

Sir:
We read with interest the article by Hardwicke et al1 on the concept of using low-cost thermal imaging for perforator identification. We agree with the authors that low-cost thermal imaging (thermoscan) provides an adjunct investigation because handheld Doppler has a 45% chance of producing a false positive overall2; with an inexperienced surgeon, the number is even higher. In addition, high-quality 3-dimensional computed tomography angiogram is not available in every hospital.
We would like to share our experiences using 2 low-cost thermoscan (second-generation FLIR One and FLIR C2). The second-generation FLIR One has a better thermal resolution, but sometimes the application is not stable and locks for a short period of time (important images can be missed). The FLIR C2 does not have this problem, but its price is also higher ($700 vs $200). The second-generation FLIR One is able to lock the thermal range but it does not show the data on the screen; this could be a big problem that we will discuss later.
We would like to share some tips from our experiences to minimize imaging errors while using low-cost thermoscan. First, always operate on dry skin. Thermoscan detects temperature from the surface, and it is critical to scan a dry surface. Even small amounts of moisture on the skin surface will produce an emission error that could block the perforator. Second, when an attempt was made to move the unit closer to the skin, the image was not in focus; to produce a clear image with the first-generation FLIR One, you need to be at least 100 cm from the skin. The second generation of the FLIR One and FLIR C2 allow a much shorter distance from the skin, about 15 cm. Third, you must focus in the center of the screen because the low-cost thermoscan only has a center thermal sensor. Fourth, opt for a larger screen, because the screens of low-cost thermoscans are small and inconvenient to use. By using a larger screen, investigators can connect the second-generation FLIR One to an iPad and the FLIR C2 can be connected to a computer. Finally, select and lock the thermal range. Locking the thermal range will prevent errors from the investigator’s skin temperature, and we recommend the narrow range for better temperature differentiation. In a wide range (20–35), 3°C is represented by each of the colors. In a narrow range (25–30), 1°C is represented by each of the colors. It is easier to detect the temperature difference with the narrow range, and the narrow range also matches the range of flap temperature (about 6°C3).
Thermoscan has become our new favorite preoperative and intraoperative assistant, identifying vascular interconnections and perforators, which gives us higher advantages and more freedom to design a free-style perforator flap as shown in the case example (Figs. 1 and 2).
Fig. 1.
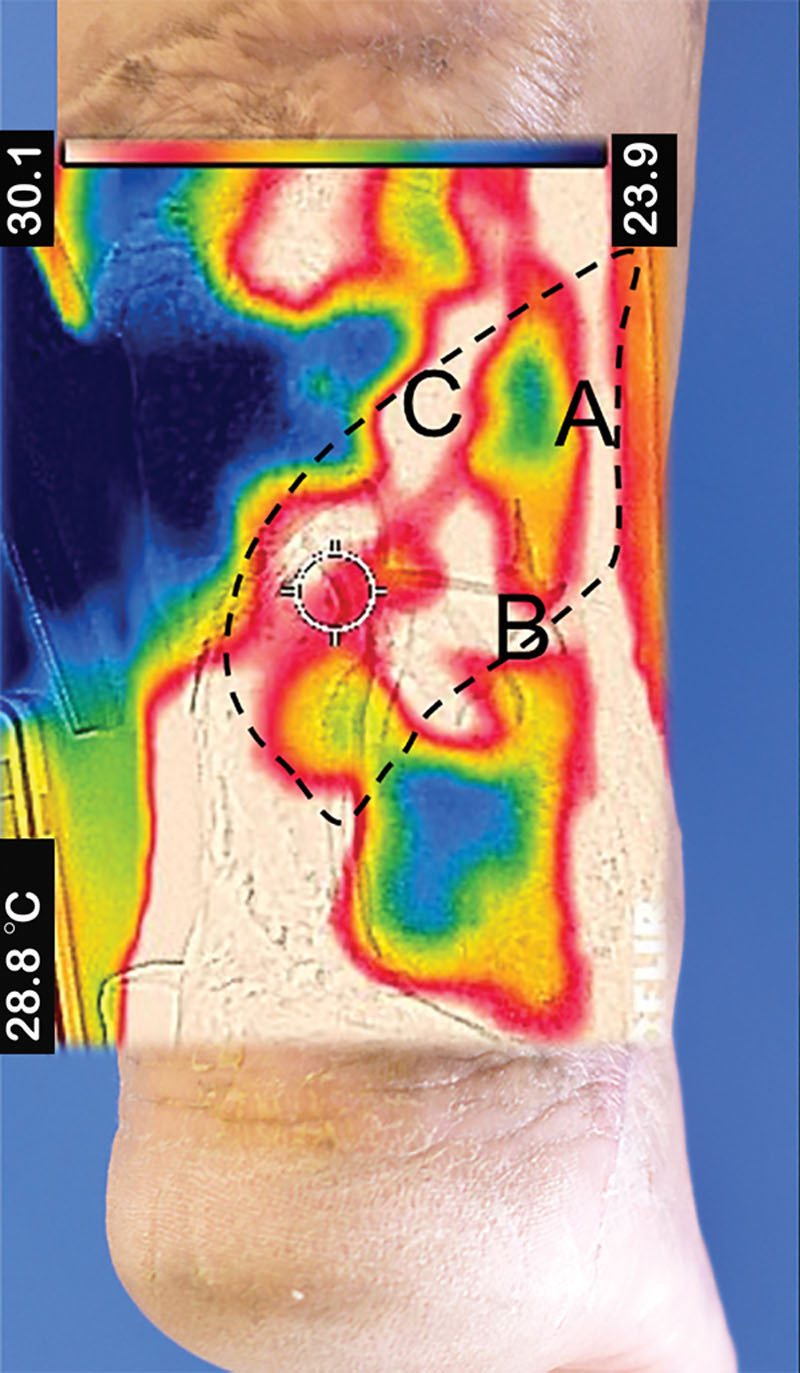
Thermal image acquired from posterior aspect of a patient’s right ankle. This patient had a chronic wound from an open fracture distal tibia Gustilo 3B with Achilles tendon rupture, which previously failed primary wound closure and wound dressing for 1 year. We brought the patient for free-style flap coverage. The flap was based on peroneal artery perforator (A), lateral calcaneal artery perforator (B), and lesser saphenous vein (C). The dashed line in the flap territory should include the vascular supply as much as possible.
