

Abstract
The study was conducted to evaluate the Antibiotic Stewardship Program (ASP) in Korean hospitals compared with the previous two surveys in 2006 and 2012. The information on ASPs was collected through an online-based survey sent by e-mail to 192 infectious diseases specialists in 101 Korean hospitals in September 2015.
Fifty-four hospitals (53.5%, 54/101) responded to the online survey. One infectious diseases specialist was employed in 30 (55.6%) of the 54 hospitals, and they were in charge of ASPs in hospitals with the program. Fifty of the 54 hospitals (92.6%) had ASPs and the same number of hospitals was conducting a preauthorization-of-antibiotics-use program. Although most hospitals adopted preauthorization strategies for more antibiotics in 2015 than in 2012 (median 14 in 2015; 13 in 2012), a limited number of antibiotics were under control. The number of per oral and parenteral antibiotics available in hospitals in 2015 decreased compared to 2006 and 2012. The number of hospitals performing a retrospective or prospective qualitative drug use evaluation of antibiotic use increased from 2006 to 2015. Manpower in charge of antibiotic stewardship in most hospitals was still very limited and ASPs heavily depended on preauthorization-of-antibiotics-use programs in this survey. In conclusion, there leaves much to be desired in ASPs in Korea in 2015.
Keywords: Stewardship, Antimicrobial, Antibiotic, Korea, 2015
Graphical Abstract
INTRODUCTION
Multi-drug resistance (MDR), caused by an excessive antibiotic use, is considered to be a present threat to public health, and an emerging crisis (1). Unfortunately the pace of antimicrobial drug development has slowed markedly in the last 30 years, and there has been a significant decrease in the development and approval of new antimicrobial agents (2). Many experts suggest reducing antibiotic misuse as an approach for overcoming the threat posed by antibiotic-resistant infections (1). Infections by resistant organisms not only result in increased morbidity and mortality but also dramatically increase healthcare costs (3). According to a study conducted in the US, the medical costs attributable to antimicrobial-resistant infections ranged from $18,588 to $29,069 per patient (4). With the aim of improving antibiotic use in healthcare facilities, an antimicrobial stewardship program (ASP) has been developed. An ASP is a set of multidisciplinary activities focusing on the proper use of antimicrobials to provide optimal patient outcomes, reduce the risk of adverse effects, promote cost-effectiveness, and lower or stabilize levels of resistance (5).
Currently many Korean hospitals employ ASPs. According to two previous surveys in 2006 and 2012, their operation was entirely oriented to preauthorization-of-antibiotics-use programs (6,7). This study was conducted to examine the changing pattern of ASPs in Korea.
MATERIALS AND METHODS
The study was conducted in September 2015 among 192 infectious diseases (ID) specialists who work in 101 secondary or tertiary hospitals in Korea. The online-based survey linked to each e-mail collected information about the general profile of each hospital, its antimicrobial management committee (AMC), and strategies of the ASPs. One answer was accepted from each hospital. The data from similar surveys of ASPs in Korea in 2006 (6) and 2012 (7) which contained similar questions with the present survey, targeting the ID specialists, were used for comparison.
Antibiotics in this study included antibacterial agents, antifungal agents and antiviral agents except antiretroviral agents, excluding antiparasitic agents and antituberculous agents.
We classified the strategies of the ASPs into three categories: education and guidelines for antibiotic use, restriction on antibiotic use and drug use evaluation (DUE). Qualitative DUE is defined as a system of systematic, criteria-based evaluation of drug use that will help ensure that antibiotics are used appropriately; quantitative review of antimicrobial consumption as a measurement system of total amount of antimicrobial use.
The factors determining preauthorization-requiring antibiotics were calculated by a priority weighting method (e.g. 1st, 6 point; 2nd, 5 point; 3rd, 4 point; 4th, 3 point; 5th, 2 point; 6th, 1 point).
SPSS version 21.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Categorical variables were analyzed by the χ2 test or Fisher's exact test. A P value of < 0.05 was considered to be statistically significant.
