

Abstract
Background and study aims: In the elderly population, there is a growing demand for minimally invasive procedures as the incidence of pancreaticobiliary disease increases with age. Patients with advanced age offer unique challenges for any procedure because they also tend to have a higher rate of baseline comorbidities and malignancy. The aim of the current study was to characterize the mortality and length of stay of octogenarians undergoing inpatient endoscopic retrograde cholangiopancreatography (ERCP).
Patients and methods: Using the 2007 – 2010 Nationwide Inpatient Sample (NIS), we performed a retrospective analysis of health-related outcomes among 80- to 89-year-old patients undergoing inpatient ERCP. Surgical patients were excluded.
Results: An estimated 61,322 octogenarians underwent inpatient ERCP in the United States from 2007 to 2010. The mean age was 84.2 (SE 0.02) with 59.5 % (n = 36,460) of the patients being female. A large majority of the patients were white (79. %, n = 41,144) and 63.5 % (n = 38,940) had a comorbidity index of at least 2. The mean length of stay was 7.1 days (SE 0.08) with an in-hospital mortality of 3.1 % (n = 1,919). The primary discharge diagnosis was most often biliary stone disease (55.9 %, n = 34,263). A diagnosis of any infection was recorded in 45.0 % (n = 27,609) of patients. Infection was associated with a significantly higher risk of in-hospital mortality (OR 3.3, 95 % CI 2.6 – 4.2, P < 0.001).
Conclusions: ERCP is now routinely being performed during inpatient admissions for octogenarians with diseases of the biliary tract. The mortality of octogenarians undergoing inpatient ERCP is higher than previous reports and is likely due to superimposed infection during the same admission.
Introduction
The growing elderly population in the United States has led to escalating healthcare utilization and expenditures. Healthcare expenses associated with the baby boomer generation grew 7.6 % from 2002 to 2010, which was faster than in any other age group 1. Concomitantly, the demand for ERCP in the elderly has risen secondary to a high incidence of pancreaticobiliary disease in this population 2 3. By the time a patient turns 70, the prevalence of gallbladder-related disease in the United States is 33 % for females and 25 % for males 4.
ERCP is now widely available in the United States at both academic and local non-teaching hospitals. Known complications from ERCP include acute pancreatitis, perforation, infection, gastrointestinal bleeding, adverse effect of anesthetic agents, and death 3. There are few studies available regarding the safety of ERCP in patient aged 80 years and older 5 6 7 8 9. These small, single-institution studies suggest that ERCP is safe in the elderly population 10.
The aim of this population-based study is to characterize the mortality and length of stay in octogenarians undergoing inpatient ERCP. To our knowledge, no prior studies have evaluated the in-hospital mortality associated with ERCP in a large cohort of elderly patients. Based on the limited data available, we hypothesize that ERCP is safe to perform on hospitalized octogenarians.
Patients and methods
Design
We performed a retrospective analysis of a national inpatient administrative database.
Database
Our institutional reviewed board approved this study using the Nationwide Inpatient Sample (NIS) which is part of a family of databases developed and compiled by the Healthcare Cost and Utilization Project (H-CUP) [Agency for Healthcare Research and Quality/H-CUP (December 2014). http:www.hcup-us.ahrq.gov/nisoverview.jsp (February 01 2015)]. The NIS is the largest publicly available all-payer inpatient healthcare database in the United States, yielding estimates of hospital inpatient stays. The NIS approximates a 20 % stratified sample of discharges from US community hospitals, which then allows for national-level estimates by using a weighting coefficient provided by the database 10. Rehabilitation and long-term acute care hospitals are excluded from the database. Policymakers, insurers, and researchers use NIS data to make national estimates of health care utilization, charges, quality, outcomes, and access. The NIS includes data typically found in discharge abstracts, such as up to 25 diagnosis and procedure codes, patient characteristics, length of stay, and payer source. The NIS data excludes individual identifiers.
Sample selection
We queried the NIS database for all ERCP procedures performed for any indication from 2007 to 2010 on inpatients whose age was 80 to 89. Admissions that contained complete age, in-hospital mortality data, and length of stay were included in the sample cohort. Patients who also underwent a surgical procedure, such as cholecystectomy, during the same admission were excluded from our study. Fig. 1 outlines the cohort selection process represented as raw counts, not United States population estimates.
Fig. 1.
