

Abstract
Background:
Direct observation cannot detect caries under restorations; therefore, the aim of this study was to compare the accuracy of radiographs and DIAGNOdent in detecting caries under restorations in primary teeth using histologic evaluation.
Materials and Methods:
A total of 74 previously extracted primary molars (37 with occlusal caries and 37 without caries) were used. Class 1 cavity preparations were made on each tooth by a single clinician and then the preparations were filled with composite resin. The accuracy of radiographs and DIAGNOdent in detecting caries was compared using histologic evaluation. The data were analyzed by SPSS version 21 using Chi-square, Mc Namara statistical tests and receiver operating characteristic curve. The significance was set at 0.05.
Results:
The sensitivity and specificity for DIAGNOdent were 70.97 and 83.72, respectively. Few false negative results were observed, and the positive predictive value was high (+PV = 75.9) and the area under curve was more than 0.70 therefore making DIAGNOdenta great method for detecting caries (P = 0.0001). Two observers evaluated the radiographs and both observers had low sensitivity ( first observer: 48.39) (second observer: 51.61) and high specificity (both observers: 79.07). The +PV was lower than DIAGNOdent and the area under curve for both observers was less than 0.70. However, the difference between the two methods was not significant.
Conclusion:
DIAGNOdent showed a greater accuracy in detecting secondary caries under primary molar restorations, compared to radiographs. Although DIAGNOdent is an effective method for detecting caries under composite restorations, it is better to be used as an adjunctive method alongside other detecting procedures.
Key Words: Careis, diagnosis, laser fluorescence, radiography
INTRODUCTION
Today dental caries are one of the most common global health problems. Detecting carious lesions under restorative materials is complicated because there can be no direct observation of dental tissue under the restoration;[1] Therefore, radiographic evaluation is implemented to achieve this goal. Various factors such as the clinician's ability, lesion's size,[1,2] location of the carious lesion,[3] and exposure characteristics[4] can affect the radiographic interpretation. Porosity of composite restorations can also cause more false positive results.[5] On the other hand taking radiographs in small children is accompanied with other complications such as child's cooperation;[6] thus the needs for a device which can detect carious lesions with high accuracy without needing an expert operator is obvious.[7] DIAGNOdent might be able to overcome this issue. The absence of harmful radiation is another benefit of DIAGNOdent. Various methods have been used to evaluate caries under restorations such as Digital radiography, analog radiography, and laser fluorescence.[8,9] DIAGNOdent is a diagnostic tool based on laser fluorescence which measures the difference between the fluorescence of normal and carious dental tissue. DIAGNOdent gives each tissue a different score thus, reducing human error.[10,11] Several studies have been carried out regarding accuracy and capability of these devices in detecting carious lesions. Many of these studies reported higher accuracy for DIAGNOdent comparing to radiographic evaluation,[11,12,13,14,15] although only one study declared this difference significant.[11] In one study, the ability of detecting primary caries was the same for DIAGNOdent and radiographic evaluation.[16] Some studies compared the accuracy of these two methods in the detection of secondary caries and suggested that DIAGNOdent could be used as an adjunctive diagnostic method.[17,18] To date, limited studies concerning caries detecton under composite restorations have been carried out. One study stated that the lower fluorescence value of composite material compared to dental tissue inhibits false positive diagnosis.[19] The aim of this study was to compare the accuracy of caries detection underclass one composite restorations of primary molars between radiographs and DIAGNOdent with the gold standard (stereo microscope).
