

Abstract
Background:
Selective alveolar corticotomy is defined as an intentional injury to cortical bone. This technique is an effective means of accelerating orthodontic tooth movement. The aim of this study is to evaluate the effect of buccal corticotomy in accelerating maxillary canine retraction.
Materials and Methods:
The sample in this clinical trial study consisted of 15 adult female patients with therapeutic need for extraction of maxillary first premolars and maximum canine retraction. By use of split-mouth design, at the time of premolars extraction, buccal corticotomy was performed around the maxillary first premolar, randomly on one side of maxilla, and the other side was reserved as the control side. Canine retraction was performed by use of friction – less mechanic with simple vertical loop. Every 2 weeks, distance between canines and second premolars was measured until complete space closure. The velocity of space closure was calculated to evaluate the effect of this technique in accelerating orthodontic tooth movement. The obtained data were statistically analyzed using independent t-test, and the significance was set at 0.05.
Results:
The rate of canine retraction was significantly higher on the corticotomy side than the control side by an average of 1.8 mm/month versus 1.1 mm/month in the corticotomy side and control side, respectively (P < 0.001).
Conclusion:
Based on result of this study, corticotomy can accelerates the rate of orthodontic tooth movement about two times faster than conventional orthodontics and it is significant in early stages after surgical porsedure. Therefore Buccal corticotomy is a useful adjunct technique for accelerating orthodontic tooth movement.
Key Words: Accelerated, orthodontics, buccal, cortex, surgerycorticotomy, tooth movement
INTRODUCTION
Changed lifestyles and patient awareness have increased the demand for adult orthodontic treatment.[1] Adult patients are more susceptible to periodontal complications.[2]
In addition, prolonged treatment time is one of the definite risk factors of root resorption and periodontal damage. There is a reduced chance of root resorption[3], enamel decalcification, and better patient cooperation when treatment time is shortened.[4]
Therefore, researchers have increasingly sought and eager for finding ways to shorten orthodontic treatment time.
Several approaches have proposed for accelerating orthodontic tooth movement. These approaches can be summarized into three major groups:[5,6]
Biologic approaches or local administration of chemicals
Physical or mechanical stimulation of the alveolar bone, such as the use of lasers, piezoelectric, direct electrical current, or magnets
Surgical approaches including dental distraction and alveolar corticotomies.
Among these approaches, the method of orthodontic treatment using corticotomies has recently become popularized[2] which uses bone healing mechanisms in combination with orthodontic loads to accelerate orthodontic tooth movement and thereby decrease treatment time. Bryan was the first researcher who introduced some surgical approaches based on osteotomy to accelerate orthodontic treatment in Guilford textbook.[7] However, it was Henrich Kole's publication in 1959[8] that reintroduced a combination of osteotomy and corticotomy for reducing orthodontic treatment time. Kole believed that the continuity of cortical bone offered the most resistance to tooth movement. His surgical intervention was accomplished by creating separated bony blocks with vertical buccal and lingual corticotomies and a supra-apical horizontal osteotomy connecting mesial and distal cuts and postulated this theory as “bony block movement.”
On the other hand, Wilcko et al.[9,10,11] stated that rapid orthodontics with corticotomies is not because of creating bony blocks but is attributed to increasing bone turnover and decreasing bone density. His suggestion was based on Harold Frost's investigation.[12] Frost found a direct correlation between the severity of bone corticotomy and/or osteotomy and the magnitude of the physiologic bone healing response, leading to accelerated bone turnover at the surgical site. This was called “Regional Acceleratory Phenomenon” (RAP). RAP was explained as a transient stage of localized tissue remodeling that resulted in healing of the injured bone, through recruitment of osteoclasts and osteoblasts.
According to Hajji et al.,[3] to resolve crowding in mandibular arch, orthodontic treatment times in patients with corticotomies were 3–4 times shorter compared to those of patients without corticotomies.
Cho et al.[13] in a study conducted on two beagle dogs applied corticotomy intervention on the buccal and lingual side of the alveolar bone. This evaluation showed that rapid orthodontic tooth movement was apparent following the application of orthodontic force after corticotomy.
