

Abstract
Background:
The purpose of this study was to investigate of radiographic pattern and relative frequency of idiopathic osteosclerosis (IO) and condensing osteitis (CO) in panoramic radiographs.
Materials and Methods:
Totally 411 panoramic radiographies were randomly selected from patients referred to Radiology Department of Faculty of Dentistry, Tabriz University of Medical Sciences. Descriptive characteristics of radiopacities, including shape, border, localization, and dental relationship, were recorded. The Chi-squared test was used.
Results:
IO was detected in 31 (7.5%) patients and 22 (68.8%) lesions had exact border while their shape was mostly irregular. About 17 (53.1%) lesions were apical, and 13 (40.6%) lesions had no relation to the teeth. The most involved teeth were the second premolar (28.1%) and first molar (25%). Moreover, CO was detected in 32 (7.8%) patients. 17 (53.1%) lesions had an ill-defined border, and their shape was mostly irregular (65.6%) with ill-defined border. Around 18 (56.3%) lesions were apical, and 11 (34.4) lesions were apical and interradicular. The most involved teeth were the second premolar (59.4%) and the first molar (21.9%).
Conclusion:
The results demonstrated that relative frequency of IO in the selected population was 7.5% and for CO, it was 7.8%.
Key Words: Condensing osteitis, frequency, idiopathic osteosclerosis
INTRODUCTION
Idiopathic osteosclerosis (IO) is known as the region of enlarged bone production in the jaw, and its shape could be round, elliptical, or irregular in shape.[1,2,3] These lesions recognized as developing intraosseous anatomic variations[4] and should be categorized distinctly from the cases due to inflammatory source or systemic disease.[5,6] These asymptomatic lesions are mostly revealed as causal results on radiographs derived for other reasons[4] on radiographic evaluation, IO may be identified in different sizes in diameter (2 or 3 mm to 1 or 2 cm)[2,7] or the lesions may be very large, almost the whole height of the body of the jaw.[8,9] They may happen at root apexes, among the roots, or in a distinct site away from the teeth, first in the premolar/molar region and with a preference for the mandibular arch. Similar radiopaque region may occur in the periapical areas of teeth with nonessential or much inflamed pulps; these lesions most likely characterize a reaction to a low-grade inflammatory inducer. Such passive region nominated as condensing osteitis (CO) or focal chronic sclerosing osteomyelitis and should not be incorporated underdetermine of IO.[10,8]
The aim of this study was to investigate the frequency of IO and CO lesions in the Tabriz patient population with respect to age, sex, shape, localization, and dental relationship.
MATERIALS AND METHODS
This study designed as descriptive study composed of 411 panoramic radiography of patients who referred to the Oral and Maxillofacial Radiology Service of Dentistry Faculty, Tabriz University of Medical. All radiographs achieved by an orthopantomography device (planmeca proline CC 2002, 60–80 kVp, 8–10 mA, 12.8 s exposure time, Helsinki, Finland) by X-ray technician who had a minimum working skill of 5 years. Then, 6-inch green-sensitive panoramic film (Medical, Konica Co., Japan) was used to take radiography.
All images were examined by a specialist in oral and maxillofacial radiology.
Lesions determined as CO if it linked with chronic inflammation. Mostly, these lesions enclosed the apex of teeth with deep caries or large restorations. But, the lesions did not display any clear link to inflammation, well determined, and were not ruled out by the cases listed above were recognized as IO. The following radiopacities were specially omitted:[2,3,5]
Distinctive mixed radiopaque-radiolucent areas of periapical cemented dysplasia and other benign fibro-osseous lesions of periodontal ligament origin
Increased thickening of the lamina dura nearby teeth that presented clear malposition or that worked as abutment for fixed bridges or partial dentures
Obviously recognizable remnants of deciduous or permanent teeth
Radiopacities understood as tori or exostoses
Solitary radiopacities seen in edentulous areas, since these might have been excessively ossified surgical sites
Patients with Gardner's syndrome, colon familial polyposis, and other diseases with the bone metabolic disorder.
The shape of the lesions was categorized as either round or irregular.
The lesions are located first as mandibular or maxillary, next more by region of the jaw: Incisive, canine, canine-premolar, premolar, premolar-molar, or molar.
