

Introduction
Neutrophilic infiltrates in the setting of systemic lupus erythematosus (SLE) are commonly associated with bullous or vasculitic disease. Recently, an increasing number of reports describe a nonbullous, nonvasculitic SLE-associated neutrophilic dermatosis. Prior cases of SLE-associated neutrophilic dermatosis describe an urticarial eruption involving the trunk and extremities. Here we report the case of a 27-year-old woman with SLE-associated neutrophilic dermatosis with palmoplantar involvement, thus, expanding the clinical spectrum of this disease. Neutrophilic dermatosis may represent the initial cutaneous manifestation of systemic disease in one-third of patients. Thus, prompt recognition of this distinct cutaneous entity should promote screening for SLE.
Case report
A 27-year-old woman with a 9-month history of SLE was admitted to the hospital with 4 days of worsening pleuritic chest pain, dyspnea, and arthralgias. She also had a 1-day history of a burning, annular eruption on her trunk, palms, and soles. Upon admission, the patient was found to have recurrent pericardial and bilateral pleural effusions in the setting of an acute SLE flare. Although complete blood count and basic metabolic panel were unremarkable, the patient's anti–double-stranded DNA antibody was 266 IU/mL, C3 was 41.4 mg/dL (laboratory-specific reference range, 90–180 mg/dL), and C4 was 6.62 mg/dL (laboratory-specific reference range, 10–40 mg/dL). From prior workup of SLE, antinuclear antibody was 1:640 with speckled pattern and was anti-Smith antibody positive and antiribonucleoprotein antibody positive. Anti–SS-A antibody was 7.3 (normal <0.9 antibody index) and anti–SS-B antibody was 0.6 (normal <0.9 antibody index). Erythrocyte sedimentation rate was 45 mm/h.
On physical examination, the patient had blanchable, erythematous macules and annular, urticarial papules and plaques bilaterally distributed on the palmoplantar surfaces (Fig 1). Additionally, there were faint, blanchable, erythematous macules on the chest and back. Shave biopsy findings of the left plantar surface showed neutrophils aligned along the dermoepidermal junction (DEJ) associated with vacuolar alteration and rare dyskeratosis (Fig 2). There was also a superficial, perivascular, and interstitial predominantly neutrophilic infiltrate with lymphocytes and leukocytoclasia, without vasculitis or a significant increase in dermal mucin (Fig 3).
Fig 1.

SLE-associated neutrophilic dermatosis. Erythematous macules and annular, urticarial papules and plaques bilaterally distributed on the palmar surfaces.
Fig 2.
Acral skin with neutrophils aligned along the DEJ associated with vacuolar alteration and rare dyskeratosis. (Hematoxylin-eosin stain.)
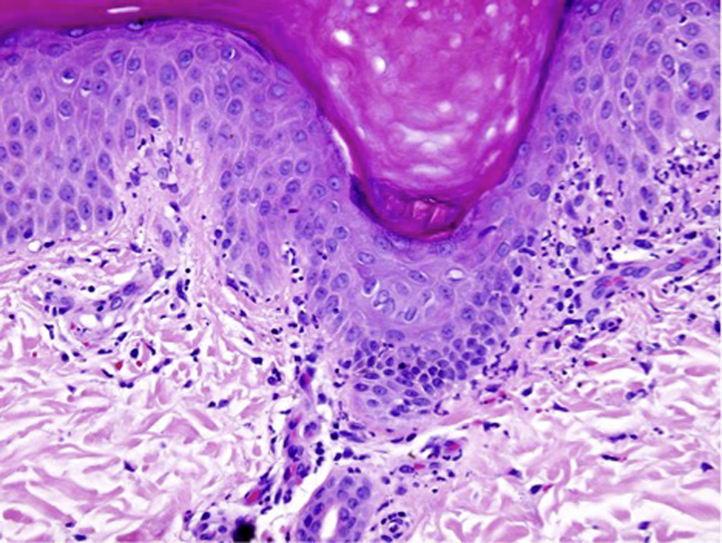
Fig 3.

Neutrophil-medicated vacuolar alteration along the DEJ with a necrotic keratinocyte. There is also a perivascular and interstitial neutrophilic infiltrate with leukocytoclasia in the absence of vasculitis. (Hematoxylin-eosin stain.)