RESULTS
Demographic information of hospitals
Fifty-four (53.5%, 54/101) hospitals responded to the 2015 online survey. In terms of the number of in-patient beds, most of the hospitals had 501-1,000 beds (63.6%, 35/54), while 21.8% (12/54) had 200-500 beds, and 12.7% (7/54) had more than 1,001 beds. One ID specialist (excluding fellows in training) was employed in the majority of the hospitals (55.6%, 30/54), while 29.6% (16/54) had two, 5.6% (3/54) had three or four, and 1.9% (1/54) had five or six (Table 1).
Table 1. Demographic information from the study hospitals: a comparison of the 2006, 2012 and 2015 surveys.
| Demographic parameters | No. (%) of hospitals | P value | ||
|---|---|---|---|---|
| 2006 (n = 44) | 2012 (n = 40) | 2015 (n = 54) | ||
| No. of in-patient beds in the hospitals | 0.148 | |||
| 200-500 | 3 (6.8) | 3 (7.5) | 12 (22.2) | |
| 501-1,000 | 33 (75.0) | 31 (77.5) | 35 (64.8) | |
| > 1,000 | 8 (18.2) | 6 (15.0) | 7 (13.0) | |
| No. of infectious diseases specialists | 0.864 | |||
| 1 | 20 (50.0) | 30 (55.6) | ||
| 2 | 12 (30.0) | 16 (29.6) | ||
| 3 | 3 (7.5) | 3 (5.6) | ||
| 4 | 3 (7.5) | 3 (5.6) | ||
| 5 | 0 (0) | 1 (1.9) | ||
| 6 | 1 (2.5) | 1 (1.9) | ||
| 7 | 1 (2.5) | 0 (0) | ||
| No. of laboratory microbiology specialists | - | |||
| 0 | 18 (33.3) | |||
| 1 | 31 (57.4) | |||
| 2 | 4 (7.4) | |||
| 3 | 1 (1.9) | |||
| No. of pediatric infectious diseases specialists | - | |||
| 0 | 33 (61.1) | |||
| 1 | 20 (37.0) | |||
| 3 | 1 (1.9) | |||
| Presence of antimicrobial management committee | 0.864 | |||
| Yes | 38 (92.7) | 35 (87.5) | 50 (92.6) | |
| No | 3 (3.65) | 5 (12.5) | 4 (7.4) | |
| No reply | 3 (3.65) | 0 (0) | 0 (0) | |
Looking at the hospitals participating in this survey, forty-eight (88.9%, 48/54) hospitals were concordant with the participants of either the survey of 2012 or 2006 (27.8% [15/54] participated in both 2012 and 2006; 16.7% [9/54] in 2012; 25.9% [14/54] in 2006).
Antimicrobial management committee (AMC)
An AMC was present in 92.6% (50/54) of the responding hospitals, and a figure was similar to those in the 2006 and 2012 surveys (92.7%, 38/44 in 2006; 87.5%, 35/40 in 2012, P = 0.864) (Table 1). Of the AMCs, 32.0% (16/50) held a meeting every 6 months and whenever there was an issue, 26.0% (13/50) did so quarterly, 14.0% (7/50) annually, and 4.0% (2/50) monthly. Significantly more AMCs in 2012 and 2015 took charge of determining antibiotics which require preauthorization (18.4%, 7/38 in 2006; 65.7%, 23/35 in 2012; 58.0%, 29/50 in 2015, P < 0.001) and DUE of antibiotics (18.4%, 7/38 in 2006; 38.7%, 19/35 in 2012; 40.0%, 20/50 in 2015, P = 0.006) than in 2006. Additionally, AMCs introduced new antibiotics (76.0%, 38/50), provided antibiotic use guidelines (46.0%, 23/50), dealt with antibiotic insurance claims (24.0%, 12/50), and analyzed antibiotic-resistance rates (14.0%, 7/50). The performance interval of these tasks was similar to the 2006 and 2012 surveys (data not shown).
