

Abstract
Endoscopes in otolaryngology may facilitate accessing the lumens and sites such as upper cervical spine with minimally invasive surgical exposure. Here, we present 2 interesting cases of youth who underwent endoscopic removal of bullets in the cranial ridge junction region.
The first case was a 20-year-old young man who underwent a gunshot in the face. A CT scan showed that a metallic foreign body located inside the right lateral body of Atlas that presented a comminuted fracture. The second case a 36-year-old man who also underwent a gunshot in the face. CT scan showed a foreign body lodged in the soft tissues before the right anterior arch of Atlas cone (C1) that presented a fracture. The bullets in these 2 patients were removed under the endoscopes with minimal damage, respectively. The patients were discharged without neck activity obstacle.
The advantage of endoscopic technique is obvious because limited visualization does not damage surrounding tissues, thus decreasing surgical complications. This was an interesting experience of surgical operation in this region.
Keywords: bullets, cranial ridge junction region, endoscopes
1. Introduction
The use of endoscopy in otolaryngology has expanded into a wide range of aspects. Endoscopes may facilitate accessing the lumens and sites with minimally invasive surgical exposure. Here, we present 2 interesting cases of youth who underwent endoscopic removal of bullets in the cranial ridge junction region (upper cervical spine).
1.1. Case presentation
The first case was a 20-year-old young man who underwent a gunshot in the face when he was watching a brawl as an onlooker on November 22, 2014. Then, he spitted much blood and suffered from neck pain, with difficulties in neck activity without conscious disturbance. He was admitted to our hospital on November 23, 2014. An entrance wound was shown in his left upper lip soft tissue, with his left front incisor missing. Comminuted fracture was presented in the left alveolar process and the 1/3 front of bony palate. A CT scan showed that a metallic foreign body located inside the right lateral body of Atlas that presented a comminuted fracture, but has not entered into the vertebral canal, with the vertebral artery and odontoid unchanged (Fig. 1). No neurovascular compromise was presented. Under general anesthesia, transoral and transnasal visualization was realized by using a 4-mm zero-degree nasal endoscope within the vicinity of the foreign body behind the nasopharyngeal region. Careful blunt dissection was performed to minimize neurovascular injury and then the bullet was visualized and completely extracted, with the help of fluoroscopy. Cystic oppression in the nasopharyngeal region was used for hemostasis for 2 days. The patient's neck was immobilized with a cervical collar and was discharged. One month later, CT scan revealed no instability for the cervical vertebra.
Figure 1.
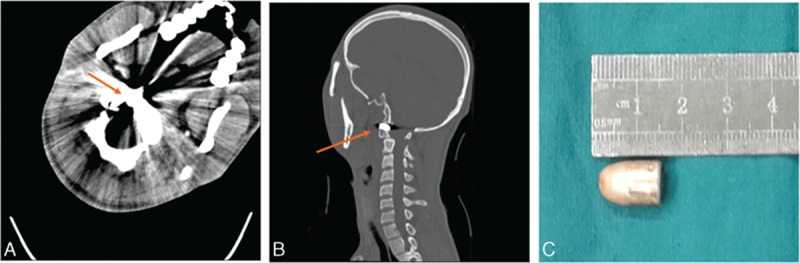
The first case: (A) axial CT scan showed that a metallic foreign body located inside the right lateral body of Atlas that presented a comminuted fracture, but has not entered into the vertebral canal; (B) sagittal CT scan showed that the bullet was located at the cranial ridge junction region; (C) the removed bullet (the arrows show the location of the bullet). CT = computed tomography.
The second case was a 36-year-old man who was admitted to our hospital on Mar 09, 2015, that had been 17 days after being shot in the face on Feb 20, 2015. The patient was awake and alert without conscious disturbance, airway and neck activity difficulties, and neurovascular compromise. The bullet had passed into the right alveolar process of the upper jaw bone and had broken the alveolar bone. CT scan showed a foreign body lodged in the soft tissues before the right anterior arch of Atlas cone (C1) that presented a fracture, without the vertebral artery and odontoid damaged. Under general anesthesia, transoral and transnasal visualization was achieved by using a 4-mm zero-degree nasal endoscope. An incision was made in the right side of the retropharyngeal wall. After careful dissection of the adjacent tissues, the bullet was fully found and taken out. Compression hemostasia was used at the operating field. The patient was then discharged without neck activity obstacle. One month later, CT scan confirmed the disappearance of the foreign body and the stability of the cervical vertebra (Fig. 2). This study was approved by the ethics committee of Southwest Hospital (Chongqing, China) and the informed consent was obtained from the patients.
Figure 2.
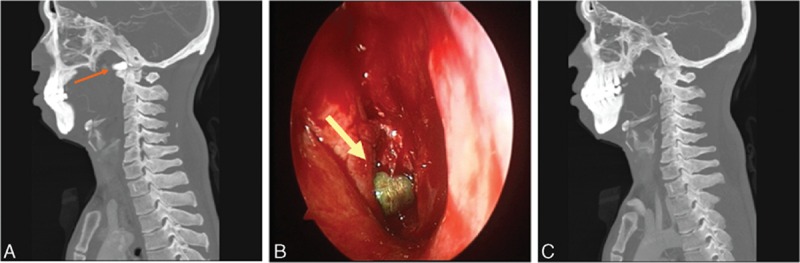
The second case: (A) sagittal CT scan showed that the bullet was located at the cranial ridge junction region; (B) intraoperative image of the bullet under the endoscopy. (C) sagittal CT scan confirmed the removal of the bullet (the arrows show the location of the bullet). CT = computed tomography.