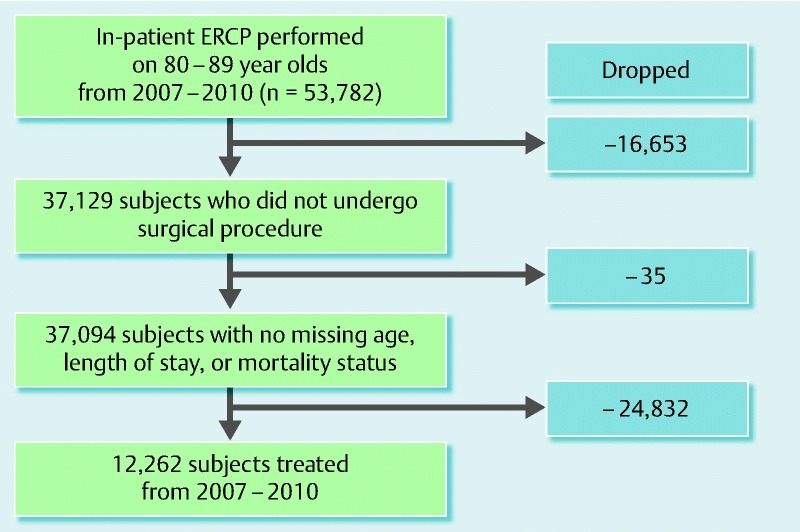
Cohort selection process represented as raw counts, not United States population estimates
Study variables
Primary outcomes considered in our study were in-hospital mortality and length of stay in octogenarians who underwent ERCP in the United States from 2007 through 2010. In-hospital mortality only includes deaths during the same admission as the ERCP. These mortality data do not include any deaths post-hospitalization. Length of stay was defined as the number of days from admission to the date of discharge. ERCP procedure codes were defined according to the International Classification of Disease, ninth revision, Clinical Modification (ICD-9-CM) system. Therapeutic ERCP procedure codes included both endoscopic operations on biliary ducts and the sphincter of Oddi (51.84 – 5.88) as well as endoscopic interventions on the pancreas (51.93, 51.94, 51.97, and 51.98). Diagnostic ERCP procedure codes were as follows: ERC (51.11), ERP (52.13), ERCP (51.10), ERCP with biopsy (51.14, 52.14), ERCP with excision/destruction of a lesion (51.64, 52.21), and ERCP with manometry (51.15). All of the aforementioned procedure codes were combined to represent the total number of ERCP procedures. Discharge diagnoses were categorized as pancreatitis, stone disease, infection, malignancy, and other (Supplementary Table 1).
Table 1. Characteristics of octogenarians who underwent ERCP while hospitalized from 2007 to 2010 (n = 61,322).
| Variable | Estimated |
| Sex, female, n (%) | 36,460 (59.5) |
| Age, years, mean (SE) | 84 (0.02) |
| Race, n (%)1 | |
| White | 41,144 (79.9) |
| Hispanic | 4,032 (7.8) |
| African-American | 2,670 (5.2) |
| Other | 3,669 (7.1) |
| More than 2 comorbidities, n (%)2 | 38,940 (63.5) |
| Alcohol abuse, n (%) | 534 (0.9) |
| Study period, n (%) | |
| 2007 | 14,996 (24.5) |
| 2008 | 15,632 (25.5) |
| 2009 | 15,220 (24.8) |
| 2010 | 15,473 (25.2) |
| Hospital region, n (%) | |
| Northeast | 15,567 (25.4) |
| Midwest | 14,539 (23.7) |
| South | 19,140 (31.2) |
| West | 12,076 (19.7) |
| Urban hospital, n (%) | 56,889 (93.1) |
| Hospital teaching, n (%) | 30,188 (49.4) |
| Primary payer, n (%)3 | |
| Medicare | 56,182 (91.7) |
| Medicaid | 973 (1.6) |
| Private insurance | 3,376 (5.5) |
| Self-pay, no charge, other | 759 (1.2) |
| Admission source, n (%) | |
| Routine | 6,814 (26.3) |
| Emergency department | 16,937 (65.5) |
| Other facility4 | 2,123 (8.2) |
| Admission type, n (%) | |
| Emergency | 34,600 (64.5) |
| Urgent | 12,284 (22.9) |
| Elective | 6,700 (12.5) |
| Other | 39 (0.07) |
| Hospital bed size, n (%) | |
| Small | 5,366 (8.8) |
| Medium | 14,331 (23.5) |
| Large | 41,382 (67.8) |
| Length of stay, days, mean (SE) | 7.1 (0.08) |
| In-hospital mortality, n (%) | 1,919 (3.13) |
Characteristics for patients and hospitals were then extracted from the dataset such as sex, race, age, primary payer, hospital region, teaching status of hospital, hospital size, urban or rural institution, year of admission, source of admission, and number of comorbidities. Hospital size is defined by the NIS and is specific to region, location, and teaching status; for example, a large urban teaching hospital in the south has more than 450 beds [Agency for Healthcare Research and Quality/H-CUP (December 2014). http://www.hcup-us.ahrq.gov/nisoverview.jsp (February 01 2015)]. Each patient was then assigned a comorbidity score based on the Elixhauser comorbidity algorithm using validated H-CUP comorbidity software [Agency for Healthcare Research and Quality/H-CUP (October 2011). http://www.hcup-us.ahrq.gov/toolssoftware/comorbidity.jsp (May 01 2015), 11 12.