Number of prescribed antibiotics in each hospital
Fifty-three hospitals (98.1%, 53/54) responded to the question about number of prescribed antibiotics. The number of parenteral antibiotics present in the hospitals was as follows: ≤ 40 in 6 of 53 hospitals (11.3%), 41-50 in 13 (24.5%), 51-60 in 15 (28.3%), 61-70 in 8 (15.1%), 71-80 in 5 (9.4%), 81-90 in 3 (5.7%), and ≥ 91 in 3 (5.7%). In terms of per oral antibiotics present in the hospitals was as follows: ≤ 40 in 17 of 53 hospitals (32.1%), 41-50 in 15 (28.3%), 51-60 in 9 (17.0%), 61-70 in 1 (1.9%), 71-80 in 5 (9.4%), 81-90 in 1 (1.9%), and ≥ 91 in 5 (9.4%). Comparing the proportion of hospitals containing > 60 parenteral or per oral antibiotics among 2006, 2012 and 2016 survey, a decreasing trend was observed: 55.7% (24/43) in 2006, 22.5% (6/37) in 2012, and 22.6% (12/53) for per oral antibiotics (P < 0.001); 50% (21/42) in 2006, 35% (11/37) in 2012, 25.9% (19/53) in 2015 for parenteral antibiotics (P = 0.187).
Strategies of ASPs
Fifty hospitals (92.6%, 50/54) had ASPs in this survey, similar to 2006 (95.5%, 42/44) and 2012 (87.5%, 35/40) (P = 0.397).
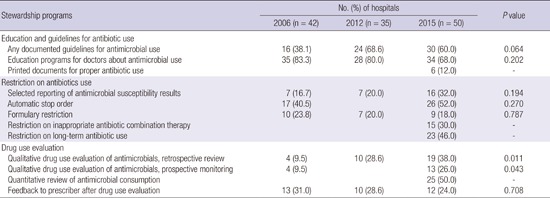
Table 2 presents the data in detail. In education and guidelines for antibiotic use, 60.0% (30/50) had some documented guidelines for antimicrobial use in 2015 (38.1%, 16/53 in 2006; 68.6%, 24/35 in 2012, P = 0.064), and 68.0% (34/50) had education programs for doctors about antimicrobial use (83.3%, 35/42 in 2006; 80.0%, 28/35 in 2012, P = 0.202). Twelve percent (6/50) provided a printed document for proper antibiotic use.
Table 2. Strategies of antimicrobial stewardship programs (ASPs): a comparison of the 2006, 2012 and 2015 surveys.
| Stewardship programs | No. (%) of hospitals | P value | ||
|---|---|---|---|---|
| 2006 (n = 42) | 2012 (n = 35) | 2015 (n = 50) | ||
| Education and guidelines for antibiotic use | ||||
| Any documented guidelines for antimicrobial use | 16 (38.1) | 24 (68.6) | 30 (60.0) | 0.064 |
| Education programs for doctors about antimicrobial use | 35 (83.3) | 28 (80.0) | 34 (68.0) | 0.202 |
| Printed documents for proper antibiotic use | 6 (12.0) | - | ||
| Restriction on antibiotics use | ||||
| Selected reporting of antimicrobial susceptibility results | 7 (16.7) | 7 (20.0) | 16 (32.0) | 0.194 |
| Automatic stop order | 17 (40.5) | 26 (52.0) | 0.270 | |
| Formulary restriction | 10 (23.8) | 7 (20.0) | 9 (18.0) | 0.787 |
| Restriction on inappropriate antibiotic combination therapy | 15 (30.0) | - | ||
| Restriction on long-term antibiotic use | 23 (46.0) | - | ||
| Drug use evaluation | ||||
| Qualitative drug use evaluation of antimicrobials, retrospective review | 4 (9.5) | 10 (28.6) | 19 (38.0) | 0.011 |
| Qualitative drug use evaluation of antimicrobials, prospective monitoring | 4 (9.5) | 13 (26.0) | 0.043 | |
| Quantitative review of antimicrobial consumption | 25 (50.0) | - | ||
| Feedback to prescriber after drug use evaluation | 13 (31.0) | 10 (28.6) | 12 (24.0) | 0.708 |
As for restriction on antibiotic use, 32.0% (16/50) adopted the strategy of selected reporting of antibiotic susceptibility results in 2015 (16.7% [7/42] in 2006, 20.0% [7/35] in 2012, P = 0.194), twenty-six hospitals (52.0%) operated an automatic stop order (40.5%, 17/42 in 2006, P = 0.270), and 18.0% (9/50) had formulary restrictions (23.8%, 10/42 in 2006; 20.0%, 7/35 in 2012, P = 0.787). In addition, fifteen hospitals had a strategy for controlling inappropriate antibiotic combination therapies, and 23 limited long-term antibiotics usage without appropriate clinical justification.