Another study by Iino et al.[14] on 12 beagle dogs protracted premolars after corticotomy. Their results showed an increase in velocity of orthodontic tooth movement.
Numerous studies have confirmed the usefulness of the corticotomy to accelerate orthodontic tooth movements. However, most studies have been conducted on animals.
There are some differences in bone metabolism rate between species and even between individuals of the same species. This difference can be considered as a confounding factor. Therefore, in this study, we decided to evaluate the effect of buccal corticotomy to accelerate orthodontic tooth movement in human samples. Based on a random manner in each patient, the maxillary canine on one side was considered as the intervention side and the other side as the control side. Thus, the effect of confounding factor such as different turnover rate is eliminated. Our surgery was applied only on buccal cortical plate; therefore, in case of a positive result, we would be able to achieve the desired result by a more conservative procedure.
In another investigation, Aboul-Ela et al.[15] evaluated the rate of tooth movement after application of corticotomy. They concluded that the rate of tooth movement in the first and second months had increased 2 times, and the third and fourth months, 1.6 times comparing to the control side.
Al-Naoum et al.[16] evaluated effect of corticotomy to accelerate orthodontic space closure after first maxillary premolar extraction in thirty patients. Velocity of canine movement in the intervention side in the 1st and 2nd weeks after corticotomy was as 4 times as the control side, and between the 2–4th and 8–12th weeks, it was almost 3 times.
MATERIALS AND METHODS
This study is a clinical trial with IRCT2013082014415N1 registration code. The sample consisted of 15 adult female patients (mean age, 25 years) requiring therapeutic extraction of the first maxillary premolars. These volunteers were selected from patients who referred to the Department of Orthodontics of Isfahan Azad University. Samples with certain systemic diseases, using certain administrated drugs, previous orthodontic treatment, advanced or active periodontal disease, and poor oral hygiene were excluded from the study. This study was performed by using split mouth design method. In a randomized manner, one side of the maxillary arch on which corticotomy was applied was considered as the experimental group, and the other side without surgical intervention was considered as the control group. All patients were completely informed of the procedure and signed an informed consent. Since the split-mouth design was applied, the experimental and control groups were the same and they were completely matched in the terms of age, sex, etc.
All patients were treated with standard fixed appliances, with 0.018 × 0.022 slot brackets (Equilibrium, Dentaurum, Springen, Germany).
To enhance posterior segment anchorage in all patients, strap up was extended to the second molar. The anchorage segment was additionally stabilized by use of a miniscrew on buccal segment between the first and second molar, tying second premolar to the screw.
After initial segmental leveling and alignment, one maxillary quadrant was randomly assigned to have corticotomy procedure. After administration of local anesthesia, by application of a sulcular incision and two vertical releasing incisions, a mucoperiosteal flap was reflected in the buccal side from distal surface of the canine to the mesial surface of the second premolar. Two millimeters of marginal crestal bone held intact and using a high-speed drill and a number 2 round bur (1 mm in diameter) vertical groove with depth of 0.5–1 mm and a length of approximately 1 cm in the distal surface of canine tooth and a similiar groove in the mesial surface of the second premolar were created only on cortical bone. In addition, 10 small holes in the cortical bone overlying the first premolar were created. The surgical site was rinsed, and the flap was repositioned and sutured. The opposite side served as the control side, without flaps or corticotomies.
At the same session, the first maxillary premolars in both sides were extracted.
Two weeks after surgery, the patients were met to install fixed sectional canine retractors on both sides. Using 0.016 × 0.016 steel wires (Orthotechnology, Florida, USA), for both sides, similar canine retractors (simple open vertical loop) were made and installed. Force magnitude of retractors was checked (in situ) and calibrated with a gram force gauge (Correx, Dentaurum, Springen, Germany) to deliver approximately 200 g force in each side every 2 weeks and as long as canines reached the vicinity of the second premolars. These retractors were activated in each session (due to increased velocity of tooth movement almost 2–3 times after corticotomy 2 times activations per month seems logical).[17] Using a compass and a caliper, the distance between the canine and second premolar was measured on each side, and the traveled distance was divided by the time of treatment, to specify the rate of tooth movement. Then, by comparing complete canine retraction time and by determination of movement velocity, the influence of this technique on reducing the treatment time was assessed. These measurements were considered an indicator of canine retraction speed taking into account that the anchor segment was almost immobilized.
