

Abstract
Exemplification of movement patterns is most noticeable in the youngest pupils group. Generally, children do not know which patterns are correct and which ones are risk factors. After correcting and stabilizing some improper patterns, a child can perform their daily activities without constant cognizance of their appropriateness. The concept of this research is included in a paradigm for the quality research conducted as action-research, which assumed a quality and efficiency improvement of health education in Polish schools.
The main aim of this study was to encourage pupils, their parents and teachers to perform pro-health behaviors oriented toward maintaining an appropriate body posture. First, the study aimed to assess the postures of children involved in the authorial program “I take care of my spine” in comparison with a group of children without diagnosed postural defects and not involved in the curriculum.
The examinations covered a group of 144 children (group A) ages 7 to 9 years (mean 7.60 ± 0.64 years) with appropriate body postures recognized in the screening test, which was conducted at a school where the curriculum “I take care of my spine” was launched. The control group included 222 healthy children at a similar age who attended schools where the curriculum was not implemented. The examinations were performed 2 times, as follows: the first time occurred before the program “I take care of my spine” was launched (initial examination), and the second time after 9 to 10 months of full participation in the program's activities and after 1 year of observation of children from group B (final examination).
A significant improvement of posturometric parameters in the main group and worsening of the parameters in the control group were noted. The results in examined groups of children and diversification of the results were linked to implementing the prevention program in the main group. In the group of children involved in the postural prevention program, the weight of school bags was significantly reduced.
This objective was particularly important for students because the manner of movement pattern exemplification will influence children's lives in the future, and in a wider perspective, it will play a crucial role in assessing their quality of life as adults.
INTRODUCTION
The twenty-first century might be described as the century of prevention (Blair). Prevention polices, including different aspects of health, have been reported.1 Many countries, in accordance with the indications of the World Health Organization (WHO),2 take care of the younger generation as an investment in future societal health. Screening performed in Polish kindergartens and schools is an example of preventive polices of early postural defects. It is observed that most children and adolescents carry overloaded school bags. According to the Chief Sanitary Inspectorate indication, the maximum load approved for younger pupils is equal to 10% to 15% of body mass, which is controlled by the Minister of National Education Regulation of the August 25, 2009 [J Laws, No. 130, item 1130].3 The development of civilization and technologies results in an increase each year in the amount of hours spent in front of a computer monitor or television (TV) screen or different technology innovations. Based on the results of international research on health behavioral patterns in children and adolescents (Health Behavior in School-Aged Children [HBSC]), 44.4% of school-age children spend 4 h in front of the TV screen on days off of school and only 35.5% of the pupils participate in the recommended level of physical activity.4 Physical activity is essential for long- and short-term physical and mental health, and it is associated with increased musculoskeletal and cardiovascular health and reduced anxiety and depression among young people.5,6 Physical activity habits established in youth are likely to be carried through into adulthood, whereas lower physical activity levels and excess sedentary behavior are associated with obesity and back pain in older adults. Sedentary behavior increases postural defects in youth.7,8
In practice, the rules of ergonomics are reduced by adjusting the workplace of a pupil and sometimes by buying a rehabilitation mattress. The question of maintaining an appropriate active position when learning and playing should be presented. For a developing younger person, body movement pattern repetitions of gymnastic exercises several times throughout the day are very important. This results from exemplification copying of patterns and attitudes from the observation of adults. After correcting certain improper patterns, a child can perform their daily activity without a constant cognizance of their appropriateness. The patterns should then be inherent and provide the body with protective mechanisms for growth spurts at puberty when the risks of postural defects are increased. Correct weight bearing on the feet and lower limbs results in a more symmetric pelvis position. This, in turn, creates favorable conditions for a symmetric load on the discs and growth cartilage of the developing spine, which is very susceptible to asymmetric overloads in daily life. The twenty-first century is predisposed to a sedentary lifestyle. Insufficient participation of children in leisure time physical activities in western countries is a well-known phenomenon.9 Puberty periods predispose adolescents to develop different postural defects and muscular deficits. Sedentary behavior has an impact on obesity, which is a metabolic syndrome in children10,11 and adults.12 The adolescent period predisposes children to develop different postural defects. Postural defects are the most frequently diagnosed problems in Poland.13 In the Czech Republic, the most frequently detected defects were as follows: protruding scapulae, increased lumbar lordosis, and round back.14 This may be the result of over diagnosis and classifying mild deviations as postural disorders, which, in turn, is caused by the fact that measurement tools are not used and diagnosis is based on a general subjective examination of body posture or with the help of Adam forward bend test or Matthias posture test.15–17 Using a plumb line, scoliometer or inclinometer allows the examiner to obtain an objective assessment and thus reduces the number of diagnoses of postural defects. Therefore, it is essential to assess the impact of the postural defects prophylaxis authorial program “I take care of my spine” on the postures of school-age children with the use of classic measurement tools. Screening of body posture cannot be based on only visual observation because of a lack of repetitiveness; every examination involving tool measurements allows 1 to describe, for example, the progression or regression of a curvature.
The aim of this study was to encourage pupils, their parents, and teachers (recipients of pro-health education actions) to perform pro-health behaviors oriented toward maintaining an appropriate body posture. This objective was particularly important for the students of this study because the manner of movement pattern exemplification will influence a children's life in the future, and from a wider perspective, it will play a crucial role in assessing their quality of life as adults. First, this study aimed to assess the postures of children involved in the authorial program “I take care of my spine” in comparison with the group of children without diagnosed postural defects and that were not involved in the curriculum. The responses for the following questions were examined:
How do posturometry parameters change in younger school-age children?
What do the above-mentioned changes cause as a result?
How do the children's body postures change following 10 months of pro-health school guidance?
How significant is it to implement posture defects prophylaxis programs in regular pediatric practice?
