

Abstract
AIM
To validate the culturally-adapted Persian Functional Rating Index (PFRI) for assessing neck pain (NP) in athletes.
METHODS
In this cross-sectional study, 100 athletes with NP and 50 healthy athletes participated and responded to the PFRI. Fifty athletes with NP completed the PFRI for at least 7 d later to establish test-retest reliability.
RESULTS
The athletes with NP responded to all items, indicating excellent clinical utility. No floor and ceiling effects were found, indicating content validity and responsiveness. The PFRI revealed capability to discriminate between the athletes with NP and healthy athletes. The PFRI demonstrated strong correlation with the Numerical Rating Scale (Spearman’s rho = 0.94), and the Persian Neck Disability Index (Pearson r = 0.995), supporting criterion and construct validity. Internal consistency reliability was high (Cronbach’s α coefficient: 0.97). The test-retest reliability was excellent (ICCagreement = 0.96). The absolute reliability values of standard error of measurement and smallest detectable change were 3.2 and 8.84, respectively. An exploratory factor analysis yielded one factor explaining 78.03% of the total variance.
CONCLUSION
The PFRI is a valid and reliable measure of functional status in athletes with NP.
Keywords: Athletes, Neck pain, Functional rating index, Reliability, Validity
Core tip: Patient-reported outcomes are widely used to evaluate the functional effectiveness of treatments in clinical investigations. There has been a lack of patient-reported outcome measure for athletes with neck pain (NP). This study assessed the psychometric properties of the culturally-adapted Persian Functional Rating Index in a group of athletes with NP and demonstrated excellent validity and reliability.
INTRODUCTION
Neck pain (NP) is a common musculoskeletal complaint in athletes. The lifetime incidence of NP has been estimated at 47.6%, with approximately 64% being sports related[1]. An epidemiological study found a relatively higher rate of NP in cycling athletes[2]. The NP in athletes may result from sprains, strains, and soft tissue contusions resulting in various problems such as deficits in mobility, strength, endurance, and postural stability[3-6]. In order to help the athletes with NP return quickly to their sporting function, it is important to accurately assess their symptoms and function using valid and reliable tools.
There are several disease-specific questionnaires developed to assess the functional limitations in people with spinal disorders including neck pain (e.g., neck disability index, neck pain and disability scale). Any outcome tool should be validated among different populations before using in the clinical assessments. The validity of the questionnaires to measure neck related pain and disability is not established among athletes with NP. Currently, there is no validated test developed specifically for assessing NP in athletes.
The Functional Rating Index (FRI) is a patient-reported questionnaire developed to evaluate the patients’ perspectives on their pain and functional status in patients with low back pain (LBP) as well as NP[7]. The Persian FRI (PFRI) is validated in the general population with LBP[8] and NP[9], and it was recently validated for athletes with LBP[10]. The present study aims to validate the PFRI in athletes with NP. The psychometric properties of floor or ceiling effects, discriminant validity, concurrent criterion validity, construct validity, internal consistency reliability, test-retest reliability, standard error of measurement (SEM), smallest detectable change (SDC), and factor structure were evaluated.
MATERIALS AND METHODS
The protocol of this cross-sectional study was approved by the review board, School of Rehabilitation, Tehran University of Medical Sciences (TUMS). The study was performed after approval by the TUMS Ethics Committee, and all subjects gave their written informed consent for taking part in the study.
Participants
Adult athletes age ≥ 18 years with NP, participating in sport activities for at least 2 h, 3 d/wk, and be able to read and write Persian were recruited from Tehran, Iran sport clubs and included in the study. Athletes were excluded if they had osteoporosis, spinal fracture, previous spinal surgery, or rheumatologic diseases. The sample size for this study was based on the recommendation provided in the guideline; thus, 100 athletes with NP were included in the study[11].