Radiopaque areas which were depicted as IO and CO that was classified by criteria of Geist and Katz [Figure 1a–e]:[2]
Figure 1.
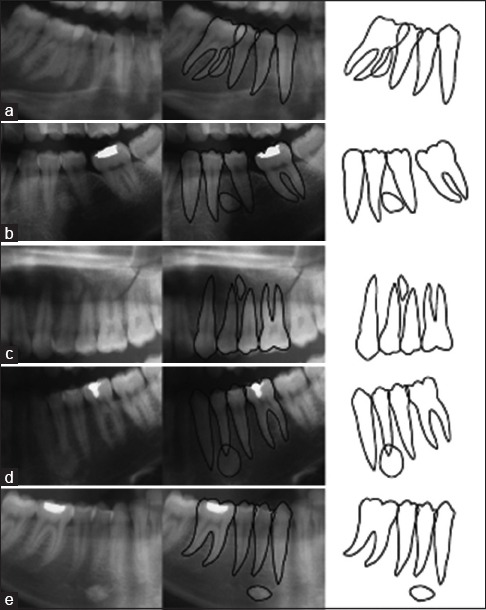
Radiographic appearance of the osteosclerotic lesions which were detected in (a) interradicular, (b) interradicular and separate, (c) apical interradicular, (d) apical, (e) separate localization.
Interradicular: If the sclerotic area was confined between the roots and interrelated with the adjacent teeths' lamina dura
Interradicular and separate: If the sclerotic area was confined between the roots and not interrelated with the adjacent teeths' lamina dura
Apical and interradicular: If the radiopacities were at the apices and showed significant extension between the roots
Apical: If the lesions were located around the apices of the roots
Separate: If the masses were located apically and clearly separated from the teeth and lamina dura.
The results were evaluated by SPSS 11.5 program (SPSS Inc., Chicago). Differences between distributions of lesions were determined by the Chi-squared test when ranked by gender, age, shape, localization, and relation to teeth. A P < 0.05 was considered statistically significant.
RESULTS
This study performed on panoramic radiographs of 411 patients (226 females, 185 males), aged 6–95 years (mean age: 33.8 ± 13.66).
There were 32 IO lesions in 31 (7.5%) subjects which mean age was 30.52 years, and other patients were 34.06 (P > 0.05). These 31 consisted of 23 females and eight males (P < 0.05).
Moreover, 32 CO lesions in 32 subjects (7.8%) were determined that mean age was 34.59 years and in other was 33.73 years (P > 0.05). These 32 patients contained 15 females and 17 males (P > 0.05).
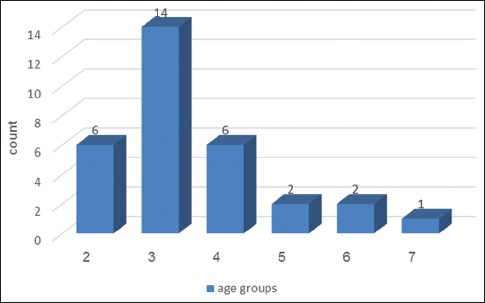
Figures 2 and 3 showed the age distribution of patient in different decades of life that had IO and CO lesions. According to the results, the frequency of IO lesions was higher in the third, second, and fourth decades of life, respectively, than in other periods and for CO lesions were more in the fourth, second, and fifth decade of life.
Figure 2.
Age distribution of patient in different decades of life with idiopathic osteosclerosis lesion.
Figure 3.

Age distribution of patient in different decades of life with condensing osteitis lesion.
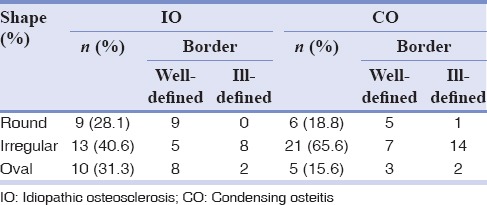
The distributions of IO and CO with respect to shape and border were given in Table 1. In the IO lesion, the most shape was irregular form, and Pearson Chi-square analysis showed this difference was statistically significant (P = 0.006). For CO lesions, the most shape was irregular. From 32 lesions and difference was not statistically significant (P = 0.078).