Statistical Analysis
All analysis was performed in SAS Version 9.4 (Cary, NC). Because NIS implements a stratified, weighted, sampling strategy, all data are presented as national estimates. Appropriate SAS procedures, such as PROC SURVEYMEANS, PROC SURVEYFREQ, and PROC SURVEYLOGISTIC, were used to accurately incorporate the sampling strategy of NIS into national estimates. Continuous variables were summarized using means and standard errors, and nominal variables were summarized using counts and percentages. To determine characteristics associated with mortality, univariate and multi-variable logistic regression were used. Variables with overall p-values less than 0.10 were retained in the multi-variable model.
Results
An estimated 61,322 octogenarians underwent inpatient ERCP in the United States from 2007 to 2010. The baseline characteristics of the patients and hospitals are shown in Table 1. The mean age at time of admission was 84.2 (SE 0.02) with 59.5 % (n = 36,460) of the patients being female. A large majority of the patients were white (79. %, n = 41,144) and 63.5 % (n = 38,940) had a comorbidity index of at least 2. ERCP was usually performed at large (67.7 %, n = 41,382), urban (93.1 %, n = 56,889) institutions. The procedures were equally distributed between teaching (50.6 %) and non-teaching hospitals (49.4 %). Most of the admissions were classified as emergent (64.5 %, n = 34,600). Medicare was the leading payer source (91.7 %, n = 56,182).
The mean length of stay (LOS) was 7.1 days (SE 0.08). The most common discharge diagnosis was pancreaticobiliary stone disease in 55.9 % (Table 2). The overall in-hospital mortality for octogenarians who had an ERCP performed during the admission was 3.1 % (n = 1,919). Risk factors for in-hospital mortality were evaluated. Odds ratio (OR) estimates were calculated for the variables listed in Table 3. Any infection (OR 3.3, 95 % CI 2.6 – 4.2, P < 0.001), presence of more than 2 comorbidities (OR 2.4, 95 % CI 1.9 – 3.2, P < 0.001), and malignancy (OR 1.6, 95 %CI 1.6 – 2.0, P < 0.001) were all associated with higher risk of in-hospital mortality. Age, sex, ethnicity, and hospital characteristics (size, region, rural or urban) were not associated with increased mortality. In multivariate analysis, octogenarians with any infection had a significantly higher risk of in-hospital mortality (OR 3.1, 95 % CI 2.5 – 4.0, P < 0.001). The presence of more than 2 more comorbidities, malignancy, and increasing age were also associated with slightly higher in-hospital mortality in the multivariate analysis.
Table 2. Most common discharge diagnoses for octogenarians undergoing Inpatient ERCP.
| Estimated | |
| Discharge diagnosis1 | N (%) |
| Pancreaticobiliary stone disease | 34,263 (55.9) |
| Malignancy | 18,272 (29.8) |
| Infection | 27,609 (45.0) |
| Pancreatitis | 5,765 (9.4) |
See Appendix Supplemental Table 1 for ICD-9 codes.
Table 3. Risk factors for in-hospital mortality in octogenarians undergoing ERCP.
| Univariate analysis | Multiple variable analysis | |||||||
| Variable | OR | 95 % CI Lower | 95 % CI Upper | p-value | OR | 95 % CI Lower | 95 % CI Upper | P value |
| Age1 | 1.05 | 0.997 | 1.096 | 0.0674 | 1.050 | 1.001 | 1.101 | 0.0463 |
| Male sex | 1.207 | 0.984 | 1.481 | 0.0717 | 0.870 | 0.706 | 1.071 | 0.1879 |
| More than 2 comorbidities2 | 2.447 | 1.868 | 3.206 | < 0.001 | 1.446 | 1.285 | 1.626 | < 0.001 |
| Race, non-white | 1.174 | 0.911 | 1.513 | 0.2145 | ||||
| Hospital size | ||||||||
| Small | ref | |||||||
| Medium | 1.162 | 0.731 | 1.845 | 1.162 | ||||
| Large | 1.218 | 0.791 | 1.874 | 0.426 | ||||
| Non-teaching hospital | 0.772 | 0.631 | 0.944 | 0.0117 | 0.787 | 0.641 | 0.966 | 0.0218 |
| Region | ||||||||
| West | ref | |||||||
| Northeast | 0.993 | 0.736 | 1.340 | 0.9646 | ||||
| Midwest | 0.825 | 0.611 | 1.114 | 0.2086 | ||||
| South | 0.942 | 0.720 | 1.232 | 0.6618 | ||||
| Rural hospital | 1.002 | 0.706 | 1.421 | 0.9932 | ||||
| Admission source, emergency department | 0.954 | 0.669 | 1.361 | 0.7952 | ||||
| Admission type | ||||||||
| Urgent or emergent | ref | ref | ||||||
| Elective | 0.642 | 0.423 | 0.976 | 0.038 | 0.748 | 0.483 | 1.157 | 0.1919 |
| Any stone disease | 0.533 | 0.433 | 0.656 | < 0.001 | 0.571 | 0.441 | 0.739 | < 0.001 |
| Any infection | 3.329 | 2.649 | 4.184 | < 0.001 | 3.105 | 2.523 | 4.070 | < 0.001 |
| Any malignancy | 1.616 | 1.320 | 1.977 | < 0.001 | 1.28 | 1.005 | 1.629 | 0.00453 |
| Any pancreatitis | 0.751 | 0.571 | 0.988 | 0.0405 | 0.960 | 0.723 | 1.274 | 0.7771 |
Discussion
Our study determined that the in-hospital mortality for octogenarians who undergo inpatient ERCP is 3.1 %. To our knowledge, this is the first large-scale population-based study to examine mortality and length of stay in octogenarians undergoing inpatient ERCP. Because this analysis used a nationally representative sample of octogenarian patients who underwent inpatient ERCP in the community setting, these findings can be generalized to the overall US octogenarian population.