Procedure
We followed the procedure used for validation of the FRI in athletes with LBP[10]. Eligible athletes were sampled from the Tehran sport clubs, Iran. The study aim and procedure were first thoroughly described to each eligible athlete. Then, after an informed consent form was read and signed by each athlete, demographic data including age, education, NP duration, and sports activities were recorded. Each eligible athlete was asked to fill out the PFRI, validated Persian Neck Disability Index (NDI)[12], and the Numerical Rating Scale (NRS)[13]. Fifty athletes with NP refilled out the PFRI at least 7 d later to evaluate the test-retest reliability. Fifty healthy athletes with no neck pain filled out the PFRI to assess discriminant validity. The NDI and the NRS were filled out to assess respect construct validity and concurrent criterion validity. High correlation was expected between the PFRI and NDI for construct validity.
Instruments
FRI: The FRI is a reliable and valid instrument that contains 10 items measuring both pain and function from 0 (no pain/full function) to 4 (worst possible pain/unable to perform function). The formula (total score/40) × 100% was used to calculate the disability score ranging from 0% (no disability) to 100% (severe disability)[7,14]. The culturally adapted and validated Persian FRI was used in this study[8-10].
NDI: The instrument used to evaluate the construct validity was the reliable and valid NDI[15]. The NDI contains 10 items with each item rated from 0 (no activity limitation) to 5 (major activity limitation). The NDI total score is calculated as a percentage, with higher scores meaning greater disability. In this study, the culturally adapted Persian NDI was used[12].
NRS: The NRS was used to assess concurrent criterion validity. With the NRS, the athletes with NP were asked to score their pain intensity between 0 (no pain) and 10 (worst possible pain)[13,16].
Statistical analysis
The floor and ceiling effects were analyzed by calculation of percentage of the lowest (0%) and the highest (100%) scores for the total PFRI. Discriminant validity was assessed by comparing the PFRI total scores of the athletes with NP with scores of the healthy athletes using the independent t test. The construct validity was analyzed by examining the correlation between the PFRI and the NDI using Pearson correlation test with levels of 0.6 ≥ [7]. The Spearman rank order correlation was used to assess concurrent criterion validity by correlating the PFRI total scores to the NRS with at least 0.7 as acceptable. The Cronbach’s α was applied to analyze the internal consistency reliability with a level of 0.7 or higher as satisfactory[11]. The intraclass correlation coefficient agreement (ICCagreement) (two-way random effects model, absolute agreement, and single measure) was used for the test-retest reliability analysis with a level of at least 0.70 as acceptable. The absolute reliability measures of the standard SEM and the SDC were estimated using the formulas σ√1-ICC and 1.96 × SEM × √2, respectively. A principal component analysis (PCA) with varimax rotation (VR) was used to analyze the factor structure of the PFRI. The SPSS software, V17 (SPSS, Inc, Chicago, IL) was used for the statistical analyses.
RESULTS
Overall, this study recruited 150 athletes. One hundred athletes with NP (60 male/40 female; mean age ± SD 30.8 ± 6.7 years; education 15.0 ± 2.2 years; NP duration 3.72 ± 1.74 mo) and 50 healthy athletes (27 male/23 female; mean age 31.5 ± 7.4 years; education 15.0 ± 2.4 years) participated in the study. Of the 100 recruited athletes with NP, 50 athletes completed the PFRI again after at least 7 d (range: 7.0-32.0 d) to establish test-retest reliability.
The sports activities of athletes in this sample of athletes (n = 150) included bodybuilding (n = 46, 30.7%), aerobics (n = 27, 18.0%), swimming (n = 16, 10.7%), karate (n = 17, 11.3%), taekwondo (n = 13, 8.7%), volleyball (n = 10, 6.7%), soccer (n = 9, 6.0%), yoga (n = 6, 4.0%), and badminton (n = 6, 4.0%).
Floor and ceiling effects
The athletes with NP responded to all items, and no missing data were detected. No floor or ceiling effect was observed for PFRI scores (range: 10.00-92.50). No athletes with NP scored the highest or lowest possible score on the PFRI. Table 1 shows the clinical data for the athletes with NP.
Table 1.