2. Discussion
The cranial ridge junction region is difficult to access because its location is deep, around, which there are complex neurovascular structures. Thus, operating through this region represents a challenge. Traditional techniques accessing this site include lateral approaches that require external surface incision, thus increasing the risk of damaging the important structures such as spinal cord, vessels, and nerves.
Previous evidence presented several cases of gunshots with bullets located at cervical vertebra. However, the treatment strategies remain controversial. In 1990, Kupcha et al advocated observation of retained intracanal bullet fragments in the cervical spine of the patients rather than surgical removal.[1] The retained bullets in the spine do not increase the risk of infection,[2] but the surgical management might result in secondary complications. However, it is worthy of note that the bullets in the cervical spine might wander away from their initial locations. As the head and neck region is a small body part with several vital contents including important nerves and blood vessels, the migration of the bullets may easily damage the surrounding structures. Thus, Slysz et al had recently recommended that surgical removal of the bullets is necessary.[3] Given that the approach of lateral neck incision for bullet removal may markedly increase the likelihood of neurovascular injury,[4,5] surgical management of the gunshot wounds of the spine is not widely advocated, and microscopic techniques may be a good strategy for removal of the foreign bodies in the cervical spine.[6]
The endoscopic technique has been widely used for operation in paranasal sinuses, which was useful for the resection of benign lesions such as polyp or a part of neoplasms such as papillary epithelioma. In these 2 cases, the endoscopic technique was unusually utilized to retrieve foreign bodies from the cranial ridge junction region that were deeply located behind pharyngeal site with complicated neurovascular systems. The advantage of this approach is obvious because limited visualization does not damage surrounding tissues, thus decreasing surgical complications. Given the location of the bullets in the cranial ridge junction region, transnasal or transoral approaches were feasible. To our knowledge, endoscopic approaches to the cranial ridge junction region for removing foreign bodies have rarely been reported in the literature. Thus, this was an interesting experience of surgical operation in this region.
A bullet retained in the cervical column without nerve injury symptoms is an unusual phenomenon in surgical practice, because neurological deficits are very common in patients from cervical spinal gunshot wounds.[7] Intervention for instability is required for patients with or without neurological deficits because atlas fracture might lead to the instability of the connection between occipital condyle and the atlas, and secondarily result in spinal cord injury.[8] The reasons why a bullet fired at the face should stop at the level of the anterior atlas regions are obscure. The most probable explanation is that the bullets lost much of its kinetic energy when it hit and penetrate the dental structures and jawbones.
CT scanning is a major method for localization of the bullets in the preoperative evaluation. Intraoperatively, fluoroscopy was used and its drawbacks of radiation exposure and limited imaging is worthy of note. Surely, as open injury of cervical vertebra, postoperative anti-infection treatment was needed.
3. Conclusion
The advantage of endoscopic technique is obvious because limited visualization does not damage surrounding tissues, thus decreasing surgical complications. These 2 cases were interesting experiences of surgical operation in the cranial ridge junction region.
Footnotes
Abbreviation: CT = computed tomography.
QL and ZJ contributed equally to this study.
Authorship: conception and design—XZ; collection and assembly of data: QL, XZ, ZJ; manuscript writing: XZ, XZ; final approval of manuscript: all authors.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Kupcha PC, An HS, Cotler JM. Gunshot wounds to the cervical spine. Spine 1990;1510:1058–63. [DOI] [PubMed] [Google Scholar]
- [2].Velmahos G, Demetriades D. Gunshot wounds of the spine: should retained bullets be removed to prevent infection? Ann R Coll Surg Engl 1994;762:85–7. [PMC free article] [PubMed] [Google Scholar]
- [3].Slysz GW, Steinke L, Ward DM, et al. Automated data extraction from in situ protein-stable isotope probing studies. J Proteome Res 2014;133:1200–10. [DOI] [PubMed] [Google Scholar]
- [4].Wang J, Ye CY, Zhu MY, et al. Gunshot-caused facial injury combined with lower cervical spine injury: a case report. West Indian Med J 2014;634:378–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Walter T, Schwabe P, Schaser KD, et al. Positive outcome after a small-caliber gunshot fracture of the upper cervical spine without neurovascular damage. Polish J Radiol 2016;81:134–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Secer M, Ulutas M, Yayla E, et al. Upper cervical spinal cord gunshot injury without bone destruction. Int J Surg Case Rep 2014;53:149–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Beaty N, Slavin J, Diaz C, et al. Cervical spine injury from gunshot wounds. J NeurosurgSpine 2014;213:442–9. [DOI] [PubMed] [Google Scholar]
- [8].Marcon RM, Cristante AF, Teixeira WJ, et al. Fractures of the cervical spine. Clinics 2013;6811:1455–61. [DOI] [PMC free article] [PubMed] [Google Scholar]