

Shigellosis trends in these communities provide insight into global movement of drug-resistant Enterobacteriaceae.
Keywords: Shigella sonnei, shigellosis, Enterobacteriaceae, bacteria, enteric infections, diarrhea, dysentery, gastroenteritis, antimicrobial resistance, Jewish orthodox, Israel, Europe, France, Belgium, United States, Canada
Abstract
Shigellae are sensitive indicator species for studying trends in the international transmission of antimicrobial-resistant Enterobacteriaceae. Orthodox Jewish communities (OJCs) are a known risk group for shigellosis; Shigella sonnei is cyclically epidemic in OJCs in Israel, and sporadic outbreaks occur in OJCs elsewhere. We generated whole-genome sequences for 437 isolates of S. sonnei from OJCs and non-OJCs collected over 22 years in Europe (the United Kingdom, France, and Belgium), the United States, Canada, and Israel and analyzed these within a known global genomic context. Through phylogenetic and genomic analysis, we showed that strains from outbreaks in OJCs outside of Israel are distinct from strains in the general population and relate to a single multidrug-resistant sublineage of S. sonnei that prevails in Israel. Further Bayesian phylogenetic analysis showed that this strain emerged approximately 30 years ago, demonstrating the speed at which antimicrobial drug–resistant pathogens can spread widely through geographically dispersed, but internationally connected, communities.
Antimicrobial-resistant (AMR) Enterobacteriaceae are recognized as a global public health threat (1,2). Understanding the emergence of these pathogens and tracking transmission across international borders is vital for informing public health surveillance, intervention, and management (3). Shigella spp. are Enterobacteriaceae that cause severe, acute diarrhea resulting in mortality rates second only to rotaviruses as known agents of diarrheal disease (4). Shigellae cause disease in both low- and high-income nations (5), and >10 organisms can initiate disease (6). Shigellae are also increasingly resistant to antimicrobial drugs (7–10). Because of the large global burden of shigellosis, the low infective dose, highly visible disease syndrome, and ability to acquire AMR, shigellae are a relevant and sensitive indicator species for studying trends in the global transmission and emergence of AMR enteric bacteria.
Of the recognized Shigella spp., the distribution of S. sonnei makes it particularly relevant for studying international transmission because it is the most commonly isolated species in middle- to high-income nations (5) and causes a substantial disease incidence in low-income nations; for example, 23.7% of all documented shigellosis cases causing moderate to severe diarrhea in children <5 years of age in Africa and Asia (11). Moreover, S. sonnei prevalence increases as nations develop economically (12–15). To examine the underlying processes of such broad epidemiologic phenomena over medium- to long-term scales in bacterial populations, robust, high-resolution molecular subtyping is used. Subtyping of S. sonnei by using whole-genome sequencing has defined a global population structure that is divided into 4 lineages; the third lineage, global III, disseminated globally after acquiring multidrug resistance (MDR) (16). This advanced subtyping and established global context was used to show that the rise of S. sonnei in Vietnam was attributable to the point introduction and subsequent expansion of a single sublineage in the 1980s (17), demonstrating the effectiveness of this approach for characterizing epidemiologic phenomena.
Similarly, assessing the global burden of a widespread pathogen such as S. sonnei calls for use of a patient group in which the effects of illness are international. One such risk group for S. sonnei is Orthodox Jewish communities (OJCs) (5). These communities are highly susceptible to shigellosis because of densely populated living conditions, high numbers of young children per family, and intracommunity transfer facilitated by large holiday gatherings (18–20). S. sonnei shigellosis is highly endemic to Israel; its incidence there since the early 1990s has primarily been driven by biennial epidemics within OJCs in Israel (primarily in the 0–4-year age group, in whom the incidence is ≈7 cases/1,000 population/y [19]). In addition to incidence in OJCs in Israel, outbreaks ranging in size from 27 culture-confirmed cases to >13,000 cases of S. sonnei shigellosis have been reported in OJCs in Europe and North America (18,20–24). These outbreaks are attributable to highly clonal organisms, determined by using pulsed-field gel electrophoresis (20,22,24) and, in the case of an outbreak in Belgium, linked to prevailing strains from Israel (22). Thus, characterizing the international connectivity of OJC-associated S. sonnei represents an opportunity to assess the effects of travel- and community-based associations on the transmission of AMR Enterobacteriaceae.
We generated whole-genome sequences from >400 clinical isolates of S. sonnei collected over 22 years from OJCs within Israel, OJCs outside of Israel, and non-OJCs in the United Kingdom. We then combined these data with the established genomic global context for S. sonnei. By analyzing phylogenetic relationships, we investigated the distinction of strains from OJC outbreaks from other locally circulating strains (i.e., among non-OJCs) and explored the possible epidemiologic relationship of outbreaks in OJCs outside of Israel and endemic shigellosis in Israel. We also sought to determine the relationship of these epidemiologic processes with AMR determinants in S. sonnei.
Materials
We performed whole-genome sequencing on 437 S. sonnei isolates as part of this study. These isolates were from patients associated with OJCs outside of Israel (n = 171), from 221 patients in Israel (200 OJC, 21 of unknown ethnicity), or from patients in the United Kingdom not associated with OJCs (n = 45) (Technical Appendix 1). The isolates were collected from 6 countries (Israel, the United Kingdom, France, Belgium, the United States, and Canada) during 1992–2014 (Figure 1). The collection included isolates from most previously reported OJC-associated outbreaks of S. sonnei shigellosis; we defined cases as being OJC-associated separately for each public health agency (Table 1).