Summary of clinical data in athletes with neck pain (n = 100)
| Outcome measures | Mean | SD | Range |
|
| Minimum | Maximum | |||
| PFRI | 30.85 | 15.94 | 10.00 | 92.500 |
| PNDI | 30.22 | 15.93 | 8.00 | 88.00 |
| NRS | Median (IQR) 2 (2-3) | |||
PFRI: Persian functional rating index; PNDI: Persian neck disability index; NRS: Numerical rating scale; IQR: Interquartile range.
Validity
For discriminant validity, the PFRI scores from the 50 athletes with NP who participated in the test-retest reliability evaluation were compared with those of the healthy athletes. The PFRI scores for athletes with NP (32.2 ± 19.04) were statistically worse than those of healthy athletes (3.7 ± 2.5) (Levenes’s test: F = 69.001, P < 0.001; t = 10.5, df = 50.7, P < 0.001).
For the evaluation of the concurrent criterion validity, Spearman’s rho displayed an excellent correlation between the PFRI scores and the NRS (correlation coefficient = 0.94, P < 0.001; 95%CI: 0.9-0.97).
An excellent correlation was found between the PFRI and the NDI (Pearson correlation coefficient = 0.995, P < 0.001; 95%CI: 0.99-1.0) for construct validity.
Relative reliability
Cronbach’s α coefficient of internal consistency was 0.96, and values of Cronbach’s α if an item was deleted ranged between 0.961 and 0.964. Corrected item-total correlation ranged from 0.812 to 0.896 (Table 2).
Table 2.
Cronbach’s alpha and item-total statistics for persian functional rating index
| FRI items | Scale mean if item deleted | Scale variance if item deleted | Corrected item-total correlation | Squared multiple correlation | Cronbach’s alpha if item deleted |
| Pain intensity | 10.89 | 34.240 | 0.877 | 0.801 | 0.963 |
| Sleeping | 11.45 | 33.563 | 0.823 | 0.724 | 0.964 |
| Personal care | 11.02 | 33.353 | 0.852 | 0.780 | 0.963 |
| Travel | 10.83 | 31.819 | 0.852 | 0.753 | 0.963 |
| Work | 11.04 | 34.463 | 0.867 | 0.804 | 0.963 |
| Recreation | 11.07 | 33.399 | 0.846 | 0.735 | 0.963 |
| Frequency of pain | 10.57 | 32.591 | 0.812 | 0.750 | 0.964 |
| Lifting | 10.97 | 33.686 | 0.831 | 0.723 | 0.963 |
| Walking | 11.58 | 31.620 | 0.896 | 0.865 | 0.961 |
| Standing | 11.64 | 31.930 | 0.883 | 0.854 | 0.962 |
FRI: Functional rating index.
ICCagreement was excellent for test-retest measurements (ICCagreement = 0.96, 95%CI: 0.93-0.98, P < 0.001) (Table 3).
Table 3.
Results of relative and absolute reliability measures for the Persian Functional Rating Index in athletes with neck pain (n = 50)
| Scale | Mean ± SD |
d (SD) | ICCagreement (95%CI) | SEM | SDC | |
| Test | Retest | |||||
| PFRI | 32.15 ± 19.04 | 30.70 ± 15.90 | 1.45 (4.95) | 0.96 (0.93-0.98) | 3.2 | 8.84 |
d: Mean difference of the test and retest scores; ICC: Intraclass correlation coefficient; SEM: Standard error of measurement; SDC: Smallest detectable change; PFRI: Persian Functional Rating Index.
Absolute reliability
The SEM and the SDC were calculated to be 3.2 (95%CI: -6.25-6.25) and 8.84, respectively (Table 3).
Factor analysis
The Kaiser-Meyer-Olkin was 0.94, which indicates the adequacy of the sample for performing the factor analysis. The Bartlett’s test of sphericity produced a high χ2 of 1107.421, df = 45, P < 0.001, which indicates that the factor model was appropriate. The PCA with VR revealed a model with 1 factor, explaining 78.03% of the total variance. Figure 1 shows the scree plot curve for factor analysis of the 10-item PFRI.
Figure 1.