MATERIALS AND METHODS
Participants
The examinations comprised a group of 144 pupils (group A) ages 7 to 9 (mean age 7.6 ± 0.64) with appropriate body postures recognized in the screening test, which was conducted at a school where the curriculum “I take care of my spine” was launched. The control group included 222 healthy children ages 7 to 9 (mean age 7.72 ± 0.73; P = n.s.) who attended schools where the curriculum was not implemented. Both groups covered children in whom postural defects were not diagnosed with insignificant exceptions including asymmetries of spatial body position within the shoulders and shoulder blades. All of those who qualified as research patients (initial examination) were examined in the same conditions by the author of the study with the use of classic tools and postural assessment tests (a plumb line, Pedi-Scoliometer by Pedihealth Oy, Finland, and digital inclinometer SAUNDERS TMX-127). A detailed examination process, initial body positions, and norms range are shown in Figures 1–4. Children with diagnosed scoliosis or other significant posture disorders in 3 planes were excluded from the analysis of the initial examination. The analysis of this group was confronted with other groups (i.e., this evaluation is beyond the scope of this study). The exclusion criteria also covered ages <7 and >9 and children participating in sports as their extra school activities. This study recruited 559 potentially eligible students for examination. After exclusion of 193 ineligible students, we included a total of 366 students for the study. The remaining students were excluded in this analysis because of growth spurts, a long absence from school, and diagnosed defect posture participation in other programs of prevention and sport.
FIGURE 1.

Distance from the plumb line to the anal cleft.
FIGURE 4.
Measurement of the angle of kyphosis and lordosis (neutral position).
In both groups, the body posture assessment was performed according to the following research method: the 3-fold torso rotation angle measurement with a use of a Pedi-Scoliometer during Adam test in a free standing position. A torso rotation measurement was performed on the 3 following levels: on the top of the thoracic kyphosis curvature, thoraco-lumbar junction, and on the top of the lumbar lordosis; the highest values of the torso rotation angles at the assessed levels were evaluated in the analysis. On the basis of the above results, the Hump-Sum factor was also measured15,16 (Figures 1–4).
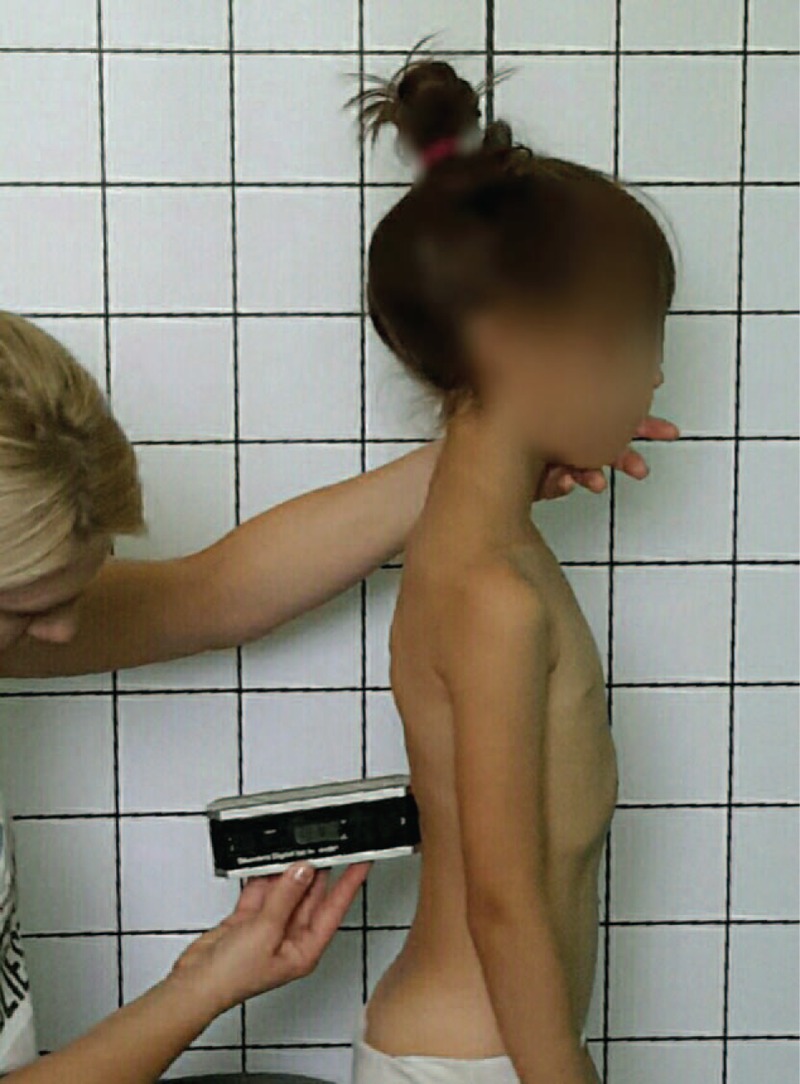
The measurement actions were taken as follows: evaluation of the deviation of the vertical in relation to the intergluteal cleft was performed (the plumb line was let down from occipital protuberance projected into the anal cleft and its right and left deviations were described in centimeters), the value of lordosis and kyphosis angle was assessed according to the Dobosiewicz method18 with a use of a digital inclinometer SAUNDERS TMX-127, and the shoulders and pelvis positions were measured with a ruler and Pedi-Scoliometer (Figure 1). The classical body posture examination included the following measurements:
Distance from the plumb line to the anal cleft (Figure 1).
Checking the scapula's level with the Pedi-Scoliometer (Figure 2).
Measurement of the angle of trunk rotation at the cervical, thoracic, and lumbar levels using the Pedi-Scoliometer (Figure 3).
Measurement of the angle of kyphosis and lordosis using an Inclinometer Sunders TMX-127 (Figure 4).
FIGURE 2.