Figure 1.
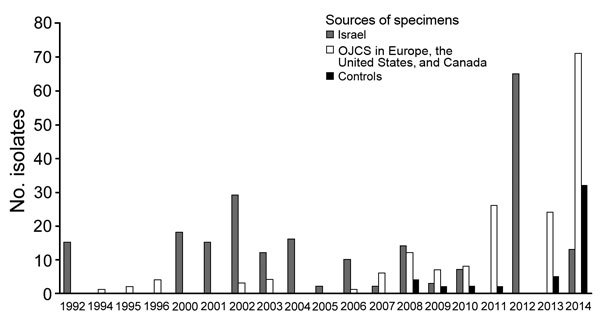
Origin and year of collection for 437 clinical isolates collected and sequenced from different countries and patient communities as part of study of travel- and community-based transmission of multidrug-resistant Shigella sonnei among international OJCs. Non-OJC samples were isolated from samples in the United Kingdom that were phage-type and temporally matched to isolates from OJCs in the United Kingdom (Technical Appendix 2 Figure 1). OJCs, Orthodox Jewish communities.
Table 1. Origins of Shigella sonnei isolates used to track travel- and community-based transmission of multidrug-resistant Shigella sonnei among international Orthodox Jewish communities* .
| Region/community | Country | Year(s) | Details | References | No. isolates |
|---|---|---|---|---|---|
| Europe OJCs | Belgium | 2008 | Outbreak | (22) | 3 |
| France | 1996–2014 | Multiple outbreaks | This study, (21) | 64 | |
|
|
United Kingdom |
2006–2014 |
Multiple outbreaks |
This study, (23) |
101 |
| Europe non-OJCs |
United Kingdom |
2008–2014 |
Matched (time and phage-type) non-OJC
cases |
This study |
45 |
| United States and Canada
OJCs |
United States |
1994–1995 |
Outbreak |
(24) |
3 |
| Israel† |
Israel |
2000–2014 |
Sentinel laboratory surveillance |
This study, (19) |
221 |
| Global context |
Multiple |
1943–2008 |
Used for background |
(16) |
118 |
| Total |
555 |
||||
| *OJC, Orthodox Jewish communities. †90% known OJC ethnicity. | |||||
Samples from Israel
The 221 samples of S. sonnei in Israel were collected during 1992–2014 in local hospital and health maintenance organization laboratories, including the national sentinel laboratory-based surveillance program (19). As described by Cohen et al. (19), 90% of the S. sonnei shigellosis isolates collected in Israel are from Jewish patients, and the isolates from Israel sequenced in this study were primarily (n = 200, 90%) derived from OJCs (Technical Appendix 2 Table 1).
Samples from Outside of Israel
United Kingdom
A total of 146 S. sonnei samples were used from the Gastrointestinal Bacteria Reference Unit at Public Health England (London, United Kingdom). These samples included 22 from a small OJC-associated outbreak (23) and an additional 79 from outbreaks during 2006–2014 that were epidemiologically confirmed to be associated with OJCs by interviews and questionnaires as part of public health investigations. Also included were a set of 45 isolates from patients with no known OJC association (non-OJC). These background isolates were contemporaneously collected and selected on the basis of phage typing; that is, including diverse phage types, but focused on representing phage types associated with OJC outbreaks (Technical Appendix 2 Figure 1).
France
A total of 64 isolates from OJC-associated outbreaks in France (21) were submitted to the French National Reference Center for E. coli, Shigella, and Salmonella at the Pasteur Institute collected during 1996–2014. These isolates included those from a small OJC-associated outbreak in 2007 (21).
Belgium
Three S. sonnei isolates were provided from Belgium. These isolates were collected during a small OJC-associated outbreak in Antwerp in 2008 (22).
United States and Canada
Three representative isolates were collected during a large, homogenous, OJC-associated outbreak of S. sonnei. This outbreak occurred across the United States and Canada during 1994–1996 (24).
Comparison Dataset
We analyzed the clinical isolates of S. sonnei alongside an existing global dataset compiled by KE Holt et al. (n = 118) (Technical Appendix 1) (16). In brief, this global context dataset comprises temporally (collected during 1943–2008, 70% collected after 1992) and geographically diverse (from 4 continents) S. sonnei isolates previously used to define the population structure of this pathogen. The dataset includes 1 sample collected in Israel in 2003.
Methods
DNA was extracted at multiple sites by using the Wizard genomic DNA extraction kit (ProMega, Madison, WI, USA) according to manufacturer’s instructions. DNA was sequenced by using the MiSeq and HiSeq 2000 platforms (Illumina, San Diego, CA, USA) at multiple institutes according to in-house protocols (Technical Appendix 1) (25–27). Sequencing data for all isolates described passed internal quality control and were assembled into <687 contiguous sequences with a total length of <5.0 MB. Sequence data are available in the European Nucleotide Archive (http://www.ebi.ac.uk/ena; accession numbers in Technical Appendix 2).
Analysis of sequencing data was similar to that previously described (28). Multiple sequence alignment for phylogenetic analysis was generated by mapping to reference isolate S. sonnei Ss046 (GenBank accession no. CP000038), then masking mobile and repetitive elements (16) and stripping sites of recombination (29). Analysis of remaining variable sites was performed by using maximum-likelihood analysis in RAxML version 7.8.6 to create phylogenetic trees (30).