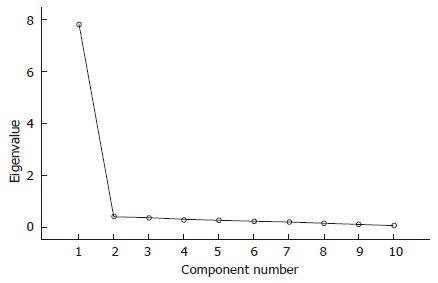
Scree plot of eigenvalues produced 1 factor for persian functional rating Index in athletes with neck pain (n = 100).
DISCUSSION
In this study, the PFRI was evaluated for validity and reliability in Persian-speaking adult athletes with NP, and it was shown to have excellent psychometric properties. All athletes with NP completed the PFRI without any problem, indicating the cultural acceptability and clinical utility of the questionnaire. The PFRI, consistent with the previous validation study in athletes with low back pain[10], is a valid and reliable tool for measuring pain and functional status in athletes with NP. To the best of our knowledge, this is the first study validating a self-administered instrument for assessing athletes with NP.
All athletes completed the PFRI without any difficulties and with no missing responses. Responding to all questions on PFRI indicates acceptability and clinical utility. The distribution of the PFRI was satisfactory as demonstrated by the absence of floor or ceiling effects. The lack of floor or ceiling effects indicates the content validity and the responsiveness of the PFRI, in accordance with findings in athletes with LBP[10].
When PFRI scores for athletes with NP were compared to the scores of healthy participants, the athletes with NP had significantly worse scores and function. This finding suggests that the PFRI discriminated athletes with NP from healthy controls. In a study which tested the ability of the PFRI to discriminate athletes with LBP from healthy athletes, a similar finding was found[10]. These data indicate that the discriminant validity of the Persian FRI in athletes with NP or LBP is consistent with those observed in the general population[8,9].
The excellent correlation between the PFRI and the NRS suggests the concurrent validity of the PFRI in athletes with NP. Our finding is in accordance with that in athletes with LBP (rho = 0.72)[10].
Construct validity was assessed by correlating the PFRI with the NDI, and, as hypothesized, excellent association was observed between the two tools. The significant correlation between the PFRI with the Persian NDI suggests that these two questionnaires measure similar construct. A similar result was found for the PFRI in athletes with LBP (r = 0.83)[10].
The PFRI showed excellent internal consistency as reflected in a Cronbach’s α value well above the minimum recommended value. Cronbach’s alpha when an item was deleted was very close to the overall alpha, which indicates similar contribution of each PFRI item to the construct measured. These results support the homogeneity and interrelatedness of the PFRI items. The internal consistency found in the present study was similar to that observed by Naghdi et al[10] when the PFRI was applied in athletes with LBP (Cronbach’s α = 0.90).
The test-retest reliability of the PFRI in athletes with NP between two assessment sessions was found to be excellent (ICCagreement = 0.96) in agreement with the result (ICCagreement = 0.97), as similarly reported in athletes with LBP[10]. The high value of ICCagreement found in this study indicated excellent reproducibility of the PFRI and consistency of the scores between two measurements.
The SEM found in this study was small, which indicates the reliability of the PFRI to identify real changes. The SDC is a useful estimate to identify real change score in an individual patient after an intervention. The SDC in the present study was 8.84%, which is clinically acceptable. This indicates only a change score greater than 9.0% can be interpreted as a real change with a 95% confidence using the PFRI. Estimation of SEM and SDC were not reported for the PFRI in athletes with LBP[10].
Factor analysis was applied to determine the possible subscales of the PFRI despite acceptable Cronbach’s α and item-total correlation values found in this study. The factor analysis resulted in a 1-factor solution for the PFRI, in accordance with results demonstrated in athletes with LBP[10]. The factor analysis confirmed that the PFRI assessed predominantly a distinct factor of the underlying construct concerning pain and function. This finding provides further evidence for construct validity of the PFRI. The PFRI can be used independently to identify changes in pain and function of athletes with NP.
There were limitations for the present study. First, the effect size based responsiveness of the PFRI to detect change over time was not evaluated in this study. The evaluation of floor and ceiling effects is one of the methods used for quantifying responsiveness[17,18]. The lack of floor and ceiling effects found in this study implies that the PFRI is able to detect changes following treatment. Second, this study assessed only the Persian FRI. An English FRI must be separately validated for athletes with NP.
