

Abstract
Objective:
Petit mal epilepsy or absence seizures involve brief, sudden lapses of consciousness and most often occurs in people under age of 20 years. This study was done to find out the most likely significant age affected by petit mal epilepsy and whether they had higher rate of behavioral, educational, and social problems.
Materials and Methods:
We run tests on total 32 patients (male 16 and female 16) from newborns to 20 years of age.
Results:
The most affected ages were from 4 to 9 years and both genders were equally affected. They have higher rate of behavioral, educational, and social problems, and most likely recovering ages from the disease were from 15 to 20 years.
Conclusion:
These findings could contribute in diagnosis and treatment of Petit Mal Epilepsy, as it often misinterpreted as daydreaming or inattention.
Key words: Absence seizure, electroencephalography, epilepsy, petit mal epilepsy
Introduction
Petit mal epilepsy or absence seizure is an uncommon seizure that begins suddenly and occurs without any warning signs. Affecting about 2 of every 1000 people, these are caused by abnormal and intense electrical activity in the brain.[1] Those who are experiencing absence seizures typically appear to stare without moving, it can occur many times a day and usually lasting <15 s followed by full recovery. Signs and symptoms of absence seizures include sudden stop in motion without falling, lip smacking, eyelid flutters, chewing motions, finger rubbing, and small movements of both hands. Childhood absence epilepsy accounts for 10-17% of all cases of childhood onset epilepsy, making it the most common form of pediatric epilepsy.[2,3,4] Petit mal epilepsy has two essential components: Clinical (impairment of consciousness) and electroencephalography (EEG).[5,6] The primary diagnostic test for absence seizures is EEG (shows generalized spike-and-slow wave discharges) and/or computed tomography (CT)/magnetic resonance imaging (MRI) (exclude other neurological disease such as stroke or a brain tumor). Fortunately, about 70% of children outgrow absence seizures by the time they are teenagers, especially if the seizures developed before the age of 9. Although most children who develop seizures of this type have experienced normal growth and development, there is a somewhat higher frequency of behavioral and educational problems with these children.[1,7] The patients with petit mal epilepsy who are treated with valproic acid or ethosuximide, which are of equal efficacy controlling absences in around 75% of patients. The patiets with petit mal epilepsy who are also treated lamotrigine monotherapy, which is less effective, with nearly half of the patients becoming seizure free.[2]
Aims and objectives
To find out the most likely ages to be affected by petit mal epilepsy
To find out whether patients with petit mal epilepsy have higher rate of behavioral, educational, and social problems
To find out most likely age to recover from petit mal epilepsy in children in most of the cases.
Materials and Methods
The study performed here was descriptive cross-sectional study. EEG and/or CT/MRI were used to diagnose the patient with petit mal epilepsy. In previously diagnosed cases, the diagnostic history was duly noted. The target population was those came at the Taihe Hospital of Hubei University of Medicine, Shiyan, Hubei, P. R. China. The study period was from January 1, 2016 to May 15, 2016. On this study, patients with petit mal epilepsy ware included up to the age of 20 years.
Consent
Before including in this study, the parents/patients were explained the purpose of the study. Once the verbal consent was obtained with the presence of a nurse, a written form has given both in English and Chinese language to get the written informed consents, patients/whose parents gave consent, were only enrolled in this study.
Ethical considerations
According to WHO guidelines of ethical consideration, following steps were followed:
All the interviews were conducted with prior consent of the respondents
Respondents were told that the data collected from the interview would be kept confidential and would be used for the study purpose only
No incentive was given to the respondents.
Quality control and quality assurance
As a part of quality control and quality assurance of data collected, the selected volunteers with sufficient eligibility had been trained in accordance to the structure of the questionnaire and the objectives of the study. The researcher was present in each and every occasion to look after the data collection procedure and to assist the data collectors in collecting the data and the study subjects in understanding the questions or other assistances if applicable. He was present also to make sure that the data collection goes smoothly without any administrative complexities and/or logistic shortcomings.
Reliability and limitation of the study
The hospital provides services for heterogeneous group of people from different societies: To all those who seek medical service of the hospital irrespective of their social class, level of education and profession. Target samples for the study were very hard to reach, so random sampling technique was followed which may cause bias and errors in the design and analysis phases of the study. Only one person was involved in taking clinical history. Therefore, the study would be reliable to draw conclusion. However, personal bias is still possible, as no cross-checking was done further.
Study procedure and data collection
Runs tests on total 32 patients from newborns to 20 years of age younger people to check the most affecting age of petit mal epilepsy and recovery age from it. Out of these total 32 patients, 16 were male and 16 were female patients to find out their individual affecting and recovering status. To diagnose petit mal epilepsy has been used EEG and CT. Gathered full history of petit mal epilepsy of these 32 patients (newly affected and those who is recovering from petit mal epilepsy). History of diagnosis has been recorded and drugs been used to treat petit mal epilepsy. Given balanced diet with regular healthy meals is of benefit in maintaining general health and wellbeing.