Prior reports would suggest that ERCP is safe and without increased mortality or complication rates in octogenarians 3 5 6 7 8 9. In one retrospective review comparing 102 patients older than age 80 to a younger cohort, ERCP was both safe and efficacious without an increase in complication rates 5. Although ERCP procedure time was usually longer and the case technically more challenging in octogenarians, ERCP was not found to have higher complication rates in this elderly cohort 6. In fact, rates of post-ERCP infection and pancreatitis were lower in octogenarians.
Generally, all patients who undergo ERCP procedures have a mortality of less than 0.5 % 13 14 15. Prior small studies focusing on the very elderly such as octogenarians found a mortality rate of 0 – 1 % 3 6 7 8 9 10 16. The mortality of octogenarians in our study was over 3 %. Almost half of the hospitalized octogenarians we evaluated had an infection during the same hospitalization at the time of ERCP and one-third had a diagnosed malignancy. Infection and malignancy includes both biliary and non-biliary etiologies such as pneumonia and lymphoma. Given concern for selection bias using an administrative dataset, we did not perform a subset analysis of patients diagnosed with cholangitis. However, cholangitis is likely a significant factor in increased in-hospital morbidity and mortality. Many octogenarians also had numerous comorbidities and the presence of more than 2 comorbidities was associated with higher inpatient mortality.
Accordingly, the finding of higher mortality in octogenarians is best explained by the increased rates of infections and malignancy in this population with baseline comorbidities. Although, the mortality rate in this study for octogenarians undergoing inpatient ERCP is higher than in previous reports, the procedure remains necessary and efficacious for many individuals. With careful patient selection and high-quality periprocedural care, we can likely minimize risks associated with ERCP in octogenarians. We recommend that patients and families undergo appropriate informed consent including information on inpatient mortality before any inpatient ERCP.
The average length of stay for octogenarians undergoing ERCP was 7.1 days in our study. This is comparable to the reported length of stay for all age groups undergoing inpatient ERCP of 6.9 – 7.8 days 15. Our large sample size should mitigate the effects of individual hospital characteristics on length of stay such as a lower procedure volume or fewer critical care resources.
Our study has a few limitations. The NIS database allows for only the assessment of inpatient mortality, morbidity, and length of stay. Death after discharge or complications requiring readmission cannot be tracked or evaluated because the NIS data are only from inpatient hospitalizations and contains no individual identifiers. We cannot comment on the mortality in outpatient octogenarians who undergo ERCP as this study only utilized hospitalized patients. All patients who underwent any surgical procedure during the same admission were excluded from the analysis in an attempt to limit confounders on inpatient mortality in this very elderly cohort. By excluding surgical patients, we may be eliminating some healthier patients that were surgical candidates and thus potentially would have lowered the mortality. Conversely, we are also excluding patients that had potential ERCP morbidities such as perforation that would have required urgent surgery and likely had a higher mortality.
Conclusion
In this large-scale population-based study of inpatient octogenarians undergoing ERCP, the rate of in-hospital mortality was 3.1 % and the length of stay was 7.1 days. Although the length of stay was comparable to all age groups, the mortality was higher than in previous reports and is attributable to concomitant infection and malignancy in this elderly cohort with baseline comorbidities.
Supplemental Table 1 . ICD-9 codes for discharge diagnosis categories.