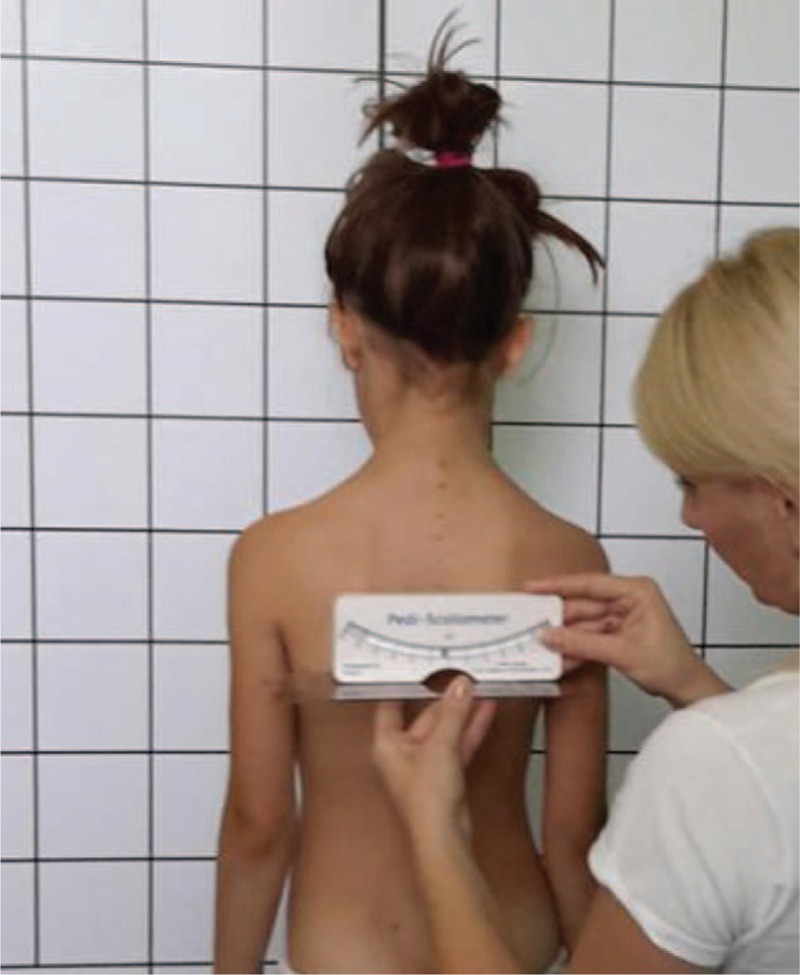
Checking the scapula's level.
FIGURE 3.

Measurement of the angle of the trunk rotation at the thoracic level.
The students’ heights were measured and recorded in centimeters, and the students’ weights were measured and recorded in kilograms. The body mass index (BMI) was presented as a percentile (BMI in kg/m2 adjusted to age and sex and in accordance with the table on the population of children). The BMI was calculated for children and teens; it is expressed as a percentile that can be obtained from either a graph or a percentile calculator. Because weight and height change during growth and development as do their relations to body fat, a child's BMI must be interpreted in relation to other children of the same sex and age. BMI for age weight status categories and the corresponding percentiles were based on expert committee recommendations.19,20
The examinations were performed 2 times, as follows: the first time before the program “I take care of my spine” was launched (initial examination) and the second time after 9 to 10 months of full participation in the program's activities and after 1 year of observation of children from group B (final examination). Additionally, children twice completed questionnaires containing questions related to everyday life ergonomic positions performed when learning and during playing or during leisure time activities. Numerous questions were presented as images to circle. The weight of the school bag carried twice a day was also measured during the 9- to 10-month intervals.
The curriculum “I take care of my spine” was proposed by AB. A detailed description of the curriculum “I take care of my spine” was published in Polish and international literature and put into practice across the entire Silesia Province.21,22 It includes several parts and involves children, their parents, and teachers so that the effect of the program can be maintained and stabilized. In this study, the results of the children who participated in the program are analyzed as the effect of exemplification of appropriate patterns. During classes, children learn about the structure and function of the spinal column, proper, and inappropriate movement patterns when learning and playing, and information about the causes of postural disorders and how they may affect their physical abilities as adults (Figure 5). The activities are enriched with various and more advanced audiovisual means, which help to develop a sense of responsibility for themselves and for others (e.g., taking care of a younger sibling or a classmate; Figure 6). Pilot studies revealed that the patterns are only maintained for several days, and it is then necessary to cyclically repeat them. This result is why the curriculum was implemented in educational institutions for a period of 6 years, from 2010 to 2015, and its effects are noticeable (Figures 5 and 6).
FIGURE 5.

(A–C) Prophylaxis program with pupils at school.
FIGURE 6.

(A–C) Exemplification of appropriate patterns.
Parents have been instructed on how to create an ergonomic workplace for their children and how to constantly control an ideal body position. A detailed analysis of behavior training aspects has been performed, and the weight of a pupil's school bag (Figure 7) was a significant factor to consider. Implementing the rules of ergonomics in daily activities performed by adults is an additional value (Figure 8). Teachers of subjects conducted in a sitting position and physical education teachers, who are temporarily not involved in their subject activities, are reminded about the presented pro-health behaviors and trained during the above-described practical classes of the curriculum (Figure 9). Conducting gymnastics between lessons became a fixed part of the school day, and revision quizzes were conducted by middle schoolers and the curriculum volunteers. Children from both groups also participated in physical education classes at school 3 to 4 times/wk for 45 min. The school curriculum included general development exercises, games, and movement activities and volleyball and basketball basics according to the school curriculum approved for classes I to III.
FIGURE 7.

Examples of good positions for carrying a pupil's school bag.
FIGURE 8.

(A and B) Parents part of the prophylaxis program.
FIGURE 9.

Teachers’ part of the prophylaxis program.
Children qualified to be in the control group were only observed (passive care). The children pursued sport activities in school sport clubs. Among the examined pupils, there was no child who, as a sport club member, trained in any type of sport on an advanced (sportsman/sportswoman) level (Figures 7–9).
Results
After a period of 9 to 10 months, the study was repeated (final examination) in both of the examined groups. The examinations were performed identically as initial examinations and individual results of pupils were put in 1 database with the intention of further evaluation. The following criteria from a detailed analysis of body posture were collected for further analysis: height, weight, torso rotation angle, angle value of kyphosis and lordosis, position level of shoulder blades, and deviation of the vertical in relation to the anal cleft, and the Hump-Sum parameter was calculated. Exceptional attention was focused on the differences between the particular examinations. The results of the initial and final examinations were first analyzed independently and then a comparative analysis of the examinations was performed. In both groups, the initial and final results were compared (the differences between the results noted independently were evaluated). The presented results are part of a larger science project and consent was obtained from the Bioethical Commission of the Medical University of Silesia in Katowice under resolution No. KNW/0022/KB1/162/10.
Statistical Analysis
The data were entered in 1 database and analyzed with Excel and Statistica v. 10 StatSoft software.23 In the study, the value of torso rotation angle before the curriculum was launched and just after intensive practicing in schools, was estimated. First, the results were described separately for both examinations (preliminary and final), followed by an evaluation of both groups. Next, comparisons were made between groups and between studies. The relationships between particular results were searched sequentially, and the results are shown as a number (%), mean (x), and standard deviation. Then, the difference between the parameters obtained in both groups was described. For data analysis, descriptive statistics were used to compare median values, a t test was applied for unrelated data and to assess relationships between examinations, and a nonparametric characteristics test χ2 and Rang Spearman test were also used. The statistical significance of P < 0.05 was assumed for all analyses.