For isolates in the OJC-associated lineage for which the sampling date was known (n = 333; Technical Appendix 1), BEAST version 1.8 software (http://beast.bio.ed.ac.uk/) was used to estimate the emergence date of the lineage (31). Root-to-tip distances were generated by using Path-O-Gen version 1.4 (32). BEAST results shown are from 4 chains of 100 million Markov chain Monte Carlo generations run according to a general time reversible plus gamma substitution model, with a relaxed normal clock and Bayesian Skyline Population model, previously used for this pathogen (16,17). Chains were sampled every 1,000 generations with a 10% initial burn-in for root-height (time to most recent common ancestor) analysis. The maximum clade credibility tree was generated with a 10% burn-in and sampling every 100,000 generations. These results were consistent with those generated similarly by using a constant population growth model (Technical Appendix 2 Table).
De novo assembly, annotation, and antimicrobial resistance gene detection in the isolates was done as previously described (28) (accession numbers for annotated draft genome assemblies in Technical Appendix 1). Contiguous sequences containing antimicrobial resistance genes were extracted from assemblies and the presence of plasmid incompatibility groups on these contiguous sequences was determined by using PlasmidFinder (33). The presence of the Tn7/Int2 cassette was confirmed by mapping, and synteny detected by using ACT (34).
Results
To determine the relationships among S. sonnei from OJCs inside and outside of Israel, we constructed a phylogenetic tree including whole-genome sequence data from 437 isolates of S. sonnei alongside the 118 isolates from the global context dataset (Table 1; Figure 2). This analysis showed the existence of a large, unique monophyletic sublineage (n = 396 isolates) of the global III lineage that was almost exclusively (388/396, 98%) composed of isolates from OJC-associated outbreaks and samples from persons in Israel (OJC-associated lineage; Figure 2; Technical Appendix 2 Figure 2). This lineage contained nearly all isolates (217/221, 98%) sequenced from Israel and collected during1992–2014 (Figure 2); 170/171 (99%) of those identified from samples collected during the same time frame from OJCs in the United States, Canada, France, Belgium, and the United Kingdom; and the 1 isolate from the global context dataset that originated in Israel (Figure 2; Technical Appendix 1). The clustering of most (387/392, 99%) of the strains from Israel and the other OJC-associated strains in the OJC-associated lineage is remarkable considering that the lineage represented approximately 10% of the diversity of the S. sonnei: the largest intra-lineage pairwise distance was 8.8-fold less in the OJC-associated lineage relative to the remainder of the tree (Figure 2).
Figure 2.
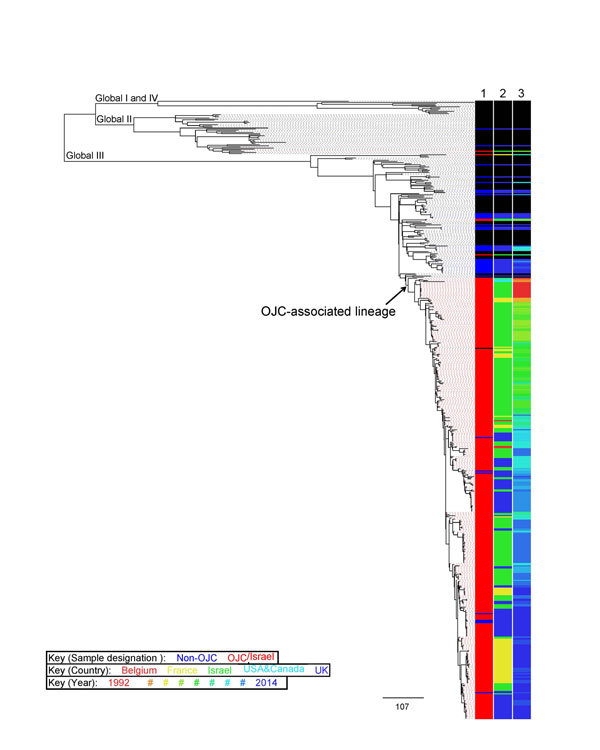
The OJC-associated lineage of multidrug-resistant Shigella sonnei in context with other global lineages. These background (non-OJC) isolates were contemporaneously collected and selected on the basis of phage typing; that is, including diverse phage types, but focused on representing phage types associated with OJC outbreaks. The midpoint rooted maximum-likelihood phylogenetic tree shows the relationships of 437 sequences from study of travel- and community-based transmission of multidrug-resistant S. sonnei among international OJCs compared with 118 isolates from a global context database of previously defined lineages of S. sonnei. Lineages are labeled along branches. Adjacent tracks are colored according to the inlaid key and show epidemiologic features of the isolate (lane 1, sample designation; lane 2, country; lane 3, year of isolation). Year of isolation is colored on a continuous heat map scale for 1992–2014, shown by hash symbols (#). Scale bar indicates single-nucleotide polymorphisms. OJCs, Orthodox Jewish communities.
The inclusion of isolates from patients in the United Kingdom that were not associated with OJCs provided further illumination of the association of this lineage with OJCs. These non-OJC samples were almost entirely (37/45, 82%) located outside the OJC-associated lineage, distributed elsewhere in the global III and II lineages (Figure 2). Ultimately, this resulted in a statistically significant association of lineage with sample designation (i.e., OJC or non-OJC) among UK isolates (p<0.0001 by Fisher exact test). This association correlated better with phylogenetic position than phage type, which was a comparatively poor indicator of genome level phylogeny (Technical Appendix 2 Figure 3). The relative phylogenetic positions of non-OJC and OJC isolates from the United Kingdom when viewed in an international context, i.e., including the other strains (Figure 2) showed that strains from UK OJCs were more likely to be related to strains from Israel than to strains circulating in non-OJCs. For example, strains from OJCs sampled in the United Kingdom in 2014 were phylogenetically adjacent to strains from Israel sampled in 2014, rather than to non-OJC strains sampled in the United Kingdom in 2014 (Figure 2.)