In terms of qualitative DUE, a significant trend of increase was observed both in retrospective and prospective methods. However, feedback to prescriber after DUE did not increase from 2006 to 2015.
Preauthorization-of-antibiotic-use programs
All hospitals with ASPs were conducting preauthorization-of-antibiotic-use programs. The spectrum of antibiotics was the most important factor (mean value 4.89), followed by possibility of development of resistant pathogens (mean value 4.81), insurance coverage (mean value 4.12), price (mean value 3.23), literature review (mean value 2.62), and adverse effect (mean value 3.23).
Table 3 summarizes detailed data on the programs. All hospitals with preauthorization-of-antibiotic-use programs had computerized systems for control (100%, 50/50). The proportion of hospitals with computerized system was higher than in 2006 and 2012 (P < 0.001). The main department determining antibiotics which require preauthorization was the division of ID in 30.0% (15/50), AMC in 58.0% (29/50), pharmacy board in 8.0% (4/50), and drug department in 4.0% (2/50) in this study. Twenty-six of 50 hospitals (52.0%) approved preauthorization-required antibiotics use by consultation (case by case approach) while 48.0% (24/50) used automated algorithms. In all the hospitals in this survey, division of ID had a primary responsibility for approval for preauthorization-required antibiotics use compared with 72.5% in 2012 (P < 0.001).
Table 3. Preauthorization-of-antibiotic-use programs: a comparison of the 2006, 2012 and 2015 surveys.
| Programs or systems | No. (%) of hospitals | 2015 (n = 50) | P value | |
|---|---|---|---|---|
| 2006 (n = 44) | 2012 (n = 40) | |||
| Computerized system for control | 26 (59.1) | 34 (85.0) | 50 (100.0) | < 0.001 |
| Cumulative number of updates for computerized system | ||||
| 0 | 6 (12.0) | |||
| 1-2 | 26 (52.0) | |||
| ≥ 3 | 16 (32.0) | |||
| No answer | 2 (4.0) | |||
| The greatest obstacle against update for computerized system | ||||
| Compatibility with existing programs | 9 (18.0) | |||
| Shortage of manpower | 32 (64.0) | |||
| Shortage of technical support | 6 (12.0) | |||
| Other | 1 (2.0) | |||
| No answer | 2 (4.0) | |||
| The main department determining antibiotics which require preauthorization | ||||
| Infectious disease | 9 (22.5) | 15 (30.0) | 0.424 | |
| Antimicrobial management committee | 17 (42.5) | 29 (58.0) | 0.144 | |
| Pharmacy board | 4 (10.0) | 4 (8.0) | 1.000 | |
| Drug department | 0 (0) | 2 (4.0) | 0.501 | |
| Others | 10 (25.0) | 0 (0) | < 0.001 | |
| Approval of preauthorization-required antibiotics use | ||||
| Consulting the department of primary responsibility (case by case approach) | 26 (52.0) | |||
| Automated algorithm | 24 (48.0) | |||
| The department of primary responsibility for approval of preauthorization-required antibiotics use | ||||
| Infectious disease | 29 (72.5) | 50 (100.0) | < 0.001 | |
| Pediatrics | 1 (2.5) | 0 (0) | 0.444 | |
| Others | 6 (15.0) | 0 (0) | 0.006 | |
| No answer | 4 (10.0) | 0 (0) | 0.036 | |
| Timing of antibiotic preauthorization commencement | ||||
| From the first prescription | 7 (15.9) | 10 (25.0) | 12 (24.0) | 0.527 |
| No restriction for a few days | 35 (79.5) | 12 (30.0) | 25 (50.0) | < 0.001 |
| From intervention by the department of primary responsibility for approval | 0 (0) | 2 (5.0) | 10 (20.0) | 0.002 |
| Others | 1 (2.3) | 6 (15.0) | 3 (6.0) | 0.076 |
| No answer | 1 (2.3) | 10 (25.0) | 0 (0) | < 0.001 |
A half of hospitals (50.0%, 25/50) permitted the use of preauthorization-required antibiotics for a few days before authorization (79.5%, 35/44 in 2006; 30.0%, 12/40 in 2012, P < 0.001), 24.0% (12/50) began restriction from the first prescription (15.9%, 7/44 in 2006; 25.0%, 10/40 in 2012, P = 0.527) and 20.0% (10/50) began restriction from intervention by the department of primary responsibility for approval (0%, 0/44 in 2006; 5.0%, 2/40 in 2012, P = 0.002). In the present survey, none of the hospitals reported they had antimicrobial cycling systems.