Results and Observation
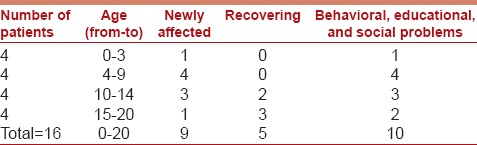
In this study, 32 patients (16 males and 16 females) were included from the Taihe Hospital of Hubei University of Medicine, Shiyan, Hubei, P. R. China. The most significant affecting ages of petit mal epilepsy were from 4 to 9 years for both male (n = 16) and female (n = 16) patients. Both the male (n = 16) and female (n = 16) are almost equally affected (8 males and 9 females were newly affected). Petit mal epilepsy patients do have higher rate of behavioral, educational and social problems. The most likely ages of recovering from petit mal epilepsy are 15-20 years [Tables 1 and 2].
Table 1.
Data collection of male patients (n=16)
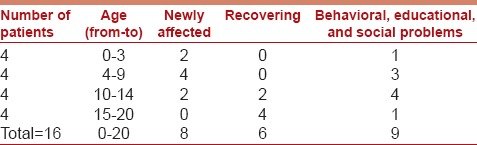
Table 2.
Data collection of female patients (n=16)
Discussion
Although petit mal epilepsy is relatively uncommon, the study that we have done here about the mean age of petit mal epilepsy is highly relevant and important. Very few studies can be found about the petit mal epilepsy. In addition, the general measures about the petit mal epilepsy including the mean affecting ages, ways of diagnosis, treatment and recovery stage should be known. This study could help us understand more about the mean affecting ages, gender mostly affected, and recovery stages of the petit mal epilepsy. Petit mal epilepsy rarely causes a true convulsion in which the person falls or collapses. Despite briefly losing consciousness, the person recovers fully with no lingering confusion or other ill effects. In children, absence seizures may interfere with learning and are often misinterpreted as daydreaming or inattention.[1] While diagnosing, in addition to EEG and/or CT/MRI, blood tests may also be ordered to check for other health problems that may be causing the seizures. In the treatment of petit mal epilepsy, there is often insufficient evidence for which of the available medications has the best combination of safety and efficacy for a particular patient.[8] Carbamazepine, vigabatrin, and tiagabine are contraindicated in the treatment of absence seizures, irrespective of cause and severity. This is based on clinical and experimental evidence.[9] In particular, the gamma-aminobutyric acid agonists vigabatrin and tiagabine are used to induce, not to treat, absence seizures and absence status epilepticus.[10] Even though many children with petit mal epilepsy gradually outgrow them over months to years, some children with absence seizures may also experience tonic-clonic seizures.[2] Hence, appropriate measures should be taken on time in case of petit mal epilepsy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mattson RH. Overview: Idiopathic generalized epilepsies. Epilepsia. 2003;44:2–6. doi: 10.1046/j.1528-1157.44.s.2.3.x. [DOI] [PubMed] [Google Scholar]
- 2.Glauser TA, Cnaan A, Shinnar S, Hirtz DG, Dlugos D, Masur D, et al. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy. N Engl J Med. 2010;362:790–9. doi: 10.1056/NEJMoa0902014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Berg AT, Shinnar S, Levy SR, Testa FM, Smith-Rapaport S, Beckerman B. How well can epilepsy syndromes be identified at diagnosis? A reassessment 2 years after initial diagnosis. Epilepsia. 2000;41:1269–75. doi: 10.1111/j.1528-1157.2000.tb04604.x. [DOI] [PubMed] [Google Scholar]
- 4.Jallon P, Loiseau P, Loiseau J. Newly diagnosed unprovoked epileptic seizures: presentation at diagnosis in CAROLE study. Epilepsia. 2001;42:464–75. doi: 10.1046/j.1528-1157.2001.31400.x. [DOI] [PubMed] [Google Scholar]
- 5.Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia. 1981;22:489–501. doi: 10.1111/j.1528-1157.1981.tb06159.x. [DOI] [PubMed] [Google Scholar]
- 6.Panayiotopoulos CP. Typical absence seizures and related epileptic syndromes: Assessment of current state and directions for future research. Epilepsia. 2008;49:2131–9. doi: 10.1111/j.1528-1167.2008.01777.x. [DOI] [PubMed] [Google Scholar]
- 7.Kyllerman M. In: Aicardi's epilepsy in children. 3rd ed. Arzimanoglou A, Guerrini R, Aicardi J, editors. Philadelphia: Lippincott Williams and Wilkins; 2004. [Google Scholar]
- 8.Posner EB, Mohamed KK, Marson AG. Ethosuximide, sodium valproate or lamotrigine for absence seizures in children and adolescents. Cochrane Database Syst Rev. 2005 doi: 10.1002/14651858.CD003032.pub2. [DOI] [PubMed] [Google Scholar]
- 9.Panayiotopoulos CP. Imitators of epileptic seizures. A clinical guide to epileptic syndromes and their treatment. Springer. 2010:97–134. [Google Scholar]
- 10.Rektor I. Comments on Knake S, Hamer HM, Rosenow F. Status epilepticus: A critical review. Epilepsy Behav. 2009;15:10–4. doi: 10.1016/j.yebeh.2009.02.027. Epilepsy Behav 2014;40:56-7. [DOI] [PubMed] [Google Scholar]