| Discharge diagnosis category | ICD-9 codes |
| Stone disease | 560.31-gallstone ileus, 574.00-claculus of gallbladder with acute cholecystitis without obstruction, 574.01 – claculus of gallbladder with acute cholecystitis with obstruction,, 574.10-calculus of gallbladder with other cholecystitis without obstruction, 574.11-calculus of gallbladder with other cholecystitis with obstruction, 574.20-calculus of gallbladder without cholecystitis without obstruction, 574.21-calculus of gallbladder without cholecystitis with obstruction, 574.30-calculus of bile duct with acute cholecystitis without obstruction, 574.31-calculus of bile duct with acute cholecystitis with obstruction,, 574.40-calculus of bile duct with other cholecystitis without obstruction, 574.41-calculus of bile duct with other cholecystitis with obstruction,, 574.50-calculus of bile duct without cholecystitis without obstruction, 574.51 calculus of bile duct without cholecystitis with obstruction, 574.60-calculus of gallbladder and bile duct with acute cholecystitis without obstruction, 574.61-calculus of gallbladder and bile duct with acute cholecystitis with obstruction, 574.70-calculus of gallbladder and bile duct with other cholecystitis without obstruction, 574.71-calculus of gallbladder and bile duct with other cholecystitis without obstruction, 574.80-calculus of gallbladder and bile duct with acute and chronic cholecystitis without obstruction, 574.81-calculus of gallbladder and bile duct with acute and chronic cholecystitis with obstruction, 574.90-calculus of gallbladder and bile duct without cholecystitis without obstruction, 574.91-calculus of gallbladder and bile duct without cholecystitis with obstruction, 997.4-retained cholelithiasis following cholecystectomy |
| Malignancy | 147.1-malignant neoplasm of posterior wall of nasopharynx, 147.9-malignant neoplasm of nasopharynx unspecified site, 150.5-malignant neoplasm of lower third of esophagus, 150.8-malignant neoplasm of other specified part of esophagus, 151.0-malignant neoplasm of cardia, 151.1-malignant neoplasm of pylorus, 151.2-malignant neoplasm of pyloric antrum, 151.3-malignant neoplasm of fundus of stomach, 151.4-malignant neoplasm of body of stomach, 151.5-malignant neoplasm of lesser curvature of stomach unspecified, 151.6-malignant neoplasm of greater curvature of stomach unspecified, 151.8-malignant neoplasm of other specified sites of stomach, 151.9-malignant neoplasm of stomach unspecified site, 152.0-malignant neoplasm of duodenum, 152.1-malignant neoplasm of jejunum, 152.2-malignant neoplasm of ileum, 152.8-malignant neoplasm of other specified sites of small intestine, 152.9-malignant neoplasm of small intestine unspecified site, 153.0-malignant neoplasm of hepatic flexure, 153.1-malignant neoplasm of transverse colon, 153.2-malignant neoplasm of descending colon, 153.3-malignant neoplasm of sigmoid colon, 153.4-malignant neoplasm of cecum, 153.6-malignant neoplasm of ascending colon, 153.7-malignant neoplasm of splenic flexure, 153.8-malignant neoplasm of other specified sites of large intestine, 153.9-malignant neoplasm of colon unspecified site, 154.0-malignant neoplasm of rectosigmoid junction, 154.1-malignant neoplasm of rectum, 154.3-malignant neoplasm of anus unspecified site, 154.8-malignant neoplasm of other sites of rectum, rectosigmoid junction, and anus, 155.0-malignant neoplasm of liver primary, 155.1-malignant neoplasm of intrahepatic bile ducts, 155.2-malignant neoplasm of liver not specified as primary or secondary, 156.0-malignant neoplasm of gallbladder, 156.1-malignant neoplasm of extrahepatic bile ducts, 156.2-malignant neoplasm of ampulla of vater, 156.8-malignant neoplasm of other specified sites of gallbladder and extrahepatic bile ducts, 156.9-malignant neoplasm of biliary tract part unspecified site, 157.0-malignant neoplasm of head of pancreas, 157.1-malignant neoplasm of body of pancreas, 157.2-malignant neoplasm of tail of pancreas, 157.3-malignant neoplasm of pancreatic duct, 157.4-malignant neoplasm of islets of Langerhans, 157.8-malignant neoplasm of other specified sites of pancreas, 157.9-malignant neoplasm of pancreas part unspecified, 158.0-malignant neoplasm of retroperitoneum, 158.8-malignant neoplasm of specified parts of peritoneum, 158.9-malignant neoplasm of peritoneum unspecified, 159.0-malignant neoplasm of intestinal tract part unspecified, 159.8-malignant neoplasm of other sites of digestive system and intra-abdominal organs, 162.2-malignant neoplasm of main bronchus, 162.3-malignant neoplasm of upper lobe bronchus or lung, 162.5-malignant neoplasm of lower lobe bronchus or lung, 162.8-malignant neoplasm of other parts of bronchus or lung, 162.9-malignant neoplasm of bronchus and lung unspecified, 170.6-malignant neoplasm of pelvic bones sacrum and coccyx, 