MATERIALS AND METHODS
In this laboratory study, 74 extracted primary molars (37 with occlusal caries and 37 without any caries) were stored in thymol saturated saline. The inclusion criteria were (a) presence of occlusal caries or no caries according to the group, (b) no enamel hypoplasia or developmental anomalies, (c) caries not extended into the pulp, (d) no previous restorations, and (e) no previous proximal caries. The samples were mounted in white stone plaster blocks (10 mm × 10 mm × 20 mm) and the plaster ended at the cementodentinal junction. Similar class 1 cavity preparations were made by a single clinician on each tooth. The depth of the preparations was at least 0.5 mm extended from the dentin to the pulp. The occlusal width of the preparations was 1 mm and about 2 mm of the marginal ridges was kept intact. The preparations were made using a straight 0.8 mm fissure bur (Fissure, Tizkavan, Hashtgerd, Iran) and high-speed handpiece (150000 rpm) with air/water spray. After these preparations were made, the residual pulp floor and axial wall caries were untouched. The location of each carious lesion on the occlusal surface was marked. A similar marking was placed on the non-carious teeth to maintain the blindness of the study. Afterward, each preparation was rinsed with air/water spray for 10 s and then dried. The cavities were etched with 35% phosphoric acid (Ultraetch, Ultradent, South Jordan, USA) for 15 s and then rinsed by air/water spray for 30 s. A cotton pellet and air spray were used to dry the cavities so that some dentin moisture remained. Bonding (3M, ESPE singlebond, MN, USA) was applied using a microbrush and then air sprayed for 3 s to reach a monotonous layer. The restorations were cured for 30 s by alight curing machine (Litex E95C, Dentamerica, Taipei, Taiwan) in a way that the light head was placed at the closest distance from the preparation depth. The composite restoration (3M, ESPE single bond, MN, USA, A1 shade) was placed using the multi-layer technique (one layer is placed and cured for 40 s and then the next layer is added in the same way). The restoration was polished first by using a diamond flame-shaped bur and then by a white mullet. The samples were divided into two groups (carious and non-carious). The occlusal surface of each tooth was polished using pumice. The DIAGNOdentdevice (DIAGNOdent pen 290, Kavodental, Biberach, Germany) was first calibrated according to manufacturer's instructions, and the probe was cleaned and the teeth surface was dried. The occlusal probe was selected and placed perpendicular on the marked region, and then the peak score was recorded. This test was performed by an operator in a complete blind fashion. Each tooth was tested twice and the mean score was regarded as the diagnosis. Scores from 0–14 were considered normal and 14–99 were considered carious. A radiograph was obtained for each mounted sample. The X-ray device (Soredex, Min Ray, Tuusula, Finland) was set at mA = 7, Kvp = 70 for 0.016 s. All radiographs were obtained in 1 day. Each radiographic film was fixed on the tube head and the retentive arm length was set so that the tube had a fixed distance from the films. Each sample was exposedfrom the buccal surface. The images were automatically developed and fixed using an automatic processor device (Hope Micromax HXP 90, PA, USA). Each image was observed by two specialist clinicians (a radiologist and a pediatric dentist) and caries were detected. The radiographs were coded beforehand so that the observers were not aware of the caries situation of the teeth. There was no time limit for observing and detecting caries. Caries was defined as a radiolucent region under the restoration, and normal was defined as the lack of this region. This process was repeated after 1 month to evaluate the reliability of the observers. Each sample was cut from the marked spot and an occluso-apical section was obtained. The sections were dyed using (sable-seek Ultradent, South Jordan, USA) to allow caries detection under the stereomicroscope (SMP 200, HP, Palo Alto, CA, USA). According to the manufacturer, the dye was placed for 10 s on the prepared surface then rinsed and dried. The samples were evaluated using an × 10 stereo-microscope by two oral pathologist simultaneously until they reached a single diagnosis. This diagnosis was used as the study's gold standard.
Caries detection by each method was recorded as positive or negative on a special form. Data was analyzed using SPSS 21 software (SPSS Inc., Chicago, IL, USA). Comparison between DIAGNOdent and radiographs was performed using the McNamara test by measuring the area under the receiver operating characteristic (ROC) curve. The Chi-square test was used to compare each method with the gold standard. The significance level set at 0.05. The sensitivity, specificity, predictive value, and likelihood ratio of each method was also evaluated.
RESULTS
Seventy-four primary teeth were evaluated by microscope (histologic), 31 (41.9%) had secondary caries and 43 (58.1%) were normal. Evaluating DIAGNOdent diagnosis compared to the gold standard using Chi-square test showed a significant difference with the gold standard (P < 0.0001) [Table 1]. For the radiographic method, we asked two specialists to detect caries and record them. The results of each observer were compared to the gold standard. The comparisons using Chi-square test showed that both observers' diagnosis was significantly different from the gold standard (P < 0.05). The inter-observer difference was not significant (P = 0.861) and the kappa coefficient was 0.725 [Table 2]. Sensitivity and specificity of DIAGNOdent were 70.97 and 83.72, respectively; the positive predictive value was high (+PV = 75.9) and the area under the ROC curve was bigger than 0.70. Although, radiographic evaluation by the observers had a low sensitivity (observer 1: 48.39, observer 2: 51.61) and a high specificity (observer 1 and 2: 79.07) and also had a lower +PV compared to DIAGNOdent. The ROC curve evaluation showed that the area under the curve was smaller than 0.70 in both observers. According to McNemarstatistic test, radiographic evaluation was also a good method for detecting secondary caries in primary teeth (P < 0.05) [Table 3]. Evaluating the area under the ROC curve showed that DIAGNOdent (AUC = 0.773) didn't differ significantly from the first (AUC = 0.673) and second observer (AUC = 0.653) (P > 0.05). According to the ROC curve area, there was no significant difference between the observers (P = 0.768). Comparing both methods with the gold standard didn't reveal any significant difference [Figure 1].