Consistent with this finding, phylogenetic relationships within the OJC-associated lineage were defined more by time than geography (Figure 2; Technical Appendix 2 Figures 2, 4) Bayesian phylogenetic analysis showed that the OJC-associated lineage emerged in 1988 (95% highest posterior distribution 1985–1990) (Figure 3). Since that time, contemporaneously collected isolates were phylogenetically proximate with subsequent evolution, resulting in strain replacement rather than coexistence over time (Figure 3; Technical Appendix 2 Figure 2). Contrasting with the clear time signature in the lineage, geographic admixing of isolates occurred within the lineage (Figure 3). For example, >5 and 7 monophyletic clusters of isolates from OJC-associated outbreaks in France and the United Kingdom, respectively, were encompassed within the diversity of strains characterized in Israel (Figure 3). Samples from a single epidemiologic OJC-associated outbreak in Belgium were separated from each other by 44 single-nucleotide polymorphisms, making them phylogenetically distinct (Figure 2; Technical Appendix 2 Figure 2). This finding is consistent with contemporaneous OJC-associated outbreaks in different geographic areas representing real-time transmission events.
Figure 3.
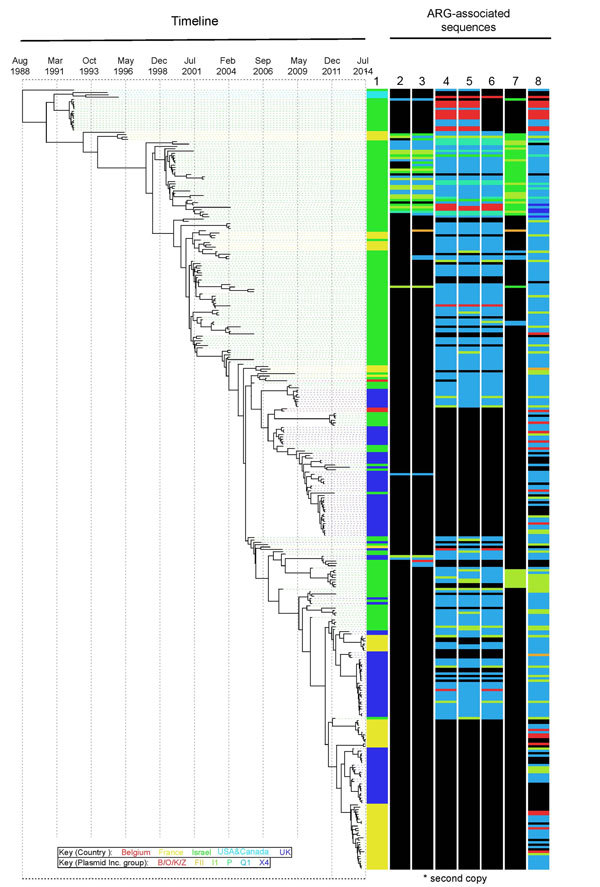
The OJC-associated lineage of multidrug-resistant Shigella sonnei across time and associated antimicrobial drug resistance. The Bayesian-inferred phylogenetic tree shows the evolutionary relationships of 333 isolates (those for which a fixed date was available) in the OJC-associated lineage since its emergence in the late 1980s. Tree tips overlay the collection date of the isolates. Lane 1 at right shows the country of origin (colors shown in key), and subsequent tracks show the plasmid incompatibility groups (colors shown in key) of contiguous sequences carrying the named antimicrobial resistance genes in that isolate: lane 2, aadA1 (second copy); lane 3, sul1; lane 4, strA; lane 5, strB; lane 6, sul2; lane 7, tetA; lane 8, blaTEM. Black indicates gene not detected. The aadA1 genes described in this figure are in addition to the copy carried by all isolates in the OJC-associated lineage on the Tn7/Int2 cassette described in Results. OJCs, Orthodox Jewish communities.
Because of the potential consequences of this intercontinental transmission to the transfer of AMR to S. sonnei, we determined the AMR characteristics of the OJC-associated lineage. We found that the lineage had a unique AMR profile relative to isolates outside of the OJC-associated lineage (Table 2). The OJC-associated lineage belonged to the global III lineage of S. sonnei, and every isolate in the OJC-associated lineage contained a Tn7/Int2 cassette that encoded the MDR thought to have facilitated the global dispersal of global III (16). This cassette contains the aadA1, sat2, and dfrA1 genes that confer resistance to aminoglycosides, streptothricin, and trimethoprim and was chromosomally integrated adjacent to the glmS gene in these isolates (indicating a single acquisition event). This region is identical to a Tn7-like island, also adjacent to the glmS gene, in the newly emerging Xv serotype of S. flexneri (reference strain 2002017 [35]; Technical Appendix 2 Figure 5). No mutations known to confer quinolone resistance were found in gyrA or parC sequences of isolates in the OJC-associated lineage, and no plasmid-encoded quinolone resistance genes were detected (Technical Appendix 1).