RESULTS
A preliminary analysis of the results revealed individual changes for the majority of the children examined. A detailed statistical analysis permitted for a null hypothesis regarding the presence of differences between the examined groups and the positive influence of “healthy spine school” on younger pupils’ body postures. The students’ body heights ranged from 120 to 142 cm (mean height 128.9 ± 4.88) in the main group and 117 to 139 cm (mean height 128.78 ± 4.95) in the control group (t = 0.21; P > 0.82). The students’ weights ranged from 20.5 to 32 kg (mean weight 26.35 ± 2.63) in the main group and from 20 to 39.7 kg (mean weight 25.92 ± 2.91) in the control group (t = 1.44; P > 0.14). In the examined group, the BMI for age percentiles were ranged between the 3rd and 95th percentiles (χ2 = 51.7 ± 27.03 in the A group and χ2 = 51.27 ± 27.19 in the B group).
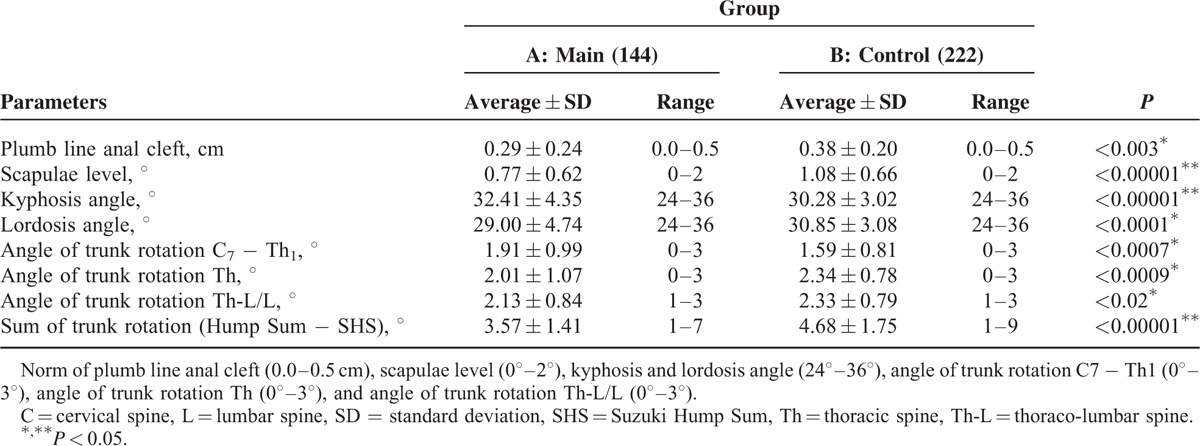
The criteria for inclusion were an appropriate body position diagnosed in the initial examination and mild deviations that did not exceed normal values for the particular age group studied (Table 1). Despite the statistically significant differences between the groups, which were favorable for the main group, the results in each group were described as “correct, normal” (Table 1).
TABLE 1.
Clinical Parameters at Study Entry
In group A (3.22%), sporadic, 2- to 3-week medical leaves from participation in the curriculum were mostly caused by infections; in 2 cases, upper fractures were the reason for absence. In group B, temporary leaves from physical education were caused by infections (20.38%) and sport injuries (4.27%) resulting in 1 to 5 weeks of absence (mean absence 2.73 ± 1.53 weeks). The absence did not significantly influence the results obtained after the period of observation in both groups (R Spearman = −0.01, P > 0.487 for group A; R = −0.03, P > 0.57 for group B).
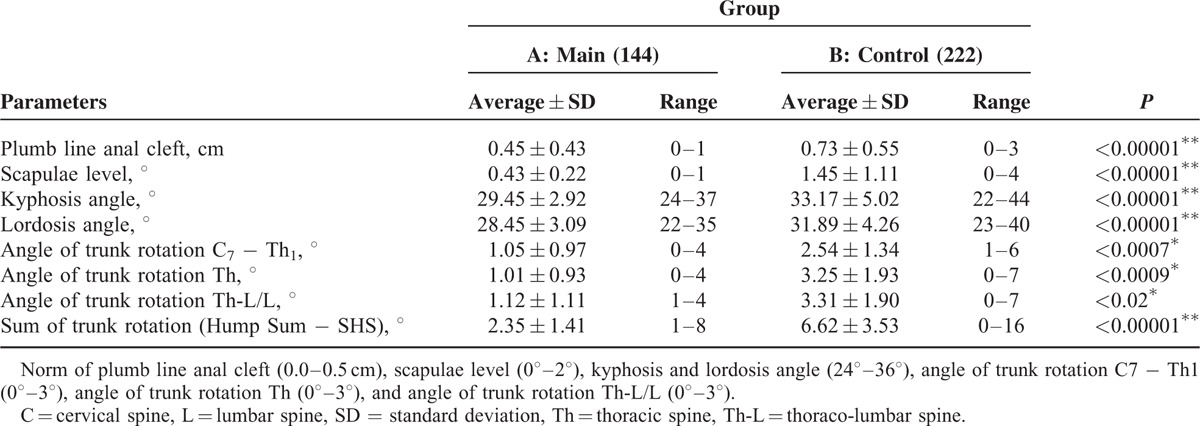
In the second examination (final) and for all of the groups, changes of posturometric parameters were noted in comparison to the initial examination. The changes involved all of the examined posturometric parameters in both of the examined groups (Table 2).
TABLE 2.