Table 1.
Distribution of caries detection by DIAGNOdent compared with histological diagnostic criteria
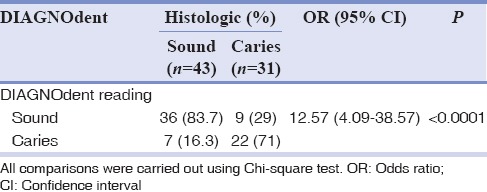
Table 2.
Distribution of caries detection by radiography (with eachobserver) compared with histological diagnostic criteria
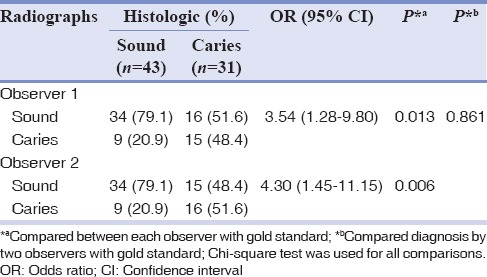
Table 3.
Comparison between DIAGNOdent and radiological (with two observers) diagnostic methods versus standard histological

Figure 1.
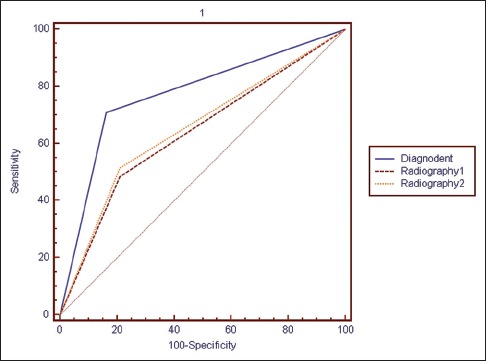
Receiver operating characteristic curve DIAGNOdent and radiological (with two observers) diagnostic methods.
DISCUSSION
Dental caries is one of the most common health problems of the society; therefore, it is important to reach an accurate and early diagnosis.[20] Detecting secondary caries under different restorations is more complicated than detecting primary caries. Different methods such as digital and analog radiography and lasers fluorescense have been used to detect caries under restorations.[8,9,10] Accurate detection of secondary caries in radiographs requires clinical experience therefore a device that doesn't need experience and also has a good accuracy in detecting caries would be favorable.[16] DIAGNOdent is a device based on different fluorescence values of healthy and carious dental tissues. This method doesn't need patient cooperation and doesn't produce ionizing radiation.[11,13,18] The accuracy of this method should be compared with radiographs so that it can be used safely in clinic. Various studies have evaluated the accuracy of DIAGNOdent in different conditions, but there was no study evaluating its accuracy in detecting secondary caries under composite restorations of primary molars. Regarding the difference between the dentin of primary and permanent teeth such as fewer s-shape tubules and more straight tubules in primary teeth, which accelerates caries expansion, and the lower amount of dentin in primary teeth, it is expected that there is a difference between the fluorescence in primary and permanent tooth tissues.[21,22,23] We compared the sensitivity and specificity of DIAGNOdent and analog radiographs. The results showed that both parameters were higher in DIAGNOdent but the difference was not significant. DIAGNOdent also had higher positive and negative predictive values (−PV) compared to radiographs. These findings along with the higher sensitivity and specificity of DIAGNOdent prove that it has a better potential to detect secondary caries under composite restorations of primary molars. On the other hand, the area under the ROC curve for DIAGNOdent was more than 70% which was higher than radiographs and shows the better performance of DIAGNOdent compared to radiographs although the difference was not statistically significant. DIAGNOdent showed a higher positive likelihood ratio (+LR) compared to radiographs, which means higher sensitivity and less false positive results while the negative likelihood ratio was lower in DIAGNOdent, which means fewer false negative results and a higher specificity. DIAGNOdent has a high repeatability[10,23] which is a superior feature compared to direct observation and bite-wing radiographs.[18] Laboratory studies have proven the efficiency of DIAGNOdent but clinical results can be affected by saliva, temperature changes, the presence of extrinsic stains on teeth and the edge of restorations. Polishing the tooth surface with pumice is suggested before using DIAGNOdent to overcome some these limitations.[19]
An in vitro study showed that tooth-storing environments could affect the amount of the tissue fluorescence.[24] We used thymol-saturated saline in our study to store the extracted teeth. This environment can affect the fluorescent features of tooth tissues; therefore caution is advised in interpreting the results of this study.