Table 2. Antimicrobial resistance determinants among isolates isolates sequenced in study of travel- and community-based transmission of multidrug-resistant Shigella sonnei among international OJCs*.
| Antimicrobial resistance determinant | Within OJC-associated lineage, n = 395 | Outside OJC-associated lineage, n = 42 |
|---|---|---|
| bl2d_oxa1 | 0.00 | 0.02 |
| catA1 | 0.00 | 0.02 |
| tetB | 0.00 | 0.05 |
| dfrA5 | 0.00 | 0.07 |
| bl2b_tem | 0.00 | 0.00 |
| dfrA16 | 0.00 | 0.00 |
| aac3iia | 0.01 | 0.00 |
| dfrA17 | 0.01 | 0.00 |
| bl2b_tem1 | 0.01 | 0.00 |
| mphA | 0.02 | 0.00 |
| dfrA14 | 0.03 | 0.02 |
| sul1 | 0.12 | 0.07 |
| tetA | 0.18 | 0.79 |
| strB | 0.53 | 0.88 |
| sul2 | 0.53 | 0.90 |
| strA | 0.53 | 0.88 |
| arnA | 0.95 | 0.95 |
| mdtP | 0.97 | 1.00 |
| mdtO | 0.97 | 0.98 |
| mdtN | 0.97 | 1.00 |
| bacA | 0.99 | 0.98 |
| emrE | 0.99 | 1.00 |
| mdfA | 0.99 | 1.00 |
| mdtK | 0.99 | 1.00 |
| aadA1 | 0.99 | 0.81 |
| macB | 0.99 | 0.98 |
| mdtL | 0.99 | 0.98 |
| mdtE | 0.99 | 1.00 |
| mdtF | 0.99 | 1.00 |
| mdtG | 1.00 | 1.00 |
| mdtH | 1.00 | 1.00 |
| dfrA1 | 1.00 | 0.90 |
| acrA | 1.00 | 1.00 |
| acrB | 1.00 | 1.00 |
| bcr | 1.00 | 1.00 |
| bl1_ec | 1.00 | 1.00 |
| ksgA | 1.00 | 1.00 |
| tolC | 1.00 | 1.00 |
| blaTEM† | 0.86 | 0.14 |
*Excludes global context isolates. OJC-associated lineage defined in Technical Appendix Figure 1 (http://wwwnc.cdc.gov/EID/22/9/15-1953-Techapp1.pdf). OJC, Orthodox Jewish communities. †Detected separately.
To consider AMR mechanisms that had potential to mobilize among bacteria, we further examined antimicrobial resistance genes that were inconsistently present (in 5%–95% of isolates) (Figure 3; Technical Appendix 1; Technical Appendix 2 Figure 2). The 7 genes found to be inconsistently present across the lineage were second copies of aadA1 present in some isolates; the aminoglycoside resistance–conferring strA and strB genes; the sulphonamide resistance genes sul1 and sul2; the tetracycline resistance gene tetA; and the ampicillin resistance gene blaTEM (Figure 3; Technical Appendix 2 Figure 2). Attempts were made to determine the coinheritance and genetic carriage elements of these genes (within the limitations of genome assembly). In isolates that had additional copies of aadA1, the gene was typically co-inherited with the sul1 gene (Figure 3; Technical Appendix 1; Technical Appendix 2 Figure 2); this combination was found on plasmids of 2 different incompatibility groups, I1 and P, as well as on contiguous sequences where no plasmid incompatibility groups were identified, shown as unknown (Figure 3; Technical Appendix 2 Figure 2). Similarly, strA, strB, and sul2 were frequently co-inherited and found on plasmids of 4 different incompatibility groups. Isolates collected earlier in the lineage’s evolution tended to carry strA/strB/sul2 on B/O/K/Z, Q1, and P incompatibility group plasmids, whereas later isolates carried the genes on I1 plasmids (Figure 3; Technical Appendix 2 Figure 2). Similarly, the tetA gene appeared to have had 2 major introductions into the lineage, earlier on a P group plasmid and later on an I1 plasmid (Figure 3; Technical Appendix 2 Figure 2). Last, blaTEM genes were found in 86% of isolates in the lineage, compared with 14% outside of the lineage (Table 2; Technical Appendix 1); these genes were carried on plasmids of 5 different incompatibility groups, with sporadic coinheritance patterns with other resistance genes (Figure 3; Technical Appendix 2 Figure 2).
Discussion
We used whole-genome sequencing to develop a high-resolution picture of the international transmission of S. sonnei and its AMR determinants among OJCs over several decades. These analyses offer insight for the epidemiology of shigellosis inside and outside of Israel as well as for the broader transmission of AMR enteric pathogens. We showed that, in countries outside of Israel, outbreak strains in OJCs were distinct from strains circulating in the general population and that OJC-associated strains were more closely affiliated with outbreaks associated with OJCs in other countries (irrespective of geographic distance) and strains circulating in Israel. Strains from Israel and strains from nearly all previously reported OJC outbreaks elsewhere formed a distinct OJC-associated sublineage that emerged ≈30 years ago. Unlike other described emergent Shigella sublineages (17,28), the OJC-associated lineage lacked a defining association with AMR.