Clinical Parameters at Follow-Up
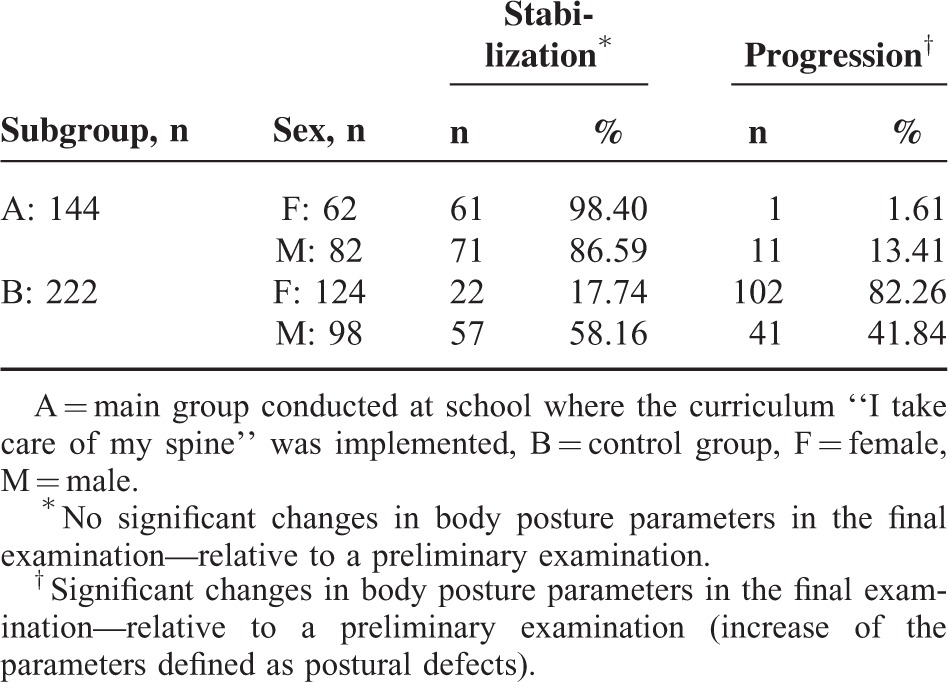
In the main group, statistically significant changes between the performed examinations were noted. The values of the measured parameters before the prophylaxis program and at follow-up are presented in Tables 3 and 4. However, in the main group, changes in the obtained results were expected. More importantly, from a practical point of view, the results for the majority of cases, despite an increase or decrease in values, were still within the norms. In 75% of the examined children, a decrease in torso rotation was noted, and the sex of the pupils did not play any significant role (χ2 = 4.77, P > 0.09, for df = 2). An increase in torso rotation value was noticed in 20.83% of the examined children from group A and 64.41% in group B; in 24.77% of examinees, a torso rotation value of more than 7 was noted and in 19.84%, the rotation values totaled 10 to 13 with a significant asymmetry in pelvis position, which was not revealed in the initial examination. In this group, girls obtained much worse results (χ2 = 21.28, P < 0.00002). The children in whom scoliosis was suspected were referred to orthopedic specialists and X-ray images were recommended. In main group A, 18 examined children were taken for additional observation. In these children, the rotation value did not exceed the range of 4 to 6. These children were put under a physiotherapist's care so that the following control examination could be performed within 6 months. A total of 6 children were referred to orthopedic consultation. The percentage of body posture stabilization and progression at the follow-up are represented in Table 5. The thoracic kyphosis angle exceeded the Dobosiewicz norm in 71 of the examined patients (31.98%) in group B and in 10 children (6.94%) of group A. In the main group, a decrease in the lordosis angle below the norm was indicated in 1 case (Tables 3 and 4).
TABLE 3.
Comparison of Pre and Postphylaxis Program Values of Measured Parameters (N = 144)
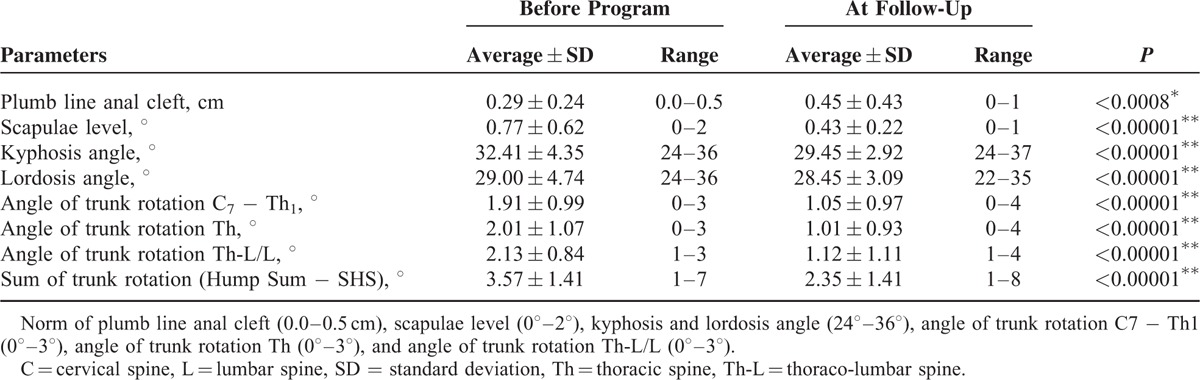
TABLE 4.
Comparison of Pre and Postobservation Values of Measured Parameters (N = 222)
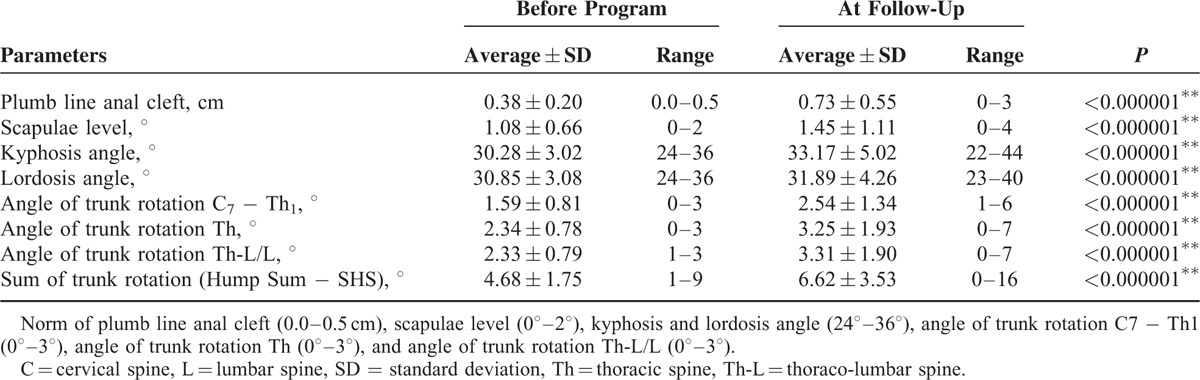
TABLE 5.
