

CASE REPORT
A 20-year-old man was admitted to our hospital with complaints of frontal headache, sinusitis, and fever for one week. He had a history of allergic rhinitis and recurrent sinus infections. At admission his temperature was 40°C and his pulse rate was 140 beats per minute. On physical examination, the center of his forehead had a soft, tender, warm, swollen area that caused an obvious bulge. The initial imaging study, a computed tomography scan, failed to clearly show the intracranial pathology. A magnetic resonance imaging study of the patient’s head with intravenous contrast revealed osteomyelitis of the frontal bone with localized swelling and underlying epidural empyema (Figures 1 and 2). This finding confirmed the diagnosis of Pott puffy tumor, which is defined as forehead swelling, usually from the anterior extension of frontal sinusitis, and associated osteomyelitis of the frontal bone.1,2
Figure 1.
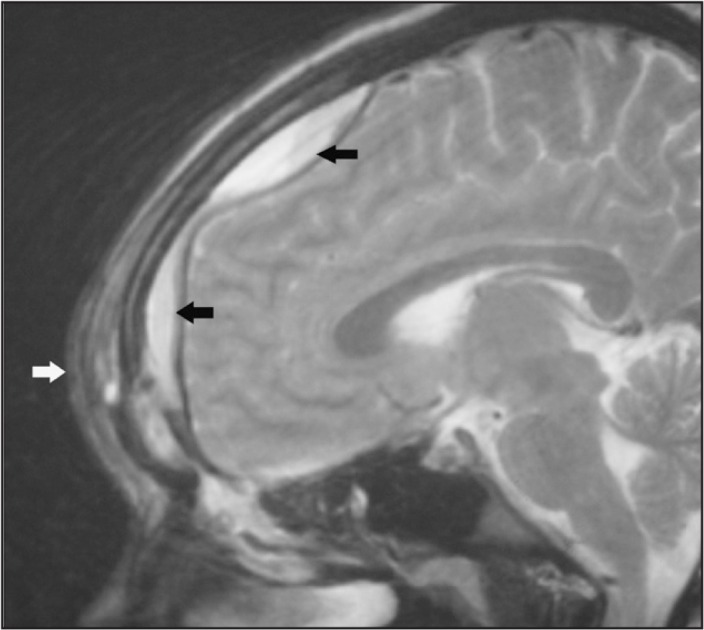
Sagittal-view magnetic resonance image of the cranium with intravenous contrast. The black arrows indicate epidural empyema. The white arrow indicates localized swelling.
Figure 2.
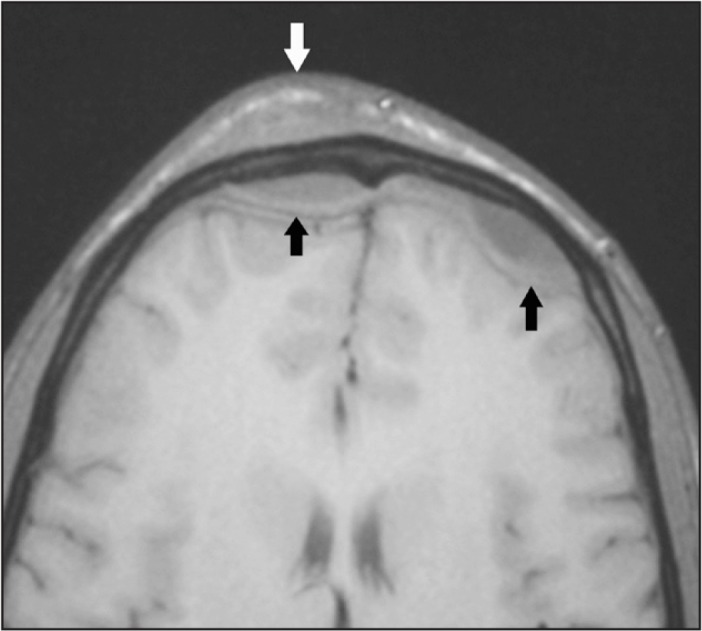
Axial-view magnetic resonance image of the cranium with intravenous contrast. The black arrows indicate epidural empyema. The white arrow indicates localized swelling.
The patient was seen by otorhinolaryngology as well as neurosurgery; he declined the recommended surgery and consequently remained febrile with a maximum temperature of over 38°C for 6 consecutive days. He continued to have occasional fever spikes and was not discharged until hospital day 39. During hospitalization he was treated with intravenous ampicillin and sulbactam every 6 hours. At discharge, his treatment was changed to oral metronidazole and daily intravenous ceftriaxone via a central catheter. He received a total of 3 months of antibiotic treatment and remained well after the antibiotic treatment was completed.
DISCUSSION
Sir Percivall Pott (1714–1788), a surgeon at St Bartholomew’s Hospital in London, first described Pott puffy tumor in 1760.3 It was called a tumor because tumor refers to one of the four historic manifestations of inflammation noted by Aulus Cornelius Celsus (c 25 BC–c 50 AD): rubor (redness), tumor (swelling), calor (warmth), and dolor (pain). Originally described as a complication of head trauma, Pott puffy tumor typically occurs as a complication of frontal sinusitis. The extracranial manifestations frequently include subperiosteal or subgaleal abscesses. Intracranial complications may include epidural empyema, subdural empyema, intraparenchymal abscess, cavernous sinus thrombosis, or meningitis.4
A review of 53 cases of Pott puffy tumor5 indicated that sinusitis, head trauma, or cranial surgery are the usual predisposing factors; the majority of cases occurred in younger males. Culture results indicated the frequent pathogens were Streptococcus species (47%), anaerobic species (28%), and Staphylococcus aureus (22%). Almost half of the cultures revealed mixed infections with more than one isolate. Epidural and subdural empyema were the most frequently reported intracranial complications.5
Pott puffy tumor is treated with surgery and antibiotics. Surgical treatment includes drainage of the frontal sinus and other areas of infection. Broad-spectrum antibiotics that have good central nervous system penetration must be started on diagnosis. Prolonged antibiotic treatment is required after surgery because osteomyelitis is usually present.
Footnotes
Disclosure Statement
The author(s) have no conflicts of interest to disclose.
References
- 1.Bambakidis NC, Cohen AR. Intracranial complications of frontal sinusitis in children: Pott’s puffy tumor revisited. Pediatr Neurosurg. 2001;35(2):82–9. doi: 10.1159/000050395. . [DOI] [PubMed] [Google Scholar]
- 2.Koch SE, Wintroub BU. Pott’s puffy tumor. A clinical marker for osteomyelitis of the skull. Arch Dermatol. 1985;121(4):548–9. doi: 10.1001/archderm.1985.01660040132029. . [DOI] [PubMed] [Google Scholar]
- 3.Pott P. Observations on the nature and consequences of wounds and contusions of the head, fractures of the skull, concussions of the brain, &c. London, England: Hitch & Hawes; 1760. pp. 22–58. [Google Scholar]
- 4.Wells RG, Sty JR, Landers AD. Radiological evaluation of Pott puffy tumor. JAMA. 1986 Mar 14;255(10):1331–3. doi: 10.1001/jama.1986.03370100125030. . [DOI] [PubMed] [Google Scholar]
- 5.Skomro R, McClean KL. Frontal osteomyelitis (Pott’s puffy tumour) associated with Pasteurella multocida—a case report and review of the literature. Can J Infect Dis. 1998 Mar;9(2):115–21. doi: 10.1155/1998/457984. [DOI] [PMC free article] [PubMed] [Google Scholar]