Isolates collected during outbreaks of S. sonnei in OJCs outside Israel were phylogenetically linked to contemporaneous isolates from Israel. This finding was suspected from previous studies that used pulsed-field gel electrophoresis, the results of which supported that samples from outbreaks among OJCs in the United States and Belgium were distinct from samples of S. sonnei circulating locally in non-OJCs (22,24) and were related to strains from Israel (22). We confirmed this link in an analysis of specimens collected in the United Kingdom that showed that strains from OJC-associated outbreaks were distinct from other circulating strains in that country but related to contemporaneous strains from Israel (Figure 2). The broader analysis, expanded in time and geography, showed that local epidemics in OJCs in France, Belgium, and North America (21,22,24) were also linked with contemporaneous isolates from Israel (Figure 3; Technical Appendix 2 Figure 2). This pattern of phylogenetic clustering by community affiliation was also recently demonstrated for S. flexneri 3a strain transmission among a global epidemiologic community of men who have sex with men, through which a unique MDR sublineage spread during ≈20 years (28). These studies demonstrate the speed with which AMR Enterobacteriaceae can be transmitted among persons in an internationally linked community rather than by contiguous geographic spread.
These findings also have implications for the epidemiology of shigellosis within Israel. The isolates from Israel in this study derive primarily from OJCs, which drive cyclic S. sonnei epidemics in Israel (19); here, they were shown to belong to a single, low-diversity sublineage. The lineage was monophyletic and had a strong time signature, consistent with a point introduction and subsequent epidemic emergence. This pattern was similar to that observed in Vietnam after the introduction of another global III S. sonnei sublineage (15,17). The date of the emergence of the OJC-associated lineage (1988 [95% highest posterior distribution 1985–1990]) is consistent with that estimated in a previous study where a 2-isolate lineage emerged in the Middle East during 1983 (16). Considering the timing and context of the emergence, it is possible that the OJC-associated lineage emerged from the large waterborne epidemic that occurred in Israel in the mid-1980s (19) or was potentially introduced from the first reported OJC-associated outbreak of shigellosis outside of Israel, which was an outbreak of >13,000 cases across the United States that also occurred in the 1980s (18). Samples from this period were not available to explore these origins of these outbreaks, but it is clear that the OJC-associated lineage is now endemic to OJCs in Israel and is causative of OJC-associated outbreaks elsewhere.
The AMR profile of the OJC-associated lineage is consistent with the phenotypic information and is likely influenced by antimicrobial resistance selection pressures in the 0–4-year age group, which is primarily affected by shigellosis in OJCs. Sulfonamide and tetracycline resistance determinants were in flux across the lineage (Figure 3), and these antimicrobial classes have been reported as being phenotypically dynamic over time among S. sonnei isolated in Israel (19). Furthermore, trimethoprim resistance was chromosomally encoded in all isolates, and plasmid-mediated ampicillin resistance was a common finding (86% of isolates) (Figure 3). These antimicrobial classes are key for the treatment of children with shigellosis. Similarly, resistance to tetracyclines, which can be used in children >7 years of age (8), and macrolides (mphA gene [21]) (Table 2) were also found. Despite being reported in other global III S. sonnei strains (16,17), resistance to quinolones was not found in the OJC-associated lineage, possibly because the use of quinolones is contraindicated in children.
The acquisition of the Tn7/Int2-encoded MDR in this lineage may have facilitated its epidemic emergence, as has been hypothesized for the broader global III lineage (16) and as is possible for S. flexneri Xv (35), although these possibilities cannot be explored fully by using these data. The presence of this gene cassette throughout the lineage and other phylogenetic clusters of antimicrobial resistance genes demonstrates that AMR can spread through this geographically dispersed, but closely associated, community. However, in contrast to the emergence of S. flexneri 3a among men who have sex with men or of S. sonnei in Vietnam, further acquisition of AMR does not appear to have shaped the subsequent evolution of the lineage. The presence of additional resistance genes (Figure 3) was not correlated with later time points, and the same genes were carried on distinct mobile genetic elements, consistent with sporadic reintroduction, rather than maintenance of the additional resistance genes in the population. This absence of a defining association with AMR suggests that it is probably primarily the epidemiologic suitability of OJCs to the transmission of S. sonnei that supports its maintenance in these communities. This likelihood is consistent with previous studies of OJC-associated shigellosis, which suggest that transmission is largely driven by communal childcare arrangements in a host population that is young and densely structured (19,20,22).
This study documents the speed with which MDR enteric bacteria can transmit intercontinentally through travel within a geographically dispersed, but closely linked, community. Awareness of this mode of sustained, geographically noncontiguous transmission must inform public health practice, including targeted control and reduction of consequences of the pathogen through developing effective relationships with affected communities; identifying specific risk factors; and designing, piloting, and eventually implementing specific culturally appropriate interventions with the participation and support of the community while avoiding stigmatization. Effective ongoing surveillance is also vital, and we demonstrated the resolution required for that purpose and the need for effective data sharing to track these otherwise silent transmission phenomena. Furthermore, the repeated application of high-resolution tools supports identification of parallels and contrasts with previous genomic epidemiology studies, supporting construction of a complete picture of the global transmission of AMR enteric pathogens, advancing our position for tackling this global public health issue.
Sample details for isolates of Shigella sonnei used in this study and reference strains from global context database.
Supporting data and phylogenetic and genetic characteristics of isolates of Shigella sonnei.
Acknowledgments
We thank David Harris and WTSI sequencing and informatics teams for coordinating sample management, sequencing, and automated analyses.
K.S.B. is in receipt of a Wellcome Trust Postdoctoral Training Fellowship for Clinicians (106690/A/14/Z) and all WTSI authors are supported by Wellcome Trust grant number 098051. This study was also aided by the European Union Seventh Framework Programme (FP7/2007–2013) under grant agreement 261472 ‘STOPENTERICS’. The French National Reference Center for E. coli, Shigella and Salmonella is co-funded by the Institut de Veille Sanitaire. The Unité des Bactéries Pathogènes Entériques belongs to the Integrative Biology of Emerging Infectious Diseases Laboratory of Excellence funded by the French Government Investissement d’Avenir programme (grant no. ANR-10-LABX-62-IBEID).