Percentage Values of Body Posture Stabilization and Progression
Children in whom a growth spurt was observed were excluded from the results analysis, and the obtained posturometric parameter results in the final examination were not influenced by changes of height between the 2 examinations in the main group A (all P > 0.06) or in the control group B (all P > 0.129), apart from the torso rotation parameter measured in the lumbar spinal segment in the main group (R = 0.26, P < 0.001) and in kyphosis angle (R = −0.14, P < 0.035) and scapulae level (R = −0.15, P < 0.019) in the control group. In children who participated in the curriculum “I take care of my spine,” a more significant difference of body mass between examinations resulted in a decrease in torso rotation value in the lumbar spine (R = −0.45, P < 0.001, for group A). Sex did not influence the obtained results in both examinations of both groups (P > 0.11; Table 5).
Children from group A, after 1 year of participation in the curriculum, performed an appropriate body position in approximately 93.75% of the cases. They were conscious of performing appropriate positions and ergonomic behaviors during daily activities. In the initial examinations, the students’ school bag weight was ranged 5.5 to 9.0 kg (mean weight 7.46 ± 0.9) in both group (t = 0.01, P > 0.98). In group A, parents were educated regarding the threats caused by the fact of carrying overloaded school bags by their children. They were informed directly during the parents’ meeting and by information posters displayed on the school walls and on the school internet site. In the final examinations, the students’ school bag weight was ranged 3.9 to 7.2 kg (mean weight 5.37 ± 0.79) in group A (Figure 10). A decrease in school bag weight was noticed as early as the first school year. The weight of the backpack decreased in the range 0.5 to 4.1 kg (mean weight 2.07 ± 0.89). In the control group, a 43.89% decrease in school bag weight ranged 0.0 to 2.9 kg (mean weight 1.17 ± 0.11; t = 2.45, P < 0.01).
FIGURE 10.
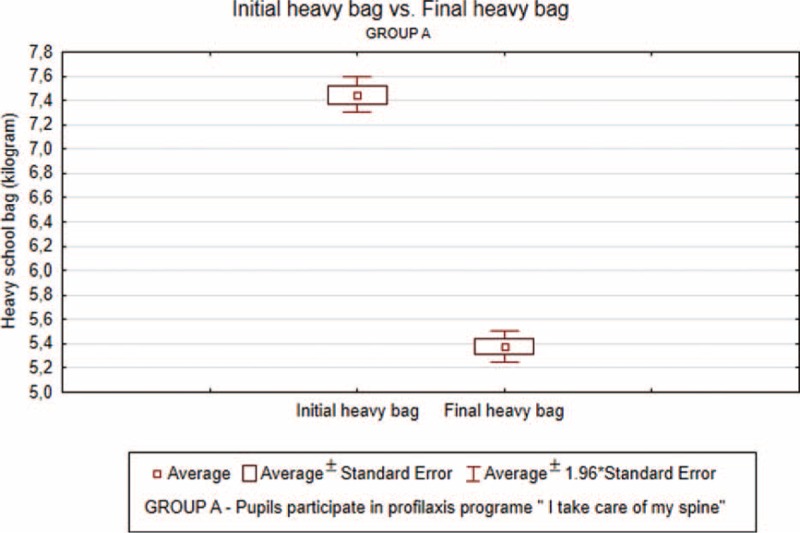
Average values and standard deviations of school bag weight in the initial and final examination in main group A).
The reduction in school bag loading consisted of a detailed analysis of necessary belongings that were put every day into the bags and the possibility of leaving books, pencil case, paint box, spare shoes, and sport gear in school lockers. Drinks (water and juice) were provided by the school, which resulted in a reduction of the load of a school bag by 0.5 kg.
In summary, it can be said that regardless of the mild deviations in body position assessed as appropriate, changes appeared within 1 year. This is caused by many endogenous and exogenous factors. Endogenous factors are not always in the scope of our influence, but exogenous factors can be modified, for example, by performing an appropriate body position when sitting, standing, learning, or playing and the reduction of the school bag weight carried by younger pupils. In the group of children who participated in the intensive postural defects prevention program for the whole school year, a significant improvement in body posture and postural behaviors were observed, for example, maintaining lumbar lordosis in a sitting position without enforcing so called “shoulder blades,” and the number of inappropriate postural behaviors, such as improper sitting and carrying a school bag on 1 shoulder, were reduced. Age and morphologic parameters did not have any influence on the obtained posturometric parameter results.
DISCUSSION
In our work environment, children over the age of 7 are particularly exposed to asymmetric loads, which are the result of a sedentary lifestyle, school bags that are too heavy, incorrectly adjusted chair and desk height, and a lack of physical activity and being overweight. Within the first years of life, contractures of muscles in the lower limbs, which are responsible for symmetric pelvis and spine position, are noted in children. It is essential to eliminate these exogenous and endogenous factors as the base for further physical activity of children and adolescents. However, to achieve this goal, deep reflection on the prevention method and its long-term influence on the body posture of growing children is necessary. One type of approach is proposed by the author of this study and was developed into the curriculum “I take care of my spine,” which involves not only children but also their parents and teachers because only such a holistic influence on young people exemplifying patterns from the adult world is optimal and provides a guarantee of long-term effects. The complete evaluation of the program will only be possible after a period of several years of practice, but some positive effects have already been observed and appreciated by children, their parents, and teachers. Through formulation of the research hypothesis of a large scientific project, pilot studies were conducted in several schools in the Province of Silesia. The following conclusion has been made from these studies: ergonomic adjustment of school furniture with a certificate of compliance with the PN standard approved by the Minister of National Education and Sport regulation on health and safety in educational institutions from December 31, 2002 (J Laws 2003, No. 6, Item 69),24 is not enough to cover the necessary needs for creating optimal conditions for good posture development of younger pupils.
The global recommendations by the WHO include the following: providing a range of activities that appeal specifically to girls, educating the public through mass media to raise awareness, and change social norms around physical activity.25,26 It is important to encourage and embed physical activity during the younger years so that participation can continue across the individual's entire lifespan. Useful interventions include the following: engaging parents in supporting activity and encouraging their children's physical activity by providing multisite interventions using a combination of school-based physical education and home-based activities27,28 as well as developing school policies that promote highly active physical education classes, suitable physical environments with resources to support structured and unstructured physical activity throughout the day and active travel programs.
The findings suggest that the authorial prophylaxis program “I take care of my spine” in schools has an influence in shaping correct body posture, increases physical activity, and enables parents and teachers to have multilevel control.
