

Abstract
Adenoid ameloblastoma with dentinoid is a rare odontogenic tumor. Granular cell ameloblastoma also is a less common histological subtype of ameloblastoma. In this report, the patient was a 31-year-old male. The lesion was located in the right mandible and was unicystic with well-defined borders. The tumor tissue was showing a combination of follicular, plexiform, and desmoplastic patterns of ameloblastoma with wide areas of granular cells, fibrous stroma, glandular pattern, and dentinoid calcified. Very few cases of distinct forms of ameloblastoma that show the formation of dentinoid has been reported. However, there are no cases of adenoid granular cell ameloblastoma with dentinoid reported.
Key Words: Adenoids, ameloblastoma, cytoplasmic granules, odontogenic tumors
INTRODUCTION
Ameloblastomas are benign but locally invasive tumors of odontogenic epithelial origin and generally without induction in the connective tissue.[1] Rare cases of ameloblastoma associated with an odontome have been reported and are known as “odontoameloblastoma.”[2]
In 1992, the first case of an ameloblastoma showing evidence of induction of dentinoid which diagnosed as a “dentinoameloblastoma” was reported by Slabbert et al.[3] The term “adenoid ameloblastoma with dentinoid” was first introduced by Evans et al. in 2004. They described a neoplasm showing histopathological features similar to ameloblastoma and adenomatoid odontogenic tumor (AOT) along with hard tissue formation.[4]
Histopathologically, ameloblastoma exhibits follicular, plexiform, acanthomatous, granular cell, desmoplastic, and basal cell patterns. Granular cell ameloblastoma is rare to occur and accounts for only 5% of all ameloblastomas.[5] Based on current knowledge, there is no reported case of granular cell ameloblastoma with dentinoid in the literature. In this paper, we present a case of a rare histological subtype of ameloblastoma with large amounts of granular cells, glandular pattern, and dentinoid areas in the right mandible of a 31-year-old male. Final histopathological diagnosis of adenoid granular cell ameloblastoma with dentinoid was made for this entity.
CASE REPORT
A 31-year-old man was referred to us with a chief complaint of a swelling on the left side of the mandible, which had been presented for nearly 1 month. Clinical examination revealed a localized expansion of the left mandible covered by normal oral mucosa.
The swelling was painful with palpation, soft in consistency, and fluctuant in nature. No history of numbness or other abnormal sensations was mentioned. The tumor caused mobility and displacement of left mandibular canine, first and second premolars. The involved teeth were vital. Cervical lymph nodes were not palpable. Patient's medical and dental history was unremarkable.
Radiographically, panoramic view showed a unilocular radiolucency with well-defined borders extending from the left canine to the left mandibular second molar. There was root divergence, but no root resorption and the lamina dura of the affected teeth were destroyed [Figure 1a].
Figure 1.

(a) radiolucent lesion occupying the body of the left mandible. (b) Axial Cone beam computed tomography image.
Cone beam computed tomography scan showed a radiolucent lesion in the left mandibular area with buccal and lingual cortices destruction [Figure 1b].
Radiographic differential diagnosis includes central giant cell granuloma, ameloblastoma, odontogenic myxoma, and keratocystic odontogenic tumor was given. Then, incisional biopsy was performed. Specimen was sent to the department of oral and maxillofacial pathology. The sections showed a combination of follicular, plexiform, and desmoplastic patterns of ameloblastoma [Figure 2a and b] with wide areas of granular cells and fibrous stroma [Figure 2c and d]. Dentinoid calcified [Figure 3a and b] and occasionally glandular area were observed in some sections [Figure 3c and d].
Figure 2.
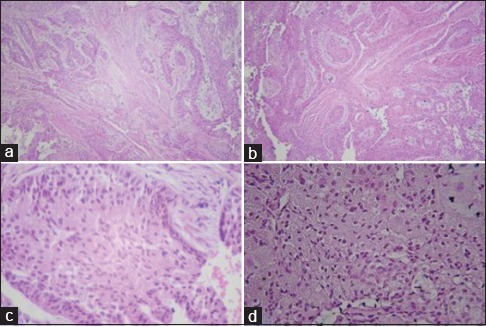
(a and b) Combination of follicular, plexiform, and desmoplastic patterns of ameloblastoma. (c and d) Proliferation of a large amount of granular cells.