Table 1.
Distribution of idiopathic osteosclerosis and condensing osteitis with respect to shape and border
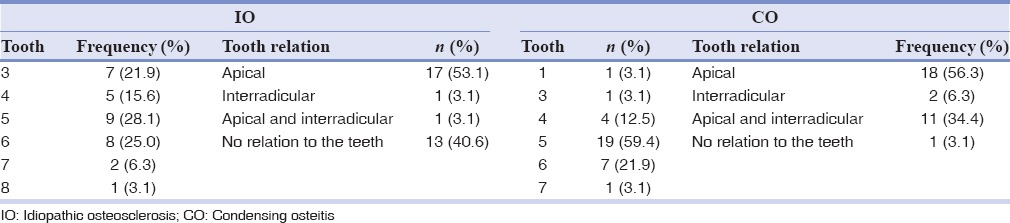
The distributions of IO and CO with respect to localization and relationship to teeth of lesion are showed in Table 2. For IO lesions, the most involved tooth was second premolar (28.1%) and first molar (25%). Of the 32 IO lesions, thirty subjects found in mandibular and two subjects in maxillary of fourth and sixth teeth. In addition, the most lesions were apical and from 40.6% of lesion that was separate from teeth, mean of distance was 15.64 mm (2–30 mm). But for CO lesions, the most involved tooth was the second premolar (59.4%) and the first molar (21.9%). Among the 32 CO lesions, 31 cases related to mandibular and only in maxillary of the first tooth. On the other hand, the most lesion was apical and then apical and interradicular. Moreover, just one CO found that had 5 mm distance from the tooth.
Table 2.
The distribution of idiopathic osteosclerosis and condensing osteitis lesions with respect to tooth and tooth relation
DISCUSSION
Many of earlier studies investigated the frequency of IO and CO lesions.[11,12,13,14,15,16] In the present study, of 411 panoramic radiographic the frequency of IO lesions was 7.5% and CO was 7.8%. In the previous literature, frequency of radiopaque lesions reported as ranges from 3.3% to 31.0%.[7,17,18] Geist and Katz detected 5.4% frequency of IO in 1921 full-mouth intraoral radiographic investigations[2] and IO frequency of 1047 panoramaric radiographs was 6.1% which was two-third of 1203 panoramaric radiographs in Japanese dental outpatients.[5,19] Lu et al. in 2003 reported the frequency of IO in South Taiwan population as 9.43% that probably due to genetic factors and breeding the lesion was seen more in the East population.[20] But this range was two times higher than other studies.[3,10,11]
On the other hand, Eliasson et al. reported the frequency of CO in 1149 periapical radiographs to 2%[21] while in the other study, with little sample size, it is found 6% CO.[22] The difference between the results obtained in this study could be evaluated by several aspects with previous studies. First, the study was performed on panoramic radiographs and due to the difference in image quality, especially in the anterior region, there were not comparable by results of studies on periapical radiographs. The results of other studies have reported a higher prevalence of radiopaque IO and CO lesions.[2,11,10,22,23] The second reason for the difference between the results was related to different criteria. For example, in this study radiopaque of edentulous areas was omitted because it is probably formed after tooth extraction. Moreover, other factors such as differences of genetic and diet may also be effective at the difference frequency. In the present study, the frequency of IO was higher in females and the incidence CO had no differences between women and men. But according to the Miloglu et al., the frequency of IO and CO was higher in Turkish women than men.[24] In addition, Geist and Katz and McDonnell, who determined women to men ratio of 1.5:1 and 2:1, respectively.[6] Similarly, Avramidou et al. identified that female patients have more radiopaque lesion than male in a sample of Greek patients.[25] However, other study showed no difference between the incidence in female and male.[5,19] In the present study, the frequency of CO increased with age until the fourth decade of life that related to tooth decay. But in this study, a decrease of CO in fifth and higher decade of life could be due to loss of tooth decay in older age that in this study edentulous sites were not examined. On the other hand, the frequency of IO was high in the third decade of life. The frequency of both radiopaque was more common in mandibular that is consistent with previous studies.