173.3-unspecified malignant neoplasm of skin of other and unspecified parts of face, 173.4-unspecified malignant neoplasm of scalp and skin of neck, 174.8-malignant neoplasm of other specified sites of female breast, 174.9-malignant neoplasm of breast (female) unspecified site, 182.0-malignant neoplasm of corpus uteri except isthmus, 183.0-malignant neoplasm of ovary, 185-malignant neoplasm of prostate, 188.2-malignant neoplasm of lateral wall of urinary bladder, 188.8-malignant neoplasm of other specified sites of bladder, 188.9-malignant neoplasm of bladder part unspecified, 189.0-malignant neoplasm of kidney except pelvis, 189.2-malignant neoplasm of ureter, 194.0-malignant neoplasm of adrenal gland, 195.0-malignant neoplasm of head face and neck, 195.2-malignant neoplasm of abdomen, 195.8-malignant neoplasm of other specified sites, 196.2-secondary and unspecified malignant neoplasm of intra-abdominal lymph nodes, 196.3-secondary and unspecified malignant neoplasm of lymph nodes of axilla and upper limb, 197.0-secondary malignant neoplasm of lung, 197.1-secondary malignant neoplasm of mediastinum, 197.2-secondary malignant neoplasm of pleura, 197.4-secondary malignant neoplasm of small intestine including duodenum, 197.5-secondary malignant neoplasm of large intestine and rectum, 197.6-secondary malignant neoplasm of retroperitoneum and peritoneum, 197.7-malignant neoplasm of liver secondary, 197.8-secondary malignant neoplasm of other digestive organs and spleen, 198.1-secondary malignant neoplasm of other urinary organs, 198.2-secondary malignant neoplasm of skin, 198.3-secondary malignant neoplasm of brain and spinal cord, 198.5-secondary malignant neoplasm of bone and bone marrow, 198.7-secondary malignant neoplasm of adrenal gland, 198.89-secondary malignant neoplasm of other specified sites, 199.0-disseminated malignant neoplasm, 199.1-other malignant neoplasm of unspecified site, 200.00-reticulosarcoma unspecified site, 200.02-reticulosarcoma involving intrathoracic lymph nodes, 200.03-reticulosarcoma involving intra-abdominal lymph nodes, 200.07-reticulosarcoma involving spleen, 200.08-reticulosarcoma involving lymph nodes of multiple sites, 200.23-Burkitt’s tumor or lymphoma involving intra-abdominal lymph nodes, 200.40-mantle cell lymphoma, unspecified site, extranodal and solid organ sites, 200.70-large cell lymphoma, unspecified site, extranodal and solid organ sites, 200.71-large cell lymphoma, lymph nodes of head, face, and neck, 200.80-other named variants of lymphosarcoma and reticulosarcoma unspecified site, 201.50-Hodgkin’s disease nodular sclerosis unspecified site, 201.55-Hodgkin’s disease nodular sclerosis involving lymph nodes of inguinal region and lower limb, 201.90-Hodgkin’s disease unspecified type unspecified site, 202.03-Nodular lymphomas involving intra-abdominal lymph nodes, 202.80-other malignant lymphomas unspecified site, 202.83 – other malignant lymphomas involving intra-abdominal lymph nodes, 202.84 other malignant lymphomas involving lymph nodes of axilla and upper limb, 202.85 – other malignant lymphomas involving lymph nodes of ingoing region and lower limb, 202.86 – other malignant lymphomas involving intrapelvic lymph nodes, 202.88 – other malignant lymphomas involving lymph nodes of multiple sites, 203.00-multiple myeloma without mention of having achieved remission, 204.00-acute lymphoid leukemia without mention of having achieved remission, 204.10-chronic lymphoid leukemia without mention of having achieved remission, 205.00-acute myeloid leukemia without mention of having achieved remission, 205.10-chronic myeloid leukemia without mention of having achieved remission, 209.00-malignant carcinoid tumor of the small intestine, unspecified portion, 209.23-malignant carcinoid tumor of the stomach, 209.72-secondary neuroendocrine tumor of liver, 211.1-benign neoplasm of stomach, 211.2-benign neoplasm of duodenum jejunum and ileum, 211.3-benign neoplasm of colon, 211.5-benign neoplasm of liver and biliary passages, 211.6-benign neoplasm of pancreas except islets of Langerhans, 215.0-other benign neoplasm of connective and other soft tissue of head face and neck, 220-benign neoplasm of ovary, 225.2-benign neoplasm of cerebral meninges, 227.1-benign neoplasm of parathyroid gland, 230.2-carcinoma in situ of the stomach, 230.7-carcinoma in situ of other and unspecified parts of intestine, 230.8-carcinoma in situ of liver and biliary system, 230.9-carcinoma in situ of other and unspecified digestive organs, 235.2-neoplasm of uncertain behavior of stomach intestines and rectum, 235.3-neoplasm of uncertain behavior of liver and biliary passages, 235.5-neoplasm of uncertain behavior of other and unspecified digestive organs, 237.5-neoplasm of uncertain behavior of brain and spinal cord, 238.73-high grade myelodysplastic syndrome lesions, 239.0-neoplasm of unspecified nature of digestive system, 239.5-neoplasm of unspecified nature of other genitourinary organs, 239.89-neoplasms of unspecified nature other specified sites, v58.11-encounter for antineoplastic chemotherapy, v71.1-observation for suspected malignant neoplasm |