At the time of presentation, the patient was taking hydroxychloroquine (200 mg twice daily), prednisone (50 mg/d), omeprazole, atovaquone, and cholecalciferol. She was treated with intravenous methylprednisolone and underwent a thoracentesis with improvement in respiratory status and resolution of chest pain. Palmoplantar surfaces were treated with clobetasol ointment twice daily with only modest improvement; however, shortly after an increase in systemic glucocorticoids and the initiation of mycophenolate mofetil, the eruption subsided. At 5-month follow-up, the patient remained free of the cutaneous eruption while maintained on hydroxychloroquine (200 mg twice daily) and mycophenolate mofetil (1500 mg twice daily). Methylprednisolone had been tapered down to 10 mg daily.
Discussion
Ackerman was among the first to consider SLE in the histologic differential diagnosis of nonbullous, nonvasculitic neutrophilic inflammatory dermatosis.1, 2 He described the presence of neutrophils and neutrophilic dust immediately beneath the epidermis of an interface dermatitis and postulated that these histopathologic features may represent a “muted” expression of bullous SLE.2 The first clinical case of SLE associated with a Sweet's syndrome–like dermatosis was reported in 1985.3 Since then, close to 50 cases of SLE-associated neutrophilic dermatosis distinct from Sweet's syndrome, pyoderma gangrenosum, and bullous lupus erythematosus (LE) have been reported.3, 4, 5, 6, 7, 8
The literature on neutrophil-dominant manifestations of SLE is fraught with confusion, in part because of the overlap in terminology. A variety of terms have been used to describe nonbullous, nonvasculitic, neutrophilic dermatosis and include nonbullous neutrophilic dermatosis, nonbullous neutrophilic LE, Sweet's syndrome–like neutrophilic dermatosis, and SLE-associated neutrophilic dermatosis. However, reproducible clinical and histopathologic reports confirm that SLE-associated neutrophilic dermatosis represents a distinct entity that is closely associated with and may herald the development of systemic disease.4, 5, 6, 7, 8 Clinical and histopathologic differential diagnoses of SLE-associated neutrophilic dermatosis are vast (Table 1).8, 9, 10 Although there are no known prognostic or therapeutic differences for SLE-associated neutrophilic dermatosis, recognition of this distinct cutaneous entity should prompt screening for SLE.
Table I.
Clinical and histopathologic differential diagnoses of SLE-associated neutrophilic dermatosis with separate discussion for generalized and palmoplantar cutaneous eruptions
| Diagnosis | Clinical features | Histopathologic features |
|---|---|---|
| SLE-associated neutrophilic dermatosis |
|
|
| Generalized eruption | ||
| Neutrophilic urticarial dermatosis∗9 |
|
|
| Neonatal lupus erythematosus∗ |
|
|
| Bullous SLE∗ |
|
|
| Dermatitis herpetiformis |
|
|
| Linear IgA bullous dermatosis∗ |
|
|
| Still's disease |
|
|
| Behcet's disease |
|
|
| Pyoderma gangrenosum∗ |
|
|
| Sweet's syndrome∗ |
|
|
| Palisaded neutrophilic and granulomatous dermatitis∗ |
|
|
| Leukocytoclastic vasculitis∗ |
|
|
| Hypocomplementemic urticarial vasculitis∗10 |
|
|
| Palmoplantar eruption | ||
| Palmoplantar eccrine hidradenitis |
|
|
| Palmoplantar pustulosis |
|
|
| Erythema multiforme |
|
|
BMZ, basement membrane; DIF, direct immunofluorescence.
Neutrophil-dominant dermatoses that may occur in association with SLE.
The cutaneous findings of SLE-associated neutrophilic dermatosis include erythematous papules and plaques, many of which are described as urticarial and some of which have an annular morphology, most commonly involving the trunk and extremities, and without bulla formation or mucosal involvement.