In popular science literature, much is said regarding a correct sitting position, and in TV advertisements, participation of a physiotherapist in the family decision process during buying a mattress is shown. However, buying some equipment is only partly sufficient for the aim of good posture. The most important aspect in body posture development is maintaining an appropriate posture on ergonomic objects of daily life. A total of 27.08% of parents whose children participated in the prevention program “I take care of my spine” had never been informed about how important good posture is in maintaining lumbar lordosis and stabilization of pelvic deep muscles. This is only further proof that people listen superficially and the information given does not reach their attention. A total of 72.5% of adults believe that drawing in abdominal muscles or shoulder blade squinching would improve posture. Excessive tightening or stretching of some groups of muscles leads to a disbalance of the muscles. Sitting for long hours in front of a computer monitor causes stretching of the back extensor muscle, which results in an increase in thoracic kyphosis and thereby decreases in lumbar lordosis. Dysfunction of these muscles affects the suboccipital muscles and is the cause of protraction head. As a consequence, disbalance in the deep front myofascial meridians has been noted. Extensive tension of these muscles moves to the upper parts of the body, such as the infrahyoid muscles, and thereby head retraction will be hindered. This will result in performance of a correct position but only for a short time. Myofascial meridians will then hinder the correction, particularly when performing daily activities. More than 50% of adults reckoned that walking with a stick at the back is a gold standard for the prevention of postural defects. Other serious problems are very common among parents, such as giving children exemptions from physical education lessons and a lack of physical activities in children's free time; in addition to a sedentary lifestyle, these are significant risk factors of postural disorders. This author's study revealed that 65.88% of the children in the control group and 25% of the main group spend their leisure time actively outdoors only during winter and summer holidays. The same observation can be found in Kędra's29 research, which included 278 parents of children attending correcting gymnastics classes. This study reports that 87% of the parents give exemptions from physical education lessons to their children. It is important to be aware that slight deviations of posturometric parameters are not only cosmetic defects, but in the future, they can seriously affect one's health, such as the condition known as idiopathic scoliosis, which as a consequence, may lead to disorders of the cardiovascular and respiratory systems, impair general physical efficacy and pain syndromes and different health problems that are frequently not associated with a school-age postural disorder.
Meeting physical activity guidelines (at least 1 h of moderate-to-vigorous physical activity [MVPA] daily—recommended by the WHO) is significantly more frequent among 11-year-olds than 15-year-olds in almost all of the countries and regions. Boys were more likely to report getting at least 60 min of MVPA daily. Gender differences were significant in most countries and regions across all age groups.25 The 11-year-olds who report at least 1 h of MVPA daily occurred in Ireland (31% F and 43% M), Austria (30% F and 40% M), Spain (26% F and 41% M), and Poland (23% F and 31% M).5 Sedentary behaviors have been related to health complaints and aggression. TV viewing during adolescence is associated with weight gain in adulthood.25,30 Current recommendations suggest that children should have no more than 1 to 2 h of high-quality TV (including videos and DVDs) per day. Older pupils watch TV more often in most countries, such as the Ukraine (71% F and 69% M), the Netherlands (64% F and 69% M), Greece (64% F and 69% M), and Poland (61% F and 64% M). However, in Austria and Switzerland, the share percentage of 11-year-olds who watch TV for 2 or more hours on weekdays is smaller (24% F and 29% M).31 Nothing will change without the participation of the pupils’ parents. Parents are likely to have a stronger influence on health behaviors than peers on 11-year-olds. Parents shape social norms and model behaviors. They are structural facilitators and determine eating, sleeping, studying, and leisure times for their children.32
That is why implementation in Polish schools of a multiannual prevention program of postural defects is fully justified. The prevention program “Straight back to health” described by Chudak and Permoda33 implemented in schools in Zielona Góra revealed a significant number of postural defects in all of the planes (more than 70% in Łódź and Zielona Góra). Unfortunately, detailed results after implementing the 3-year program were not described. As a result, it is impossible to evaluate its efficacy. In order to make possible references to the longitudinal effects of action on a multiannual basis and considering dynamic postural changes in posturogenesis, careful observations are necessary. Such a 6-year observation was presented in this study. In the early stages, the programming stage implementation of the curriculum in the daily school life of children seemed to be easier than later in the process. It is now clear that even short breaks (holidays) result in building inappropriate movement patterns that must be addressed during the first month of the next school year. It is also important to be aware of additional asymmetric loads of the movement system such as playing a musical instrument, especially for children in music schools. The results of such studies will be presented in the future work of the author.
CONCLUSION
This study provides a significant improvement of posturometric parameters in the intervention group and worsening of parameters in the control group. Positive results in the intervention groups were closely linked to the prevention programs. The most significant deficits are noted in the torso rotation values, particularly in the thoracic and lumbar spine and after the Hump Sum. In the group of children involved in the postural prevention program, the weight of school bags was significantly reduced. It is significantly important in pediatric practice to examine the whole body posture with the use of objective measurement tools and thereby prevent an over diagnosis or potential inaccuracy of the subjective assessment. A spine protection program is required on account of a sedentary lifestyle and the increasing rate of postural defects/deformations that occur during the development of youths to adolescents.
Acknowledgment
The authors wish to thank Edyta Rybak for proofreading the manuscript.
Footnotes
Abbreviations: BMI = body mass index, HBSC = Health Behavior in School-Aged Children, MVPA = moderate-to-vigorous physical activity, SD = standard deviation, WHO = World Health Organization.
The authors have no funding and conflicts of interest to disclose.