In conclusion, the PFRI demonstrated excellent validity and reliability, and therefore, can be used in both clinical and research settings for athletes with NP.
ACKNOWLEDGMENTS
The authors would like to thank the Research Deputy at Tehran University of Medical Sciences. We also thank the athletes who participated in the study.
COMMENTS
Background
Neck pain (NP) is one of the common complaints in athletes. Reliable and valid tests are required to accurately examine the athletes with NP. There are various self-report questionnaires [e.g., Functional Rating Index (FRI)] developed for evaluation of disability in patients with various spinal conditions such as NP. The self-report questionnaires allow the clinicians to evaluate the extent to which spinal disorders affect pain and function perceived by patients. However, the commonly used self-report questionnaires are developed for use in general population with spinal disorders.
Research frontiers
It is necessary to use self-report questionnaires validated specifically for athletes with NP. The current research hotspot is that there is no specific test available for assessing athletes with NP. It is, therefore, necessary to develop either new self-report questionnaires or validate existing instruments for athletes with NP.
Innovations and breakthroughs
FRI is one of the commonly used self-report instrument to evaluate the patients’ perspectives on their disability in general population with low back pain (LBP) as well as NP. The FRI first developed in English language is reliable, valid and responsive, and has been adapted and validated into various languages. The Persian FRI (PFRI) is previously validated for athletes with LBP. This report presents a study, for the first time, validating the PFRI in athletes with NP. The results show satisfactory psychometric properties of PFRI for use in athletes with NP.
Applications
The results of the present study demonstrated that the PFRI is reliable and valid in athletes with NP and it may be useful for assessing pain and functional status of Persian speaking athletes with NP. The equivalency of PFRI with the original English version indicates that the FRI is reliable and valid in athletes with NP, and may be used in multinational investigations as an outcome measure.
Terminology
Many athletes may experience NP due to ligament sprains, muscle strains, and contusions. The athletes with NP may complain from deficits in neck mobility, muscle recruitment, strength, endurance, or postural stability. The FRI is a quick, self-report questionnaire used to assess disability in patients with both LBP and NP. The scale contains 10 questions measuring both pain and function in a five-point scale from 0 (no pain/full function) to 4 (worst possible pain/unable to perform function). Total score calculated in percentage range between 0% and 100%, with higher scores indicating higher disability.
Peer-review
This paper is a well designed paper and gives out the result that the other scoring system can be used for evaluation for neck pain of the athletes.
Footnotes
Institutional review board statement: The study was reviewed and approved by the review board, School of Rehabilitation, Tehran University of Medical Sciences.
Informed consent statement: All subjects gave their informed consent prior to the study enrolment.
Conflict-of-interest statement: The authors have no competing interests to declare.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Specialty type: Orthopedics
Country of origin: Iran
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): 0
Grade C (Good): C, C, C
Grade D (Fair): 0
Grade E (Poor): 0
Peer-review started: February 18, 2016
First decision: March 25, 2016
Article in press: June 3, 2016
P- Reviewer: Kuptniratsaikul V, Wu WT, Yang HO S- Editor: Qiu S L- Editor: A E- Editor: Wu HL
References
- 1.Villavicencio AT, Hernández TD, Burneikiene S, Thramann J. Neck pain in multisport athletes. J Neurosurg Spine. 2007;7:408–413. doi: 10.3171/SPI-07/10/408. [DOI] [PubMed] [Google Scholar]