Sridhar et al.,[25] Diniz et al.,[26] and Pourhashemi et al.[27] showed that DIAGNOdent performs better than radiographs for detecting primary occlusal caries in permanent teeth, which is similar to our results, except that we evaluated secondary caries under composite restorations.
Attril and Ashley,[14] Anttonen et al.,[15] Virajsilp et al.,[13] and Mepparambath et al.[28] reported a higher accuracy for DIAGNOdent in detecting primary caries in deciduous teeth compared to clinical examination and radiographs which is similar to our results, except that the mentioned studies evaluated primary caries.
Kavvadia and Lagouvardos[16] concluded that DIAGNOdent is very reliable in detecting occlusal caries of primary teeth and has the same efficiency of observational and radiographic methods. Our study showed no significant difference between the efficiency of DIAGNOdent and radiographs.
This study showed no significant difference between DIAGNOdent and radiographs in caries detecting accuracy, while Shi et al.[11] stated that caries detecting accuracy of DIAGNOdent was significantly higher than radiographs for non-restored permanent premolars and molars. This difference between the results could be due to the difference between the samples (permanent premolars and molars instead of primary molars, primary caries instead of secondary caries).
Bamzahim et al.[17] compared the accuracy of DIAGNOdent and radiographs in detecting secondary caries under amalgam restorations of primary teeth and reported similar results to our study.
Our study showed a higher sensitivity and specificity for DIAGNOdent compared to radiographs while, Bamzahim et al.[17] reported a lower sensitivity and specificity for DIAGNOdent compared to radiographs in detecting secondary caries under amalgam restorations. The possible cause for this different result could be the presence of amalgam instead of composite. Amalgam creates a better contrast between the restoration and caries on the radiograph, which improves the diagnosis. Amalgam can also affect the detecting accuracy of fluorescent laser.
The result of our study was similar to the results of Kositbowornchai et al.[5] who had compared the accuracy of DIAGNOdent and digital radiographs for detecting caries under third molar composite restorations. Our study showed that DIAGNOdent had low false negative and false positive results, which was also similar to the results of Kositbowornchai et al.[5] The use of DIAGNOdent as a complementary method for detecting caries is suggested in the studies of Akbari et al.,[29] Lussi et al.,[30] Rodrigues et al.,[18] and Huth et al.[31]
Regarding the difference between clinical conditions and laboratory environments, caution is advised in interpreting the results. It is suggested to verify the superiorcaries detecting abilities of DIAGNOdent via clinical studies. DIAGNOdent proved to be an effective method for detecting secondary caries under composite restorations of primary molars. It is suggested to use this device along with conventional methods such as radiographs and clinical examinations.