REFERENCES
- 1.World Health Organization. Global Strategy on Diet, Physical Activity and Health 2004; 2015. http://www.who.int/dietphysicalactivity/strategy/eb11344/strategy_english_web.pdf (accessed December 15, 2015). [Google Scholar]
- 2.World Health Organization. Ottawa Charter for Health Promotion, 1986–1986; 2015. http://www.euro.who.int/de/publications/policy-documents/ottawa-charter-for-health-promotion,1986 (accessed December 12, 2015). [Google Scholar]
- 3.Minister of National Education Regulation. J Laws, No. 130, item 1130. http://www.abc.com.pl/wyszukany-akt/-/akt/dz-u-2009-139-1130 (accessed September 25, 2009). [Google Scholar]
- 4.Bobakova D, Hamrik Z, Badura P, et al. Test–retest reliability of selected physical activity and sedentary behaviour HBSC items in the Czech Republic, Slovakia and Poland. Int J Public Health 2015; 60:59–67. [DOI] [PubMed] [Google Scholar]
- 5.Iannotti RJ, Janssen I, Haug E, et al. Interrelationships of adolescent physical activity, sedentary behaviour, and positive and negative social and psychological health. Int J Public Health 2009; 54:191–198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.William B, Strong WB, Malina RM. Evidence based physical activity for school-age youth. J Pediatr 2005; 146:732–737. [DOI] [PubMed] [Google Scholar]
- 7.Quka N, Stratoberdha D, Selenica R. Risk factors of poor posture in children and its prevalence. Acad J Interdiscip Stud 2015; 4:97–101. [Google Scholar]
- 8.Ningthoujam R. Postural deformities in lower extremities among school children. Int J Phys Educ 2014; 3:78–84. [Google Scholar]
- 9.Katzmarzyk PT, Barreira TV, Broyles ST, et al. Physical activity, sedentary time, and obesity in an international sample of children. Med Sci Sports Exerc 2015; 47:2062–2069. [DOI] [PubMed] [Google Scholar]
- 10.Dias KA, Green DJ, Ingul CB, et al. Exercise and vascular function in child obesity: a meta-analysis. Pediatrics 2015; 136:e648–e659. [DOI] [PubMed] [Google Scholar]
- 11.Salonen MK, Wasenius N, Kajantie E, et al. Physical activity, body composition and metabolic syndrome in young adults. PLoS ONE 2015; 10:e0126737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Leischik R, Foshag P, Strauss M, et al. Physical activity, cardiorespiratory fitness and carotid intima thickness: sedentary occupation as risk factor for atherosclerosis and obesity. Eur Rev Med Pharmacol Sci 2015; 19:3157–3168. [PubMed] [Google Scholar]
- 13.Mrozkowiak M, Sokołowski M. The diversity of the occurrence of body postures correct, faulty and scoliosis in children and adolescents aged 4 to 19 years with regard to sex and age in Poland. Rev Health Sci 2009; 1:14–17. [Google Scholar]
- 14.Kratěnová J, Žejglicová K, Malý M, et al. Prevalence and risk factors of poor posture in school children in the Czech Republic. J School Health 2007; 77:131–137. [DOI] [PubMed] [Google Scholar]
- 15.Asher M, Marc Lai S, Burton D, et al. Quantifier variables of the back surface deformity obtained with a noninvasive structured light method: evaluation of their usefulness in idiopathic scoliosis diagnosis. Spine 2004; 29:861–868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Patias P, Grivas TB, Kaspiris A, et al. A review of the trunk surface metrics used as scoliosis and other deformities evaluation indices. Scoliosis 2010; 5:5–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Popova-Ramova E, Poposka A, Ramov L. School screening for spine deformity with clinical test and spine mouse device. Jokull J 2013; 63:97–105. [Google Scholar]
- 18.Dobosiewicz K. Non-specific back pain in children and adolescents—neurophysiological, biomechanical and psychosocial factors. Neurol Dziec 2006; 15:51–57. [Google Scholar]
- 19.Javed A, Jumean M, Murad MH. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: a systematic review and meta-analysis. Pediatr Obes 2015; 10:234–244. [DOI] [PubMed] [Google Scholar]
- 20.Jodkowska M, Woynarowska B, Oblacińska A. A Screening Test for the Abnormalities’ Detection in the Physical Development of Children and Adolescents in School Age. Ezdorat Ed Warszawa2007. [Google Scholar]
- 21.Brzek A, Famuła A, Gaździk T. Preventive Program “My Healthy Spine in School” as the Exemplification of Actions Quality Improvement and Effectiveness of Health Education in Polish Schools. Jagiellonian Univ Ed2012; 174–183. [Google Scholar]
- 22.Brzek A, Dyrda B, Nowotny-Czupryna O, et al. Postural defects prevention programme as the exemplification of actions in the scope of health promotion in early school education—an action research perspective. New Educ Rev 2011; 24:194–204. [Google Scholar]
- 23.Aviva P, Sabin C. Manual Statistics at Outline. PZWL Ed2006; 1. [Google Scholar]
- 24.PN standard approved by Minister of National Education and Sport regulation on health and safety in educational institutions. J Laws 2003;6, item 69. http://dokumenty.rcl.gov.pl/D2003006006901.pdf (accessed December 31, 2002). [Google Scholar]
- 25.World Health Organization. Global Recommendations on Physical Activity for Health. 2010; Geneva: World Health Organization, (accessed February 23, 2012). [PubMed] [Google Scholar]
- 26.Kuntsche E, Pickett W, Overpeck M, et al. Television viewing and forms of bullying among adolescents from eight countries. J Adolesc Health 2006; 39:908–915. [DOI] [PubMed] [Google Scholar]
- 27.Brunton G, Harden A, Rees R, et al. Children and Physical Activity: A Systematic Review of Barriers and Facilitators. London: EPPI Centre, Social Science Research Unit Institute of Education, University of London; 2003. [Google Scholar]
- 28.De Meester F, van Lenthe FJ, Spittaels H, et al. Interventions for promoting physical activity among European teenagers: a systematic review. Int J Behav Nutr Phys Act 2009; 6:82–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kędra E. The problem of bad posture of children and youth in light of studies. AFM Ed Kraków2011. [Google Scholar]
- 30.Currie C, Zanotti C, Morgan A, et al. Social determinants of health and well-being among young people. Heal the Behaviour in School-Aged Children (HBSC) Study International Report from the 2009/2010 Survey (http://www.hbsc.unito.it/it/images/pdf/hbsc/prelims-part1.pdf). [Google Scholar]
- 31.Canadian Paediatric Society. Impact of media use on children and youth. Paediatr Child Health 2003; 8:301–306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ciairano S, Rabaglietti E, Roggero A, et al. Patterns of adolescent friendships, psychological adjustment and antisocial behavior: the moderating role of family stress and friendship reciprocity. Int J Behav Dev 2007; 31:539–548. [Google Scholar]
- 33.Permoda A, Chudak B. The problem of defects and body posture anomalies among children and adolescents in the area of the Green Mountains. Public Health 2010; 120:361–364. [Google Scholar]