| Infection | 003.1-Salmonella Septicemia, 004.9-Shigellosis unspecified, 006.3-amebic liver abscess, 008.42-intestinal infection due to pseudomonas, 008.45-intestinal infection due to Clostridium difficle, 008.63-Enteritis due to Norwalk Virus, 008.8-intestinal infection due to other organism not elsewhere classified, 009.0-infectious colitis enteritis and gastroenteritis, 009.1-colitis enteritis and gastroenteritis of presumed infectious origin, 011.90-unspecified pulmonary tuberculosis, 038.0-Streptococcal septicemia, 038.10-Staphylococcal septicemia unspecified, 038.11-Methicillin susceptible staphylococcus aureus septicemia, 038.12-Methicillin resistant staphylococcus aureus septicemia, 038.19-other Staphylococcal septicemia, 038.2-Pneumococcal septicemia, 038.3 – septicemia due to anaerobes, 038.40 – septicemia due to gram-negative organism unspecified, 038.41-septicemia due to Hemophilus influenzae, 038.42-septicemia due to Escherichia coli, 038.43-septicemia due to Pseuodomonas, 038.44-septicemia due to Serratia, 038.49-other septicemia due to gram-negative organisms, 038.8-other specified septicemias, 038.9-speticemia unspecified, 053.19-Herpes Zoster with other nervous system complications, 053.9-Herpes Zoster without complications, 054.79-Herpes simplex with other specified complications, 070.1-viral Hepatitis A without hepatic coma, 070.20-viral hepatitis B with hepatic coma acute or unspecified without hepatitis delta, 070.30-viral hepatitis B without hepatic coma acute or unspecified without hepatitis delta, 070.32-chronic viral hepatitis B without hepatic coma without hepatitis delta, 070.44-chornic hepatitis C with hepatic coma, 070.51-acute hepatitis C without mention of hepatic coma, 070.54-chronic hepatitis C without hepatic coma, 070.59-other specified viral hepatitis without hepatic coma, 070.70-unspecified viral hepatitis C without hepatic coma, 070.9-unspecified viral hepatitis without hepatic coma, 075-infectious mononucleosis, 078.5-cytomegaloviral disease, 079.99-unspecified viral infection, 094.89-other specified neurosyphilis , 112.2-candidiasis of other urogenital sites, 112.4-candidiasis of lung, 112.5-disseminated candidiasis, 112.84-candidal esophagitis, 114.9-Coccidiodomycosis unspecified, 117.3 Aspergillosis, 117.9-other and unspecified mycoses, 136.9-unspecified infectious and parasitic diseases, 202.13-mycosis fungoides involving intra-abdominal lymph nodes, 324.0-intracranial abscess, 357.0-acute infective polyneuritis, 421.0-acute and subacute bacterial endocarditis, 480.9-viral pneumonia unspecified, 481-pneumococcal pneumonia (Streptococcus pneumonia pneumonia), 482.0-pneumonia due to Klebsiella pneumoniae, 482.1-pneumonia due to Pseudomonas, 482.4-pneumonia due to Staphylococcus unspecified, 482.41-Methicillin susceptible pneumonia due to Staphylococcus aureus, 482.82-pneumonia due to Escherichia coli, 482.83-pneumonia due to other gram-negative bacteria, 482.84-pneumonia due to Legionnaires’ disease, 482.9-bacterial pneumonia unspecified, 485-bronchopneumonia organism unspecified, 486-pneumonia organism unspecified, 487.0-Influenza with pneumonia, 487.1-Influenza with other respiratory manifestations, 510.9-Empyema without fistula, 522.5-periapical abscess without sinus, 527.3-abscess of salivary gland, 540.0-acute appendicitis with generalized peritonitis, 540.1-acute appendicitis with peritoneal abscess, 540.9-acute appendicitis without peritonitis, 562.11-diverticulitis of colon without hemorrhage, 567.2-peritonitis (acute) generalized, 567.22-peritoneal abscess, 567.23-spontaneous bacterial peritonitis, 567.38-other retroperitoneal abscess, 569.61-infection of colostomy or enterostomy, 572.0-abscess of liver, 575.0-acute cholecystitis, 575.10-cholecystitis unspecified, 576.1-cholangitis, 590.10-acute pyelonephritis without lesion of renal medullary necrosis, 590.2-renal and perinephric abscess, 590.80-pyelonephritis unspecified, 599.0-urinary tract infection site not specified, 682.2-cellulitis and abscess of trunk, 682.6-cellulitis and abscess of leg except foot, 682.7-cellulitis and abscess of foot except toes, 682.3-cellulitis and abscess of upper arm and forearm, 682.5-cellulitis and abscess of buttock, 711.01-pyogenic arthritis involving shoulder region, 711.03-pyogenic arthritis involving forearm, 711.06-pyogenic arthritis involving lower leg, 730.08-acute osteomyelitis involving other specified sites, 730.18-chronic osteomyelitis involving other specified sites, 730.25-unspecified osteomyelitis involving