Histopathologic features include an interstitial and perivascular predominantly neutrophilic infiltrate with leukocytoclasia and variable vacuolar alteration along the DEJ, without the presence of vasculitis or bullae.5 The degree of neutrophilic infiltrate varies from paucicellular to cell rich Sweet's syndrome like, which suggests a spectrum of neutrophilic dermatoses within SLE patients. Perivascular lymphocytes are also typically present in small numbers. Histopathologic changes that are consistent with SLE, such as interface changes, dermal mucin, and basement membrane thickening, are variably present. When performed, direct immunofluorescence is positive for immunoreactants at the DEJ in 50% of cases, with deposition of C3, IgG, and IgM along the DEJ.8 Currently, treatment is targeted at the underlying disease, and the eruption usually responds to immunomodulatory or immunosuppressive therapy.6
The pathogenesis of these nonbullous lesions remains unclear. Many patients develop the eruption while on immunosuppressive therapy, which may inhibit the formation of bullae and supports the idea of a forme fruste variant of bullous LE, as suggested by Ackerman.2 Other patients have the eruption as the presenting symptom of SLE without concurrent systemic therapy, suggesting that this could be a distinct cutaneous manifestation of SLE. Although absent in some cases, histopathologic findings characteristic of SLE, such as vacuolar alteration and immunoreactants along the DEJ, raise the possibility of an antibody-mediated pathogenesis. The occurrence of this entity in patients with other autoimmune connective-tissue disorders, such as rheumatoid arthritis, Still's disease, and Sjögren's syndrome, has been reported, suggesting that the disorder represents a clinicopathologic response in individuals predisposed by diverse autoimmune connective-tissue disorders and not exclusively SLE.6
This case shows unique palmoplantar involvement of SLE-associated neutrophilic dermatosis. Increased awareness and recognition of the clinical spectrum of neutrophilic dermatoses in the setting of SLE is imperative, particularly in the one-third of cases in which cutaneous manifestations are the presenting symptoms of systemic disease.
Footnotes
Funding sources: None.
Conflicts of interest: None declared.
This case report has been accepted for poster presentation at the 2016 AAD Summer Meeting in Boston, Massachusetts on Friday, July 29 in the Connective Tissue Diseases section.
References
- 1.Yell J.A., Mbuagbaw J., Burge S.M. Cutaneous manifestations of systemic lupus erythematosus. Br J Dematol. 1996;135(3):355–362. [PubMed] [Google Scholar]
- 2.Ackerman A.B. 2nd ed. Williams & Wilkins; Baltimore: 1997. Histologic Diagnosis of Inflammatory Skin Diseases: An Algorithmic Method Based On Pattern Analysis. P.525, 542. [Google Scholar]
- 3.Goette D.K. Sweet's syndrome in subacute cutaneous lupus erythematosus. Arch Dermatol. 1985;121(6):789–791. [PubMed] [Google Scholar]
- 4.Gleason B.C., Zembowicz A., Granter S.R. Non-bullous neutrophilic dermatosis: an uncommon dermatologic manifestation in patients with lupus erythematosus. J Cutan Pathol. 2006;33(11):721–725. doi: 10.1111/j.1600-0560.2006.00559.x. [DOI] [PubMed] [Google Scholar]
- 5.Brinster N.K., Nunley J., Pariser R., Horvath B. Nonbullous neutrophilic lupus erythematosus a newly recognized variant of cutaneous lupus erythematosus. J Am Acad Dermatol. 2012;66(1):92–97. doi: 10.1016/j.jaad.2009.05.019. [DOI] [PubMed] [Google Scholar]
- 6.Saeb-Lima M., Charli-Joseph Y., Rodríguez-Acosta E.D., Domínguez-Cherit J. Autoimmunity-related neutrophilic dermatosis: a newly described entity that is not exclusive of systemic erythematosus. Am J Dermatopathol. 2013;35(6):655–660. doi: 10.1097/DAD.0b013e3182840f7f. [DOI] [PubMed] [Google Scholar]
- 7.Larson A.R., Granter S.R. Systemic lupus erythematosus-associated neutrophilic dermatosis–an under-recognized neutrophilic dermatosis in patients with systemic lupus erythematosus. Hum Pathol. 2014;45(3):598–605. doi: 10.1016/j.humpath.2013.10.029. [DOI] [PubMed] [Google Scholar]
- 8.Larson A.R., Granter S.R. Systemic lupus erythematosus-associated neutrophilic dermatosis: A review and update. Adv Anat Pathol. 2014;21(4):248–253. doi: 10.1097/PAP.0000000000000026. [DOI] [PubMed] [Google Scholar]
- 9.Kieffer C., Cribier B., Lipsker D. Neutrophilic urticarial dermatosis: a variant of neutrophilic urticaria strongly associated with systemic disease. Report of 9 new cases and review of the literature. Medicine (Baltimore) 2009;88(1):23–31. doi: 10.1097/MD.0b013e3181943f5e. [DOI] [PubMed] [Google Scholar]
- 10.Grotz W., Baba H.A., Becker J.U., Baumgärtel M.W. Hypocomplementemic urticarial vasculitic syndrome: an interdisciplinary challenge. Dtsch Arztebl Int. 2009;106(46):756–763. doi: 10.3238/arztebl.2009.0756. [DOI] [PMC free article] [PubMed] [Google Scholar]