Fig. 2.
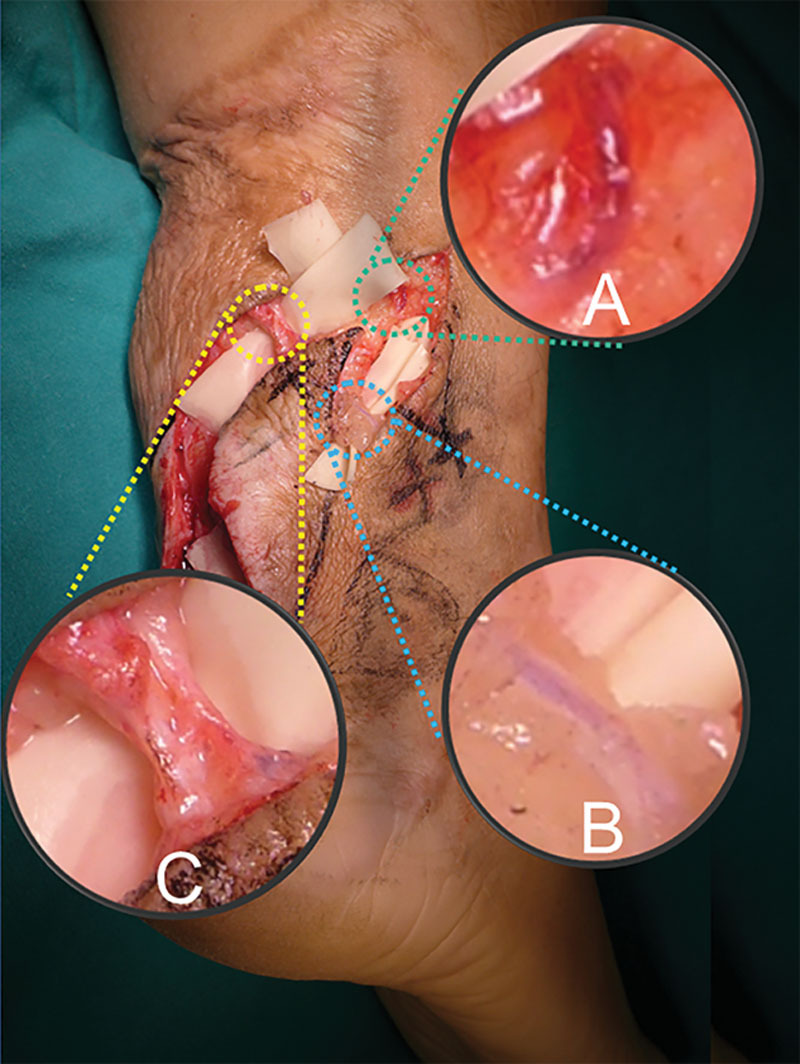
Intraoperative structures are shown. Peroneal artery perforator (A), lateral calcaneal artery perforator (B), and lesser saphenous vein (C) were identified, which match the preoperative thermal image.
DISCLOSURE:
The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Hardwicke JT, Osmani O, Skillman JM. Detection of perforators using smartphone thermal imaging. Plast Reconstr Surg. 2016;137:39–41. doi: 10.1097/PRS.0000000000001849. [DOI] [PubMed] [Google Scholar]
- 2.Stekelenburg CM, Sonneveld PM, Bouman MB, et al. The hand held Doppler device for the detection of perforators in reconstructive surgery: what you hear is not always what you get. Burns. 2014;40:1702–1706. doi: 10.1016/j.burns.2014.04.018. [DOI] [PubMed] [Google Scholar]
- 3.Kalra S, Dancey A, Waters R. Intraoperative selection of dominant perforator vessel in DIEP free flaps based on perfusion strength using digital infrared thermography—a pilot study. J Plast Reconstr Aesthet Surg. 2007;60:1365–1368. doi: 10.1016/j.bjps.2007.02.032. [DOI] [PubMed] [Google Scholar]