pelvic region and thigh, 730.26-unspecified osteomyelitis involving lower leg, 730.27-unspecified osteomyelitis involving ankle and foot, 730.28-unspecified osteomyelitis involving other specified sites, 790.7-bacteremia, 995.92-severe sepsis, 996.61-infection and inflammatory reaction due to cardiac device implant and graft, 996.62-infection and inflammatory reaction due to other vascular device implant and graft, 996.63-infection and inflammatory reaction due to nervous system device implant and graft, 996.64-infection and inflammatory reaction due to indwelling urinary catheter, 996.65-infection and inflammatory reaction due to other genitourinary device implant and graft, 996.66-infection and inflammatory reaction due to internal joint prosthesis, 996.67-infection and inflammatory reaction due to other orthopedic device implant and graft, 996.69-infection and inflammatory reaction due to other internal prosthetic device implant and graft, 997.3-ventilator associated pneumonia, 997.62-infection (chronic) of amputation stump, 998.59-other postoperative infection |
| Pancreatitis | 577.0-acute pancreatitis, 577.1-chronic pancreatitis |
| Other | All remaining primary discharge codes. |
Footnotes
Competing interests: None
References
- 1.Lasman D, Hartman M, Washington B. et al. US Health spending trends by age and gender: selected years 2002 – 2010. Health Affairs. 2014;33:815–822. doi: 10.1377/hlthaff.2013.1224. [DOI] [PubMed] [Google Scholar]
- 2.Harness J K, Strodel W E, Talsma S E. Symptomatic biliary tract disease in the elderly patient. The American Surgeon. 1986;56:586–590. [PubMed] [Google Scholar]
- 3.Behlül B, Ayfer S, Vatansever S. et al. Safety of endoscopic retrograde cholangiopancreatography in patients 80 years of age and older. Przeglad Gastroenterologiczny. 2014;9:227–231. doi: 10.5114/pg.2014.45105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Everhart J E, Khare M, Hill M. et al. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. 1999;117:632–639. doi: 10.1016/s0016-5085(99)70456-7. [DOI] [PubMed] [Google Scholar]
- 5.Ali M, Ward G, Staley D. et al. A retrospective study of the safety and efficacy of ERCP in octogenarians. Digestive Diseases and Sciences. 2011;56:586–590. doi: 10.1007/s10620-010-1304-4. [DOI] [PubMed] [Google Scholar]
- 6.Lukens F J, Howell D A, Upender S. et al. ERCP in the very elderly; outcomes among patients older than eighty. Dig Dis Sci. 2010;55:847–851. doi: 10.1007/s10620-009-0784-6. [DOI] [PubMed] [Google Scholar]
- 7.Fritz E, Kirchgatterer A, Hubner D. et al. ERCP is safe and effective in patients 80 years of age and older compared with younger patients. Gastrointest Endosc. 2006;64:899–905. doi: 10.1016/j.gie.2006.05.010. [DOI] [PubMed] [Google Scholar]
- 8.Kim J E, Cha B H, Lee S H. et al. Safety and efficacy of endoscopic retrograde cholangiopancreatography in very elderly patients. Korean J Gastroenterol. 2011;57:237–242. doi: 10.4166/2011.57.4.237. [DOI] [PubMed] [Google Scholar]
- 9.Cho D H, Park G T, Oh J E. et al. A single institution’s experience of endoscopic retrograde cholangiopancreaticography in the elderly patients: outcomes, safety, and complications. Korean J Gastroenterol. 2011;58:88–92. doi: 10.4166/kjg.2011.58.2.88. [DOI] [PubMed] [Google Scholar]
- 10.Katsinelos P, Kountouras J, Chatzimavroudis G. et al. Outpatient therapeutic endoscopic retrograde cholangiopancreatography is safe in patients aged 80 years and older. Endoscopy. 2011;43:128–133. doi: 10.1055/s-0030-1255934. [DOI] [PubMed] [Google Scholar]
- 11.Elixhauser A, Steiner C, Harris D R. et al. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. doi: 10.1097/00005650-199801000-00004. [DOI] [PubMed] [Google Scholar]
- 12.Grendar J, Shaheen A A, Myers R P. et al. Predicting in-hospital mortality in patients undergoing complex gastrointestinal surgery: determining the optimal risk adjustment method. Arch Surg. 2012;147:126–135. doi: 10.1001/archsurg.2011.296. [DOI] [PubMed] [Google Scholar]
- 13.Varadarajulu S, Kilgore M L, Wilcox C M. et al. Relationship among hospital ERCP volume, length of stay, and technical outcomes. Gastrointest Endosc. 2006;64:338–347. doi: 10.1016/j.gie.2005.05.016. [DOI] [PubMed] [Google Scholar]
- 14.Masci E, Toti G, Mariani A. et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417–423. doi: 10.1111/j.1572-0241.2001.03594.x. [DOI] [PubMed] [Google Scholar]
- 15.Vandervoort J, Soetikno R M, Tham T C. et al. Risk factors for complications after performance of ERCP. Gastrointest Endosc. 2002;56:652–656. doi: 10.1067/mge.2002.129086. [DOI] [PubMed] [Google Scholar]
- 16.Yun D Y, Han J, Oh J S. et al. Is endoscopic retrograde cholangiopancreatography safe ub oatuebts 90 years of age and older? Gut Liver. 2014;8:552–556. doi: 10.5009/gnl13310. [DOI] [PMC free article] [PubMed] [Google Scholar]