[3,5,10,19] This case could be the result of taking panoramic radiographs because the image of anatomic structures in mandibular was not clear than maxillary and be less superimposition. In addition, differences in the incidence of CO and IO were related to anatomy of jaw bone and blood flow in jaw, although the cause of the lesions is unknown. In this study, IO and CO were more in premolar and then in a molar. The result of Miloglu et al. showed that IO was more in premolar and CO in a molar.[24] The reason of high frequency of IO in premolar was attributed to remain of premolar root and replacement with bone sclerotic. A histological investigation by Henrikson clarified the existence of bone sclerotic at the site of IO.[26] Further, in this study, the most lesions were periapical which matched by Geist and Katz.[2] While in another study, the most lesions had no relationship by teeth.[19] In addition, most of the lesions were irregular and spherical radiopaque with well-defined border that was similar to other results.[2,3]
CONCLUSION
In the light of these findings, we could demonstrate that relative frequency of IO in Iranian population is 7.5% and for CO, it is 7.8%. IO was more prevalent in women in mandibular and in the third decade of life, but CO lesion had no difference between women and men. Moreover, CO similar to IO was more in mandibular and showed high rate in the fourth decade of life.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Halse A, Molven O. Idiopathic osteosclerosis of the jaws followed through a period of 20-27 years. Int Endod J. 2002;35:747–51. doi: 10.1046/j.1365-2591.2002.00561.x. [DOI] [PubMed] [Google Scholar]
- 2.Geist JR, Katz JO. The frequency and distribution of idiopathic osteosclerosis. Oral Surg Oral Med Oral Pathol. 1990;69:388–93. doi: 10.1016/0030-4220(90)90307-e. [DOI] [PubMed] [Google Scholar]
- 3.Petrikowski CG, Peters E. Longitudinal radiographic assessment of dense bone islands of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:627–34. doi: 10.1016/s1079-2104(97)90131-1. [DOI] [PubMed] [Google Scholar]
- 4.Bsoul SA, Alborz S, Terezhalmy GT, Moore WS. Idiopathic osteosclerosis (enostosis, dense bone silands, focal periapical osteopetrosis) Quintessence Int. 2004;35:590–1. [PubMed] [Google Scholar]
- 5.Yonetsu K, Yuasa K, Kanda S. Idiopathic osteosclerosis of the jaws: Panoramic radiographic and computed tomographic findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:517–21. doi: 10.1016/s1079-2104(97)90156-6. [DOI] [PubMed] [Google Scholar]
- 6.McDonnell D. Dense bone island. A review of 107 patients. Oral Surg Oral Med Oral Pathol. 1993;76:124–8. doi: 10.1016/0030-4220(93)90307-p. [DOI] [PubMed] [Google Scholar]
- 7.Austin BW, Moule AJ. A comparative study of the prevalence of mandibular osteosclerosis in patients of Asiatic and Caucasian origin. Aust Dent J. 1984;29:36–43. doi: 10.1111/j.1834-7819.1984.tb04541.x. [DOI] [PubMed] [Google Scholar]
- 8.MacDonald-Jankowski DS. Idiopathic osteosclerosis in the jaws of Britons and of the Hong Kong Chinese: Radiology and systematic review. Dentomaxillofac Radiol. 1999;28:357–63. doi: 10.1038/sj/dmfr/4600485. [DOI] [PubMed] [Google Scholar]
- 9.Kawai T, Murakami S, Kishino M, Sakuda M. Gigantic dense bone island of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82:108–15. doi: 10.1016/s1079-2104(96)80387-8. [DOI] [PubMed] [Google Scholar]
- 10.Williams TP, Brooks SL. A longitudinal study of idiopathic osteosclerosis and condensing osteitis. Dentomaxillofac Radiol. 1998;27:275–8. doi: 10.1038/sj/dmfr/4600362. [DOI] [PubMed] [Google Scholar]