Statistical analysis was conducted using SPSS version 20. Kolmogorov–Smirnov and paired-sample t-tests were employed to evaluate inter-group differences (with α set at 0.05).
RESULTS
According to evaluation of velocity of tooth movement in two groups in the 1st, 2nd, 3rd, and 4th months and whole assessment time (because the average time to complete canine retraction was about 4 months, the total duration of the study was 4 months and comparing the monthly rate of tooth movement was included in the study to find out how long the effect of corticotomy in accelerating tooth movement is statistically significant), the following results were observed.
Average velocity of maxillary canine retraction in the 1st month in the experimental group was significantly higher than the control group (2.2 mm/month vs. 1 mm/month), (P < 0.0001) [Table 1].
Table 1.
Average velocity of tooth movement in two groups in the first, second, third, and fourth months
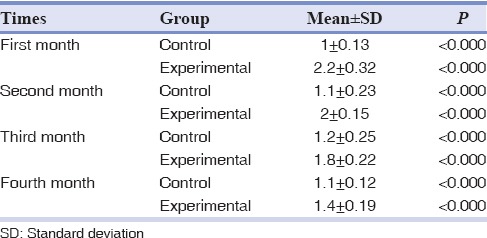
Average velocity of maxillary canine retraction in the 2nd month in the experimental group was significantly higher than the control group (2 mm/month vs. 1.1 mm per month) and was significantly higher (P < 0.001) [Table 1].
Average velocity of maxillary canine retraction in the 3rd month in the experimental group was significantly higher than the control group (1.8 mm/month vs. 1.2 mm/month) (P < 0.001) [Table 1].
Average velocity of maxillary canine retraction in the 4th month in the experimental group was significantly higher than the control group (1.4 mm/month vs. 1.1 mm/month) (P < 0.001) [Table 1].
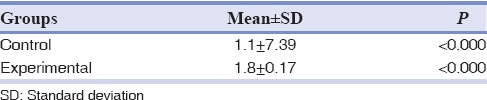
The measurements showed a significant difference in the velocity of tooth movement between the experimental and the control groups. (Averages of 1.8 mm/month vs. 1.1 mm/month) [Table 2].
Table 2.
Average velocity of tooth movement in control and experimental group
DISCUSSION
This randomized controlled trial was established to investigate the effect of buccal corticotomy on tooth movement in comparison with the conventional orthodontic technique. It was assumed that if corticotomy be applied only on the buccal side, instead of both the buccal and palatal cortical plates, orthodontic forces in conjunction with the corticotomy procedures will still produce substantially greater maxillary canine movement velocity than orthodontic forces alone.
Compared to osteotomy and two-sided corticotomy, this single-side approach creates less discomfort for the patient, and the surgeon also spends less treatment time. The results of this study show that buccal corticotomy alone could accelerate orthodontic canine movement significantly.
In one study, Aboul-Ela et al.[15] concluded that the rate of tooth movement in the 1st and 2nd months accelerated by 2 times and in the 3rd month increased by 1.6 times which was in agree with our findings but in the 4th month, the velocity of tooth movement accelerated by 1.04 times, which was not statistically significant, and was not in agree with the present study. The reason may be that although in the study of Aboul-Ela et al.,[15] as with the present study, corticotomy was applied only on the buccal cortex; however, unlike the recent study, they did not make a vertical incision in the cortical bone and just made some perforations on the cortical bone. Probably, it can explain the shorter duration of the local acceleration phenomenon in that study. This issue is in agree with Harold Frost that observed a direct correlation between the amount of injury with the intensity of physiological healing response, which he named regional accelerated phenomena (RAP). RAP does not offers new healing processes but rather explains the acceleration of normal healing events; the greater the insult, the more accelerated regional healing response.
The findings of this study are consistent with the findings of Iino et al.,[14] Wilcko et al.,[2] and Ren et al.,[18] which have reported the increase rate of corticotomy speed by 2–3 times.
