at the time of initial diagnosis.[7] This finding presents similarity to 30.2 and 32.3 years in studies carried out by Krishnapillai and Angadi P, Sriram and Shetty, respectively. Overall, it may be said that it is a disease involving middle age population in most cases.[8,9]
The mandible was affected in 126 cases (85.13%) and the maxilla in 22 cases (14.87%), with ratio of 6:1. Mandibular posterior region was involved in almost half of the mandibular lesions. In our review, solid/multicystic ameloblastoma was the most frequently encountered histopathological type (66.21%) followed by unicystic (22.90%) which is in contrast to study conducted in Latin American population where unicystic ameloblastoma was the most common (63.20%) type.[11] One case each of desmoplastic and peripheral ameloblastoma was found.
Among solid/multicystic, plexiform pattern was most common with 33.8% of cases followed by follicular comprising of 27.7% of cases. Histopathologically, in different studies, follicular pattern has been reported to be the most common subtype.[8] Remaining 10% cases were mixture of subtypes of ameloblastoma, especially plexiform and follicular pattern in equal proportion. Similar studies on ameloblastoma mentioned cases of mixed variety of ameloblastoma varying between 3.3% and 20%.[12,13]
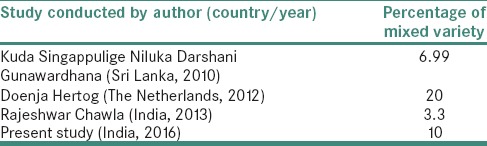
A study conducted in Sri Lankan (2010) population on clinicopathological comparison of ameloblastoma showed 6.99% of cases with mixed patterns of ameloblastoma.[14] Hertog et al. in their study in the Netherland population, over the period of 40 years, found almost 20% of cases of ameloblastoma with mixed patterns microscopically. Intraobserver variation was also recorded in their study which was mainly found in typing follicular and plexiform type versus mixed type ameloblastoma.[13] One more study including Indian population by Chawla et al. showed only 3.3% of cases with mixed patterns of ameloblastoma [Table 5]. In this study, we have provided the overall number of cases with mixed pattern and also compared these data with previous studies with finding of similar pattern. However, it should be noted that various classifications currently followed do not have a separate mention of mixed pattern. In addition, a single study aimed at the occurrence and detailed description of histopathological features of mixed variety is lacking. There is no mention about the mixed pattern of ameloblastoma even in the WHO (2005) classification of odontogenic tumors.
Table 5.
Comparison of mixed variety n different studies
CONCLUSIONS
This study provides a broad analysis of ameloblastomas in the Eastern Indian population using different parameters. Since variants of ameloblastoma differ in biologic behavior, the data collected in this study provides clinical and histopathological information which is of significance to the Oral Pathologist and the Clinician. Moreover, inclusion of details on mixed variety of ameloblastoma in various studies should be encouraged to throw light on overall rate of occurrence of variety of the tumor.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Philipsen HP, Reichart PA. Revision of the 1992-edition of the WHO histological typing of odontogenic tumours. A suggestion. J Oral Pathol Med. 2002;31:253–8. doi: 10.1034/j.1600-0714.2002.310501.x. [DOI] [PubMed] [Google Scholar]
- 2.Philipsen HP, Reichart PA, Slootweg PJ, Slater LJ. World Health Organization classification of tumours pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005. Neoplasms and tumour-like lesions arising from the odontogenic apparatus and maxillofacial skeleton: Introduction; pp. 285–6. [Google Scholar]
- 3.Gümgüm S, Hosgören B. Clinical and radiologic behaviour of ameloblastoma in 4 cases. J Can Dent Assoc. 2005;71:481–4. [PubMed] [Google Scholar]
- 4.Adebiyi KE, Ugboko VI, Omoniyi-Esan GO, Ndukwe KC, Oginni FO. Clinicopathological analysis of histological variants of ameloblastoma in a suburban Nigerian population. Head Face Med. 2006;2:42. doi: 10.1186/1746-160X-2-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Larsson A, Almerén H. Ameloblastoma of the jaws. An analysis of a consecutive series of all cases reported to the Swedish Cancer Registry during 1958-1971. Acta Pathol Microbiol Scand A. 1978;86A:337–49. [PubMed] [Google Scholar]
- 6.Angadi PV. Head and neck: Odontogenic tumor: Ameloblastoma. Atlas Genet Cytogenet Oncol Haematol. 2011;15:223–9. [Google Scholar]
- 7.Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: Biological profile of 3677 cases. Oral Oncol. 1995;31B:86–99. doi: 10.1016/0964-1955(94)00037-5. [DOI] [PubMed] [Google Scholar]
- 8.Krishnapillai R, Angadi PV. A clinical, radiographic, and histologic review of 73 cases of ameloblastoma in an Indian population. Quintessence Int. 2010;41:e90–100. [PubMed] [Google Scholar]
- 9.Sriram G, Shetty RP. Odontogenic tumors: A study of 250 cases in an Indian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e14–21. doi: 10.1016/j.tripleo.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 10.Wu PC, Chan KW. A survey of tumours of the jawbones in Hong Kong Chinese: 1963-1982. Br J Oral Maxillofac Surg. 1985;23:92–102. doi: 10.1016/0266-4356(85)90058-0. [DOI] [PubMed] [Google Scholar]
- 11.Ledesma-Montes C, Mosqueda-Taylor A, Carlos-Bregni R, de León ER, Palma-Guzmán JM, Páez-Valencia C, et al. Ameloblastomas: A regional Latin-American multicentric study. Oral Dis. 2007;13:303–7. doi: 10.1111/j.1601-0825.2006.01284.x. [DOI] [PubMed] [Google Scholar]
- 12.Chawla R, Ramalingam K, Sarkar A, Muddiah S. Ninety-one cases of ameloblastoma in an Indian population: A comprehensive review. J Nat Sci Biol Med. 2013;4:310–5. doi: 10.4103/0976-9668.116984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hertog D, Bloemena E, Aartman IH, van-der-Waal I. Histopathology of ameloblastoma of the jaws; some critical observations based on a 40 years single institution experience. Med Oral Patol Oral Cir Bucal. 2012;17:e76–82. doi: 10.4317/medoral.18006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Darshani Gunawardhana KS, Jayasooriya PR, Rambukewela IK, Tilakaratne WM. A clinico-pathological comparison between mandibular and maxillary ameloblastomas in Sri Lanka. J Oral Pathol Med. 2010;39:236–41. doi: 10.1111/j.1600-0714.2009.00850.x. [DOI] [PubMed] [Google Scholar]