Biography
Dr. Baker is a veterinarian researcher working as a research fellow at the Wellcome Trust Sanger Institute and the University of Liverpool and has also been awarded a Wellcome Trust Postdoctoral Clinical Research Training Fellowship. Her research interests include genomic epidemiology of enteric pathogens and the dynamics of antimicrobial resistance in bacterial populations.
Footnotes
Suggested citation for this article: Baker KS, Dallman TJ, Behar A, Weill FX, Gouali M, Soble J, et al. Travel- and community-based transmission of multidrug-resistant Shigella sonnei lineage among international Orthodox Jewish communities. Emerg Infect Dis. 2016 Sep [date cited]. http://dx.doi.org/10.3201/eid2209.151953
References
- 1.World Health Organization. WHO Global strategy for containment of antimicrobial resistance. Switzerland: The Organization; 2001. [Google Scholar]
- 2.Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Atlanta: US Department of Health and Human Services; 2013 [cited 2016 May 26]. http://www.cdc.gov/drugresistance/threat-report-2013/index.html
- 3.van der Bij AK, Pitout JD. The role of international travel in the worldwide spread of multiresistant Enterobacteriaceae. J Antimicrob Chemother. 2012;67:2090–100. 10.1093/jac/dks214 [DOI] [PubMed] [Google Scholar]
- 4.GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–71. 10.1016/S0140-6736(14)61682-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kotloff KL, Winickoff JP, Ivanoff B, Clemens JD, Swerdlow DL, Sansonetti PJ, et al. Global burden of Shigella infections: implications for vaccine development and implementation of control strategies. Bull World Health Organ. 1999;77:651–66. [PMC free article] [PubMed] [Google Scholar]
- 6.Kothary MH, Babu US. Infective dose of foodborne pathogens in volunteers: a review. J Food Saf. 2001;21:49–68. 10.1111/j.1745-4565.2001.tb00307.x [DOI] [Google Scholar]
- 7.Vinh H, Baker S, Campbell J, Hoang NV, Loan HT, Chinh MT, et al. Rapid emergence of third generation cephalosporin resistant Shigella spp. in Southern Vietnam. J Med Microbiol. 2009;58:281–3. 10.1099/jmm.0.002949-0 [DOI] [PubMed] [Google Scholar]
- 8.Ashkenazi S, Levy I, Kazaronovski V, Samra Z. Growing antimicrobial resistance of Shigella isolates. J Antimicrob Chemother. 2003;51:427–9. 10.1093/jac/dkg080 [DOI] [PubMed] [Google Scholar]
- 9.Kuo CY, Su LH, Perera J, Carlos C, Tan BH, Kumarasinghe G, et al. Antimicrobial susceptibility of Shigella isolates in eight Asian countries, 2001–2004. J Microbiol Immunol Infect. 2008;41:107–11. [PubMed] [Google Scholar]
- 10.Vrints M, Mairiaux E, Van Meervenne E, Collard JM, Bertrand S. Surveillance of antibiotic susceptibility patterns among Shigella sonnei strains isolated in Belgium during the 18-year period 1990 to 2007. J Clin Microbiol. 2009;47:1379–85. 10.1128/JCM.02460-08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Livio S, Strockbine NA, Panchalingam S, Tennant SM, Barry EM, Marohn ME, et al. Shigella isolates from the global enteric multicenter study inform vaccine development. Clin Infect Dis. 2014;59:933–41 . 10.1093/cid/ciu468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bangtrakulnonth A, Vieira AR, Lo Fo Wong DM, Pornreongwong S, Pulsrikarn C, Sawanpanyalert P, et al. Shigella from humans in Thailand during 1993 to 2006: spatial-time trends in species and serotype distribution. Foodborne Pathog Dis. 2008;5:773–84. 10.1089/fpd.2008.0109 [DOI] [PubMed] [Google Scholar]
- 13.Qiu S, Xu X, Yang C, Wang J, Liang B, Li P, et al. Shift in serotype distribution of Shigella species in China, 2003–2013. Clin Microbiol Infect. 2015;21:252.e5–8 . 10.1016/j.cmi.2014.10.019 [DOI] [PubMed] [Google Scholar]
- 14.Banga Singh KK, Ojha SC, Deris ZZ, Rahman RA. A 9-year study of shigellosis in Northeast Malaysia: antimicrobial susceptibility and shifting species dominance. J Public Health (Bangkok). 2011;19:231–6. 10.1007/s10389-010-0384-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vinh H, Nhu NT, Nga TV, Duy PT, Campbell JI, Hoang NV, et al. A changing picture of shigellosis in southern Vietnam: shifting species dominance, antimicrobial susceptibility and clinical presentation. BMC Infect Dis. 2009;9:204. 10.1186/1471-2334-9-204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Holt KE, Baker S, Weill FX, Holmes EC, Kitchen A, Yu J, et al. Shigella sonnei genome sequencing and phylogenetic analysis indicate recent global dissemination from Europe. Nat Genet. 2012;44:1056–9. 10.1038/ng.2369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Holt KE, Thieu Nga TV, Thanh DP, Vinh H, Kim DW, Vu Tra MP, et al. Tracking the establishment of local endemic populations of an emergent enteric pathogen. Proc Natl Acad Sci U S A. 2013;110:17522–7. 10.1073/pnas.1308632110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Centers for Disease Control and Prevention. Multistate outbreak of Shigella sonnei gastroenteritis—United States. MMWR Morb Mortal Wkly Rep. 1987;36:440–2, 448–9. [PubMed] [Google Scholar]