Figure 3.
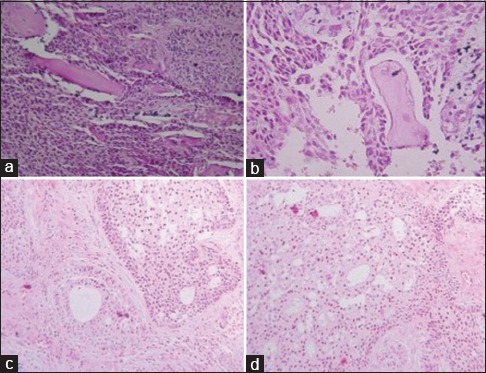
(a and b) Matrix material consistent with dentinoid. (c and d) Zone of follicular pattern of ameloblastoma demonstrating peripheral ameloblastic cells and duct-like pattern. The central zone exhibiting granular cells and foci of cystic degeneration.
Considering these features, a provisional histopathological diagnosis was considered.
The patient was submitted for left partial hemimandibulectomy from left central incisor to left third molar area.
Histopathological examination of the last specimen showed neoplastic proliferation of odontogenic epithelial cells in follicular and plexiform patterns and large amounts of granular cells. Occasionally, wide fibrous stroma, glandular pattern, and dentinoid areas were observed. Considering the histopathological features of present and previous tissue sections, the diagnosis of adenoid granular cell ameloblastoma with dentinoid was confirmed. The patient is under close follow-up and shows no evidence of recurrence 18 months after the operation.
DISCUSSION
Granular cell ameloblastoma is a rare subtype of ameloblastoma in which granular cells located in the center of the follicles.[6] Its median age is 35-year-old with no distinct gender predilection in the literature.[7]
Granular cell ameloblastoma should be differentiated from other odontogenic and nonodontogenic lesions along with granular cells, including granular cell tumor, congenital epulis, and granular cell odontogenic tumor.[8]
The granular cell tumor is a soft tissue tumor and should be distinguished from ameloblastomas that cause cortical perforation and soft tissue extension.[9] Congenital epulis is also a soft tissue tumor and with regards to its age outbreak, there is no need to distinguish it from a granular cell ameloblastoma.[9] Granular cell odontogenic tumors exhibit a proliferation of large cells with eosinophilic granular cytoplasm and may show dystrophic calcifications.[10] Granules of granular cells in granular cell ameloblastoma are positive for cytokeratin, CD68, lysozyme, and alpha-1-antichymotrypsin, and in granular cell odontogenic tumor are positive for vimentin, CD68, lysozyme, muscle-specific actin, alpha-smooth muscle actin, calponin, neuron-specific enolase, CD138, and bcl-2 in immunohistochemistry (IHC) staining.[11] Granular cell lesions are easy to rule out with observing follicular, plexiform, and desmoplastic patterns of ameloblastoma in the specimens.
In this case, differential diagnosis between adenoid ameloblastoma with dentinoid and AOT is also important. This is due to the presence of glandular pattern and dentinoid areas in the histopathological assessment. Duct-like structures are the characteristic of the AOTs, and dystrophic calcifications are usually seen in these lesions.[10] Considering that granular cell is not exist in AOTs, distinction between the present case and AOT was performed without IHC.
Few reports of ameloblastoma along with hard tissue formation were found in the literature. Bone formation was only reported in one neoplasm,[12] two polycystic ameloblastomas showed diffuse interstitial ossification[13] and enamel formation were described in few reports.[14] In most other reported cases, the hard tissue had been construed as dentin or dentinoid.[15] Consequently, hard tissue in these unusual cases of ameloblastoma has a wide variety of nature.