The results of the study by Lee et al.[19] showed that on contrary to the initial hypothesis, based on the need to create a separate block of bone to accelerate orthodontic tooth movement, corticotomy without need for creating blocks of bone, and only reliance on regional acceleration phenomenon, increases the rate of tooth movement,. Moreover, they stated that even orthodontic tooth movement alone can initiate local acceleration phenomenon, which corticotomy will intensify the phenomenon. Since orthodontic tooth movement was done on both sides, the difference in velocity between the two sides is merely related to the role of corticotomy, and this does not prejudice the results of our study.
In a recent investigation, Aboul-Ela et al.[15] found no significant molar anchorage loss during canine retraction on either the corticotomy or the control side. They had used mini implants for anchorage on both sides.
Cho et al.[13] have reported an acceleration of speed as 4 times in upper jaw of two beagle dogs. The reason for this more acceleration than the recent study can be referring to two definite differences existing between the two studies. First, they had employed animal models. It has been found that dog bone in terms of composition and density is most similar to human bone. However, in terms of metabolism and iliac bone formation rate, the speed is 2 times faster than humans. Further, the duration of a single cycle remodeling for dog is almost 42% faster than humans.
Second, they had done corticotomy on both the buccal and lingual sides, which may be responsible for more accelerating of tooth movement.
Our findings are consistent with the Sanjideh et al.[20] research which represents an 85% greater amount of tooth movement in the corticotomy sides than the control ones.
Ferguson[21] in a human study have reported that using corticotomy, mandibular crowding has been resolved four times faster. The more acceleration in tooth movement compared to our study probably relates to the type of tooth movement examined in the two studies. In that study, no tooth has been extracted, so dominant type of tooth movement has been tipping, which we know that compared with bodily tooth movement, predominate type of tooth movement in our study, can be done with more ease and speed.
Although corticotomy significantly accelerates the rate of orthodontic tooth movement, significant reductions in treatment time of comprehensive orthodontic treatment are questionable. There are some case reports that claim comprehensive orthodontic treatment can be completed in 4–9 months by application of a single stage corticotomy, whereas conventional orthodontics takes 1.5–2.5 years.[2,22] Based on the previous longitudinal experimental studies,[13,14] duration of increased local acceleration phenomenon after corticotomy is between 1 and 4 months. Hence, it is difficult to realize how a single corticotomy can accelerate the treatment time by 14–21 months.
It is advisable to make some modifications in future clinical trials on corticotomy-assisted orthodontics to obtain more information about this useful adjunctive procedure. First, to evaluate this intervention in a longer treatment time to find out the influence of this technique on comprehensive orthodontic treatment time; second, to evaluate the effect of corticotomy on anchorage preservation or even anchorage loss; third, by use of a split mouth design, this technique can be compared with some claimed less invasive adjuncts such as low-level laser corticotomy and micro-osteoperforations; fourth, to establish an absolute stationary anchorage for posterior segments, for example, by use of mini plates; to better evaluation of the role of corticotomy on anterior segment retraction.
CONCLUSION
Selective alveolar corticotomy only on the buccal maxillary cortex can significantly increase the rate of orthodontic canine retraction, and it is probably a useful adjunct to shorten treatment time. It is perhaps due to regional accelerated phenomenon that accrue after surgical procedure and results in increased bone turn over and decrease bone density
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Burstone CJ, Tanne K. Biomechanical basis of tooth movement. Nihon Kyosei Shika Gakkai Zasshi. 1986;45:541–51. [PubMed] [Google Scholar]