- 19.Cohen D, Bassal R, Goren S, Rouach T, Taran D, Schemberg B, et al. Recent trends in the epidemiology of shigellosis in Israel. Epidemiol Infect. 2014;142:2583–94. 10.1017/S0950268814000260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Garrett V, Bornschlegel K, Lange D, Reddy V, Kornstein L, Kornblum J, et al. A recurring outbreak of Shigella sonnei among traditionally observant Jewish children in New York City: the risks of daycare and household transmission. Epidemiol Infect. 2006;134:1231–6. 10.1017/S0950268806006182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Boumghar-Bourtchai L, Mariani-Kurkdjian P, Bingen E, Filliol I, Dhalluin A, Ifrane SA, et al. Macrolide-resistant Shigella sonnei. Emerg Infect Dis. 2008;14:1297–9. 10.3201/eid1408.080147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.De Schrijver K, Bertrand S, Gutierrez Garitano I, Van den Branden D, Van Schaeren J. Outbreak of Shigella sonnei infections in the Orthodox Jewish community of Antwerp, Belgium, April to August 2008. Euro Surveill. 2011;16:19838. [PubMed] [Google Scholar]
- 23.McDonnell J, Dallman T, Atkin S, Turbitt DA, Connor TR, Grant KA, et al. Retrospective analysis of whole genome sequencing compared to prospective typing data in further informing the epidemiological investigation of an outbreak of Shigella sonnei in the UK. Epidemiol Infect. 2013;141:2568–75. 10.1017/S0950268813000137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sobel J, Cameron DN, Ismail J, Strockbine N, Williams M, Diaz PS, et al. A prolonged outbreak of Shigella sonnei infections in traditionally observant Jewish communities in North America caused by a molecularly distinct bacterial subtype. J Infect Dis. 1998;177:1405–9. 10.1086/517825 [DOI] [PubMed] [Google Scholar]
- 25.Ashton PM, Baker KS, Gentle A, Wooldridge DJ, Thomson NR, Dallman TJ, et al. Draft genome sequences of the type strains of Shigella flexneri held at Public Health England: comparison of classical phenotypic and novel molecular assays with whole genome sequence. Gut Pathog. 2014;6:7 . 10.1186/1757-4749-6-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Quail MA, Kozarewa I, Smith F, Scally A, Stephens PJ, Durbin R, et al. A large genome center’s improvements to the Illumina sequencing system. Nat Methods. 2008;5:1005–10. 10.1038/nmeth.1270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Quail MA, Otto TD, Gu Y, Harris SR, Skelly TF, McQuillan JA, et al. Optimal enzymes for amplifying sequencing libraries. Nat Methods. 2011;9:10–1. 10.1038/nmeth.1814 [DOI] [PubMed] [Google Scholar]
- 28.Baker KS, Dallman TJ, Ashton PM, Day M, Hughes G, Crook PD, et al. Intercontinental dissemination of azithromycin-resistant shigellosis through sexual transmission: a cross-sectional study. Lancet Infect Dis. 2015;8:933–21. 10.1016/S1473-3099(15)00002-X [DOI] [PubMed] [Google Scholar]
- 29.Croucher NJ, Page AJ, Connor TR, Delaney AJ, Keane JA, Bentley SD, et al. Rapid phylogenetic analysis of large samples of recombinant bacterial whole genome sequences using Gubbins. Nucleic Acids Res. 2015;43:e15. 10.1093/nar/gku1196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stamatakis A. RAxML-VI-HPC: maximum likelihood-based phylogenetic analyses with thousands of taxa and mixed models. Bioinformatics. 2006;22:2688–90. 10.1093/bioinformatics/btl446 [DOI] [PubMed] [Google Scholar]
- 31.Drummond AJ, Rambaut A. BEAST: Bayesian evolutionary analysis by sampling trees. BMC Evol Biol. 2007;7:214. 10.1186/1471-2148-7-214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rambaut A, Lam TT, Max Carvalho L, Pybus OG. Exploring the temporal structure of heterochronous sequences using TempEst (formerly Path-O-Gen). Virus Evolution. 2016;2:1. 10.1093/ve/vew007 [DOI] [PMC free article] [PubMed]
- 33.Carattoli A, Zankari E, Garcia-Fernandez A, Voldby Larsen M, Lund O, Villa L, et al. In silico detection and typing of plasmids using PlasmidFinder and plasmid multilocus sequence typing. Antimicrob Agents Chemother. 2014;58:3895–903. 10.1128/AAC.02412-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Carver TJ, Rutherford KM, Berriman M, Rajandream MA, Barrell BG, Parkhill J. ACT: the Artemis Comparison Tool. Bioinformatics. 2005;21:3422–3. 10.1093/bioinformatics/bti553 [DOI] [PubMed] [Google Scholar]
- 35.Ye C, Lan R, Xia S, Zhang J, Sun Q, Zhang S, et al. Emergence of a new multidrug-resistant serotype X variant in an epidemic clone of Shigella flexneri. J Clin Microbiol. 2010;48:419–26. 10.1128/JCM.00614-09 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Sample details for isolates of Shigella sonnei used in this study and reference strains from global context database.
Supporting data and phylogenetic and genetic characteristics of isolates of Shigella sonnei.