Finally, because of an existing neoplastic proliferation of odontogenic epithelial cells in follicular, plexiform and glandular patterns, dentinoid areas, and abundant granular cells, we concluded the present tumor to be a rare case of adenoid granular cell ameloblastoma with dentinoid. To make accurate diagnosis, it is essential that all the oral and maxillofacial pathologist to be aware of this entity.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Torres-Lagares D, Infante-Cossío P, Hernández-Guisado JM, Gutiérrez-Pérez JL. Mandibular ameloblastoma. A review of the literature and presentation of six cases. Med Oral Patol Oral Cir Bucal. 2005;10:231–8. [PubMed] [Google Scholar]
- 2.Bello I, Qannam A. Odontoameloblastoma and ameloblastic fibro-odontoma: Using case reports to illustrate differences between both lesions. Oral Surg Oral Med Oral Pathol and Oral Radiol. 2015;119:e113–4. [Google Scholar]
- 3.Slabbert H, Altini M, Crooks J, Uys P. Ameloblastoma with dentinoid induction: Dentinoameloblastoma. J Oral Pathol Med. 1992;21:46–8. doi: 10.1111/j.1600-0714.1992.tb00969.x. [DOI] [PubMed] [Google Scholar]
- 4.Evans BL, Carr RF, Phillipe LJ. Adenoid ameloblastoma with dentinoid: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:583–8. doi: 10.1016/j.tripleo.2004.02.077. [DOI] [PubMed] [Google Scholar]
- 5.Sharma SH, Hasan R, Kumar S, Shivamurthy A, Shetty T. Cytology of granular cell ameloblastoma of jaw: A rare case entity. Int J Sci Study. 2015;3:224–6. [Google Scholar]
- 6.Gardner DG, Heikinheimo K, Shear M, Philipsen HP, Coleman H. Ameloblastoma. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization Classification of Tumors, Pathology and Genetics of Head and Neck Tumors. Lyon: IARC Press; 2005. pp. 296–300. [Google Scholar]
- 7.Reichart PA, Philipsen HP, Sonner S. Ameloblastoma: Biological profile of 3677 cases. Eur J Cancer B Oral Oncol. 1995;31B:86–99. doi: 10.1016/0964-1955(94)00037-5. [DOI] [PubMed] [Google Scholar]
- 8.Mirchandani R, Sciubba JJ, Mir R. Granular cell lesions of the jaws and oral cavity: A clinicopathologic, immunohistochemical, and ultrastructural study. J Oral Maxillofac Surg. 1989;47:1248–55. doi: 10.1016/0278-2391(89)90718-0. [DOI] [PubMed] [Google Scholar]
- 9.Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 4th ed. St. Louis: Mosby Elsevier; 2016. Soft Tissue Tumors; pp. 473–532. [Google Scholar]
- 10.Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology. 4th ed. St. Louis: Mosby Elsevier; 2016. Odontogenic cysts and tumors; pp. 632–89. [Google Scholar]
- 11.Yogesh TL, Sowmya SV. Granules in granular cell lesions of the head and neck: A review. ISRN Pathol. 2011;2011:1–10. [Google Scholar]
- 12.Okada Y, Sugimura M, Ishida T. Ameloblastoma accompanied by prominent bone formation. J Oral Maxillofac Surg. 1986;44:555–7. doi: 10.1016/s0278-2391(86)80095-7. [DOI] [PubMed] [Google Scholar]
- 13.Raubenheimer EJ, van Heerden WF, Noffke CE. Infrequent clinicopathological findings in 108 ameloblastomas. J Oral Pathol Med. 1995;24:227–32. doi: 10.1111/j.1600-0714.1995.tb01172.x. [DOI] [PubMed] [Google Scholar]
- 14.Boyle P, Kalnins V. Enamel formation in ameloblastomas. Arch Oral Biol. 1960;2:285–88. [Google Scholar]
- 15.Kumar K, Shetty DC, Wadhwan V, Dhanapal R, Singh HP. Dentinoameloblastoma with ghost cells: A rare case report with emphasis on its biological behavior. Dent Res J (Isfahan) 2013;10:103–7. doi: 10.4103/1735-3327.111809. [DOI] [PMC free article] [PubMed] [Google Scholar]