- 2.Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19. [PubMed] [Google Scholar]
- 3.Hajji SS, Ferguson DJ, Miley DD, Wilcko WM, Wilcko MT. The influence of accelerated osteogenic response on mandibular decrowding. J Dent Res. 2001;80:180. [Google Scholar]
- 4.Düker J. Experimental animal research into segmental alveolar movement after corticotomy. J Maxillofac Surg. 1975;3:81–4. doi: 10.1016/s0301-0503(75)80022-1. [DOI] [PubMed] [Google Scholar]
- 5.Mostafa YA, Mohamed Salah Fayed M, Mehanni S, ElBokle NN, Heider AM. Comparison of corticotomy-facilitated vs standard tooth-movement techniques in dogs with miniscrews as anchor units. Am J Orthod Dentofacial Orthop. 2009;136:570–7. doi: 10.1016/j.ajodo.2007.10.052. [DOI] [PubMed] [Google Scholar]
- 6.Eells JT, Henry MM, Summerfelt P, Wong-Riley MT, Buchmann EV, Kane M, et al. Therapeutic photobiomodulation for methanol-induced retinal toxicity. Proc Natl Acad Sci U S A. 2003;100:3439–44. doi: 10.1073/pnas.0534746100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Guilford SH. Orthodontia: Or Malposition of the Human Teeth; its Prevention and Remedy. 3rd ed. Philadelphia: Davis; 1898. [Google Scholar]
- 8.Kole H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol. 1959;12:413–20. doi: 10.1016/0030-4220(59)90051-9. [DOI] [PubMed] [Google Scholar]
- 9.Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontic decrowding with alveolar augmentation: Case report. World J Orthod. 2003;4:197–205. [Google Scholar]
- 10.Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated osteogenic orthodontics technique: A 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J Oral Maxillofac Surg. 2009;67:2149–59. doi: 10.1016/j.joms.2009.04.095. [DOI] [PubMed] [Google Scholar]
- 11.Wilcko MT, William M, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: A synthesis of scientific perspectives. Semin Orthod. 2008;14:305–16. [Google Scholar]
- 12.Frost HM. The biology of fracture healing. An overview for clinicians. Part II. Clin Orthop Relat Res. 1989;248:294–309. [PubMed] [Google Scholar]
- 13.Cho KW, Cho SW, Oh CO, Ryu YK, Ohshima H, Jung HS. The effect of cortical activation on orthodontic tooth movement. Oral Dis. 2007;13:314–9. doi: 10.1111/j.1601-0825.2006.01286.x. [DOI] [PubMed] [Google Scholar]
- 14.Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop. 2007;131:448.e1–8. doi: 10.1016/j.ajodo.2006.08.014. [DOI] [PubMed] [Google Scholar]
- 15.Aboul-Ela SM, El-Beialy AR, El-Sayed KM, Selim EM, El-Mangoury NH, Mostafa YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthod Dentofacial Orthop. 2011;139:252–9. doi: 10.1016/j.ajodo.2009.04.028. [DOI] [PubMed] [Google Scholar]
- 16.Al-Naoum F, Hajeer MY, Al-Jundi A. Does alveolar corticotomy accelerate orthodontic tooth movement when retracting upper canines? A split-mouth design randomized controlled trial. J Oral Maxillofac Surg. 2014;72:1880–9. doi: 10.1016/j.joms.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 17.Kim SJ, Park YG, Kang SG. Effects of Corticision on paradental remodeling in orthodontic tooth movement. Angle Orthod. 2009;79:284–91. doi: 10.2319/020308-60.1. [DOI] [PubMed] [Google Scholar]
- 18.Ren A, Lv T, Kang N, Zhao B, Chen Y, Bai D. Rapid orthodontic tooth movement aided by alveolar surgery in beagles. Am J Orthod Dentofacial Orthop. 2007;131:160e.1–10. doi: 10.1016/j.ajodo.2006.05.029. [DOI] [PubMed] [Google Scholar]
- 19.Lee W, Karapetyan G, Moats R, Yamashita DD, Moon HB, Ferguson DJ, et al. Corticotomy-/osteotomy-assisted tooth movement microCTs differ. J Dent Res. 2008;87:861–7. doi: 10.1177/154405910808700904. [DOI] [PubMed] [Google Scholar]
- 20.Sanjideh PA, Rossouw PE, Campbell PM, Opperman LA, Buschang PH. Tooth movements in foxhounds after one or two alveolar corticotomies. Eur J Orthod. 2010;32:106–13. doi: 10.1093/ejo/cjp070. [DOI] [PubMed] [Google Scholar]
- 21.Ferguson D. Rapid orthodontics following alveolar decortication and grafting. J Taiwan Orthod Soc. 2009;2:31–47. [Google Scholar]
- 22.Hosl E, Baldauf A. Mechanical and Biological Basics in Orthodontic Therapy. Heidelberg: Hüthig Buch Verlag; 1991. pp. 207–26. [Google Scholar]