- 2.Wilber CA, Holland GJ, Madison RE, Loy SF. An epidemiological analysis of overuse injuries among recreational cyclists. Int J Sports Med. 1995;16:201–206. doi: 10.1055/s-2007-972992. [DOI] [PubMed] [Google Scholar]
- 3.Zmurko MG, Tannoury TY, Tannoury CA, Anderson DG. Cervical sprains, disc herniations, minor fractures, and other cervical injuries in the athlete. Clin Sports Med. 2003;22:513–521. doi: 10.1016/s0278-5919(03)00003-6. [DOI] [PubMed] [Google Scholar]
- 4.Michaelson P, Michaelson M, Jaric S, Latash ML, Sjölander P, Djupsjöbacka M. Vertical posture and head stability in patients with chronic neck pain. J Rehabil Med. 2003;35:229–235. doi: 10.1080/16501970306093. [DOI] [PubMed] [Google Scholar]
- 5.O’Leary S, Jull G, Kim M, Vicenzino B. Cranio-cervical flexor muscle impairment at maximal, moderate, and low loads is a feature of neck pain. Man Ther. 2007;12:34–39. doi: 10.1016/j.math.2006.02.010. [DOI] [PubMed] [Google Scholar]
- 6.Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM, Sopky BJ, Godges JJ, Flynn TW. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38:A1–A34. doi: 10.2519/jospt.2008.0303. [DOI] [PubMed] [Google Scholar]
- 7.Feise RJ, Michael Menke J. Functional rating index: a new valid and reliable instrument to measure the magnitude of clinical change in spinal conditions. Spine (Phila Pa 1976) 2001;26:78–86; discussion 87. doi: 10.1097/00007632-200101010-00015. [DOI] [PubMed] [Google Scholar]
- 8.Ansari NN, Feise RJ, Naghdi S, Ebadi S, Yoosefinejad AK. The functional rating index: reliability and validity of the Persian language version in patients with low back pain. Spine (Phila Pa 1976) 2011;36:E1573–E1577. doi: 10.1097/BRS.0b013e3182103282. [DOI] [PubMed] [Google Scholar]
- 9.Ansari NN, Feise RJ, Naghdi S, Mohseni A, Rezazadeh M. The functional rating index: reliability and validity of the Persian language version in patients with neck pain. Spine (Phila Pa 1976) 2012;37:E844–E848. doi: 10.1097/BRS.0b013e31824b5bde. [DOI] [PubMed] [Google Scholar]
- 10.Naghdi S, Ansari NN, Yazdanpanah M, Feise RJ, Fakhari Z. The validity and reliability of the functional rating index for evaluating low back pain in athletes. Scand J Med Sci Sports. 2015;25:840–845. doi: 10.1111/sms.12447. [DOI] [PubMed] [Google Scholar]
- 11.Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, Bouter LM, de Vet HC. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42. doi: 10.1016/j.jclinepi.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 12.Mousavi SJ, Parnianpour M, Montazeri A, Mehdian H, Karimi A, Abedi M, Ashtiani AA, Mobini B, Hadian MR. Translation and validation study of the Iranian versions of the Neck Disability Index and the Neck Pain and Disability Scale. Spine (Phila Pa 1976) 2007;32:E825–E831. doi: 10.1097/BRS.0b013e31815ce6dd. [DOI] [PubMed] [Google Scholar]
- 13.Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149–158. doi: 10.1016/S0304-3959(01)00349-9. [DOI] [PubMed] [Google Scholar]
- 14.Feise RJ, Menke JM. Functional Rating Index: literature review. Med Sci Monit. 2010;16:RA25–RA36. [PubMed] [Google Scholar]
- 15.Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14:409–415. [PubMed] [Google Scholar]
- 16.Haefeli M, Elfering A. Pain assessment. Eur Spine J. 2006;15 Suppl 1:S17–S24. doi: 10.1007/s00586-005-1044-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Terwee CB, Dekker FW, Wiersinga WM, Prummel MF, Bossuyt PM. On assessing responsiveness of health-related quality of life instruments: guidelines for instrument evaluation. Qual Life Res. 2003;12:349–362. doi: 10.1023/a:1023499322593. [DOI] [PubMed] [Google Scholar]
- 18.Ansari NN, Naghdi S, Hasanvand S, Fakhari Z, Kordi R, Nilsson-Helander K. Cross-cultural adaptation and validation of Persian Achilles tendon Total Rupture Score. Knee Surg Sports Traumatol Arthrosc. 2016;24:1372–1380. doi: 10.1007/s00167-015-3977-x. [DOI] [PubMed] [Google Scholar]