CONCLUSION
DIAGNOdent has a higher sensitivity and specificity compared to radiographs. The +PV and −PV and also the +LR of DIAGNOdent is higher than radiographs
DIAGNOdent proved to be more accurate than radiographs for detecting secondary caries under composite restorations of primary molars but the difference was not significant
DIAGNOdent should be used alongside conventional methods such as radiographs and clinical examinations.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Matteson SR, Phillips C, Kantor ML, Leinedecker T. The effect of lesion size, restorative material, and film speed on the detection of recurrent caries. Oral Surg Oral Med Oral Pathol. 1989;68:232–7. doi: 10.1016/0030-4220(89)90199-0. [DOI] [PubMed] [Google Scholar]
- 2.Goshima T, Goshima Y. The optimum level of radiopacity in posterior composite resins. Dentomaxillofac Radiol. 1989;18:19–21. doi: 10.1259/dmfr.18.1.2599234. [DOI] [PubMed] [Google Scholar]
- 3.Nair M, Tyndal D, Ludlow J, May K, Ye F. The effects of restorative material and location on the detection of simulated recurrent caries. A comparison of dental film, direct digital radiograph and tuned aperture computed tomography. Dentomaxillofac Radiol. 1998;27:80–4. doi: 10.1038/sj/dmfr/4600323. [DOI] [PubMed] [Google Scholar]
- 4.Hintze H, Wenzel A, Frydenberg M. Accuracy of caries detection with four storage phosphor systems and E-speed radiographs. Dentomaxillofac Radiol. 2002;31:170–5. doi: 10.1038/sj/dmfr/4600686. [DOI] [PubMed] [Google Scholar]
- 5.Kositbowornchai S, Sukanya C, Tidarat T, Chanoggarn T. Caries detection under composite restorations by laser fluorescence and digital radiography. Clin Oral Investig. 2013;17:2079–84. doi: 10.1007/s00784-012-0908-9. [DOI] [PubMed] [Google Scholar]
- 6.Hellén-Halme K, Petersson GH. Influence of education level and experience on detection of approximal caries in digital dental radiographs. An in vitro study. Swed Dent J. 2010;34:63–9. [PubMed] [Google Scholar]
- 7.Kaakko T, Riedy CA, Nakai Y, Domoto P, Weinstein P, Milgrom P. Taking bitewing radiographs in preschoolers using behavior management techniques. ASDC J Dent Child. 1999;66:320–4, 294. [PubMed] [Google Scholar]
- 8.Pontual AA, de Melo DP, de Almeida SM, Bóscolo FN, Haiter Neto F. Comparison of digital systems and conventional dental film for the detection of approximal enamel caries. Dentomaxillofac Radiol. 2010;39:431–6. doi: 10.1259/dmfr/94985823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Senel B, Kamburoglu K, Uçok O, Yüksel SP, Ozen T, Avsever H. Diagnostic accuracy of different imaging modalities in detection of proximal caries. Dentomaxillofac Radiol. 2010;39:501–11. doi: 10.1259/dmfr/28628723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lussi A, Imwinkelried S, Pitts N, Longbottom C, Reich E. Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res. 1999;33:261–6. doi: 10.1159/000016527. [DOI] [PubMed] [Google Scholar]
- 11.Shi XQ, Welander U, Angmar-Månsson B. Occlusal caries detection with KaVo DIAGNOdent and radiography: An in vitro comparison. Caries Res. 2000;34:151–8. doi: 10.1159/000016583. [DOI] [PubMed] [Google Scholar]
- 12.Rahiotis C, Vougiouklakis G. Effect of a CPP-ACP agent on the demineralization and remineralization of dentine in vitro. J Dent. 2007;35:695–8. doi: 10.1016/j.jdent.2007.05.008. [DOI] [PubMed] [Google Scholar]
- 13.Virajsilp V, Thearmontree A, Aryatawong S, Paiboonwarachat D. Comparison of proximal caries detection in primary teeth between laser fluorescence and bitewing radiography. Pediatr Dent. 2005;27:493–9. [PubMed] [Google Scholar]
- 14.Attrill DC, Ashley PF. Occlusal caries detection in primary teeth: A comparison of DIAGNOdent with conventional methods. Br Dent J. 2001;190:440–3. doi: 10.1038/sj.bdj.4800998. [DOI] [PubMed] [Google Scholar]
- 15.Anttonen V, Seppä L, Hausen H. Clinical study of the use of the laser fluorescence device DIAGNOdent for detection of occlusal caries in children. Caries Res. 2003;37:17–23. doi: 10.1159/000068227. [DOI] [PubMed] [Google Scholar]