- 11.Moshfeghi M, Azimi F, Anvari M. Radiologic assessment and frequency of idiopathic osteosclerosis of jawbones: An interpopulation comparison. Acta Radiol. 2014;55:1239–44. doi: 10.1177/0284185113515210. [DOI] [PubMed] [Google Scholar]
- 12.Chen CH, Wang CK, Lin LM, Huang YD, Geist JR, Chen YK. Retrospective comparison of the frequency, distribution, and radiographic features of osteosclerosis of the jaws between Taiwanese and American cohorts using cone-beam computed tomography. Oral Radiol. 2014;30:53–63. [Google Scholar]
- 13.Razavi SM, Kiani S, Khalesi S. Periapical lesions: A review of clinical, radiographic, and histopathologic. Avicenna J Dent Res. 2014;7:e19435. [Google Scholar]
- 14.Alkurt MT, Sadik E, Peker İ. Prevalence and distribution of idiopathic osteosclerosis on patients attending a dental school- J Istanbul Univ Fac Dent. 2014;48:29–34. [Google Scholar]
- 15.Kumar V. Different radiographic modalities used for detection of common periodontal and periapical lesions encountered in routine dental practice. Oral Hyg Health. 2014;2:163. [Google Scholar]
- 16.Yeh HW, Chen CY, Chen PH, Chiang MT, Chiu KC, Chung MP, et al. Frequency and distribution of mandibular condensing osteitis lesions in a Taiwanese population. J Dent Sci. 2015;10:291–295. [Google Scholar]
- 17.Farman AG, de V Joubert JJ, Nortjé CJ. Focal osteosclerosis and apical periodontal pathoses in “European” and Cape coloured dental outpatients. Int J Oral Surg. 1978;7:549–57. doi: 10.1016/s0300-9785(78)80072-6. [DOI] [PubMed] [Google Scholar]
- 18.Alattar MM, Baughman RA, Collett WK. A survey of panoramic radiographs for evaluation of normal and pathologic findings. Oral Surg Oral Med Oral Pathol. 1980;50:472–8. doi: 10.1016/s0030-4220(80)80017-x. [DOI] [PubMed] [Google Scholar]
- 19.Kawai T, Hirakuma H, Murakami S, Fuchihata H. Radiographic investigation of idiopathic osteosclerosis of the jaws in Japanese dental outpatients. Oral Surg Oral Med Oral Pathol. 1992;74:237–42. doi: 10.1016/0030-4220(92)90389-8. [DOI] [PubMed] [Google Scholar]
- 20.Lu P, Chuang F, Roan R, Chen J. 81st General Session of the International Association for Dental Research. Program book by Kiyonobu-honma on Oct17. 2014. The prevalence of idiopathic osteosclerosis and condensing ostitis in South Taiwan population. [Google Scholar]
- 21.Eliasson S, Halvarsson C, Ljungheimer C. Periapical condensing osteitis and endodontic treatment. Oral Surg Oral Med Oral Pathol. 1984;57:195–9. doi: 10.1016/0030-4220(84)90211-1. [DOI] [PubMed] [Google Scholar]
- 22.Marmary Y, Kutiner G. A radiographic survey of periapical jawbone lesions. Oral Surg Oral Med Oral Pathol. 1986;61:405–8. doi: 10.1016/0030-4220(86)90427-5. [DOI] [PubMed] [Google Scholar]
- 23.Rohlin M, Akesson L, Hakansson J, Hakansson H, Nasstrom K. Comparison between panoramic and periapical radiography in the diagnosis of periodontal bone loss. Dentomaxillofac Radiol. 1989;18:72–6. doi: 10.1259/dmfr.18.2.2635121. [DOI] [PubMed] [Google Scholar]
- 24.Miloglu O, Yalcin E, Buyukkurt M-C, Acemoglu H. The frequency and characteristics of idiopathic osteosclerosis and condensing osteitis lesions in a Turkish patient population. Med Oral Patol Oral Cir Bucal. 2009;14:e640–5. doi: 10.4317/medoral.14.e640. [DOI] [PubMed] [Google Scholar]
- 25.Avramidou FM, Markou E, Lambrianidis T. Cross-sectional study of the radiographic appearance of radiopaque lesions of the jawbones in a sample of Greek dental patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:e38–43. doi: 10.1016/j.tripleo.2008.04.020. [DOI] [PubMed] [Google Scholar]
- 26.Henrikson CO. Radiopaque areas in human jaws. A report of 18 cases. Scand J Dent Res. 1963;71:373–9. [Google Scholar]