- 16.Kavvadia K, Lagouvardos P. Clinical performance of a diode laser fluorescence device for the detection of occlusal caries in primary teeth. Int J Paediatr Dent. 2008;18:197–204. doi: 10.1111/j.1365-263X.2007.00913.x. [DOI] [PubMed] [Google Scholar]
- 17.Bamzahim M, Aljehani A, Shi XQ. Clinical performance of DIAGnodent in the detection of secondary carious lesions. Acta Odontol Scand. 2005;63:26–30. doi: 10.1080/00016350510019621. [DOI] [PubMed] [Google Scholar]
- 18.Rodrigues JA, Neuhaus KW, Hug I, Stich H, Seemann R, Lussi A. In vitro detection of secondary caries associated with composite restorations on approximal surfaces using laser fluorescence. Oper Dent. 2010;35:564–71. doi: 10.2341/09-332-L. [DOI] [PubMed] [Google Scholar]
- 19.Hitij T, Fidler A. Effect of dental material fluorescence on DIAGNOdent readings. Acta Odontol Scand. 2008;66:13–7. doi: 10.1080/00016350701810641. [DOI] [PubMed] [Google Scholar]
- 20.Yamaguchi K, Miyazaki M, Takamizawa T, Inage H, Moore BK. Effect of CPP-ACP paste on mechanical properties of bovine enamel as determined by an ultrasonic device. J Dent. 2006;34:230–6. doi: 10.1016/j.jdent.2005.06.005. [DOI] [PubMed] [Google Scholar]
- 21.Chowdhary N, Subba Reddy VV. Dentin comparison in primary and permanent molars under transmitted and polarised light microscopy: An in vitro study. J Indian Soc Pedod Prev Dent. 2010;28:167–72. doi: 10.4103/0970-4388.73793. [DOI] [PubMed] [Google Scholar]
- 22.Angker L, Nockolds C, Swain MV, Kilpatrick N. Quantitative analysis of the mineral content of sound and carious primary dentine using BSE imaging. Arch Oral Biol. 2004;49:99–107. doi: 10.1016/j.archoralbio.2003.08.006. [DOI] [PubMed] [Google Scholar]
- 23.Tranaeus S, Shi XQ, Lindgren LE, Trollsås K, Angmar-Månsson B. In vivo repeatability and reproducibility of the quantitative light-induced fluorescence method. Caries Res. 2002;36:3–9. doi: 10.1159/000057583. [DOI] [PubMed] [Google Scholar]
- 24.Francescut P, Zimmerli B, Lussi A. Influence of different storage methods on laser fluorescence values: A two-year study. Caries Res. 2006;40:181–5. doi: 10.1159/000092223. [DOI] [PubMed] [Google Scholar]
- 25.Sridhar N, Tandon S, Rao N. A comparative evaluation of DIAGNOdent with visual and radiography for detection of occlusal caries: An in vitro study. Indian J Dent Res. 2009;20:326–31. doi: 10.4103/0970-9290.57376. [DOI] [PubMed] [Google Scholar]
- 26.Diniz MB, Boldieri T, Rodrigues JA, Santos-Pinto L, Lussi A, Cordeiro RC. The performance of conventional and fluorescence-based methods for occlusal caries detection: An in vivo study with histologic validation. J Am Dent Assoc. 2012;143:339–50. doi: 10.14219/jada.archive.2012.0176. [DOI] [PubMed] [Google Scholar]
- 27.Pourhashemi SJ, Jafari A, Motahhari P, Panjnoosh M, Kharrazi Fard MJ, Sanati I, et al. An in-vitro comparison of visual inspection, bite-wingradiography, and laser fluorescence methods for the diagnosis of occlusal caries. J Indian Soc Pedod Prev Dent. 2009;27:90–3. doi: 10.4103/0970-4388.55333. [DOI] [PubMed] [Google Scholar]
- 28.Mepparambath R, S Bhat S, K Hegde S, Anjana G, Sunil M, Mathew S. Comparison of Proximal Caries Detection in Primary Teeth between Laser Fluorescence and Bitewing Radiography: An in vivo Study. Int J Clin Pediatr Dent. 2014;7:163–7. doi: 10.5005/jp-journals-10005-1257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Akbari M, Ahrari F, Jafari M. A comparative evaluation of DIAGNOdent and caries detector dye in detection of residual caries in prepared cavities. J Contemp Dent Pract. 2012;13:515–20. doi: 10.5005/jp-journals-10024-1178. [DOI] [PubMed] [Google Scholar]
- 30.Lussi A, Megert B, Longbottom C, Reich E, Francescut P. Clinical performance of a laser fluorescence device for detection of occlusal caries lesions. Eur J Oral Sci. 2001;109:14–9. doi: 10.1034/j.1600-0722.2001.109001014.x. [DOI] [PubMed] [Google Scholar]
- 31.Huth KC, Lussi A, Gygax M, Thum M, Crispin A, Paschos E, et al. In vivo performance of a laser fluorescence device for the approximal detection of caries in permanent molars. J Dent. 2010;38:1019–26. doi: 10.1016/j.jdent.2010.09.001. [DOI] [PubMed] [Google Scholar]