Fig. 1 shows the change of hospital proportions according to preauthorization-required antibiotics from 2006 to 2015. Hospitals in 2015 adopted preauthorization strategies for more antibiotics than in 2012 (number of preauthorization-required antimicrobials, median [range] were 14 [5.0-42.0] in 2015; 13 [9.5-20.0] in 2012). Most carbapenems such as imipenem, meropenem, doripenem and ertapenem were controlled by the preauthorization system in most hospitals, and increasing numbers of hospitals required a preauthorization for their use. Glycopeptides, such as vancomycin and teicoplanin, which have been the most frequently controlled antibiotics, needed approval in 98% of the hospitals (100%, 43/43 in 2006; 85.0%, 34/40 in 2012, P = 0.004). Tigecycline, which was recently introduced to the market, needed approval prior to being used in all the hospitals. Another newly introduced antibiotic, linezolid, also needed approval in most hospitals, but there was no significant difference from the 2006 and 2012 surveys (93.0%, 40/43 in 2006; 82.5%, 33/40 in 2012; 92.0%, 46/50 in 2015, P = 0.235). However, the proportion of hospitals requiring preauthorization for cefepime, ceftazidime, piperacillin/tazobactam, and aztreonam remained relatively low and did not show a change from 2006 to 2012. Among antifungal agents, the number of hospitals requiring preauthorization before use of liposomal amphotericin B and voriconazole increased from 2006 through 2015 (P = 0.032 and P = 0.002, respectively).
Fig. 1.

The change of hospital proportions according to preauthorization-required antibiotics: a comparison of the 2006 (n = 43), 2012 (n = 40) and 2015 (n = 50) surveys.
Compliance of other departments with ASPs
When we asked the other departments’ compliance with ASPs, most hospitals answered yes (70.4%, 38/54). The reason for a low compliance was ignorance (56.3%, 4/16), followed by prescribers’ stubbornness (25.0%, 4/16) and lack of interest (18.7%, 3/16) in hospitals answering a low compliance with ASPs. The hospitals were employing several policies to improve compliance: private conversations with the staff of other departments (57.4%, 31/54), education of other departments (31.5%, 17/54), giving a disadvantage for repeated inappropriate antibiotic use (24.1%, 13/54), and holding conferences about antibiotic use with other departments (16.7%, 9/54). No hospital offered incentives for appropriate antibiotic use.
Microbiologic culture report systems and therapeutic drug monitoring (TDM)
Active reporting systems for cultures of microorganisms were established at more hospitals in 2015 than in 2012 (55.0%, 22/40 in 2012 vs. 75.9%, 41/54 in 2015, P = 0.033). Cell phone messages (80.5%, 33/41) were used most frequently, followed by telephones (12.2%, 5/41), and computer networks (7.3%, 3/41). The specimens subject to active reporting were limited to blood (97.6%, 40/41) and cerebrospinal fluid (39.0%, 16/51) in most hospitals.
Forty-three of the 54 hospitals (79.6%) were performing therapeutic drug monitoring (TDM) (Table 4). TDM was applied to vancomycin (97.7%, 42/43), amikacin (37.2%, 16/43), gentamicin (27.9%, 12/43), and voriconazole (14.0%, 6/43). These frequencies were not significantly different from those in 2012. The departments in charge of the service were laboratory medicine (46.5%, 20/43), the drug department (37.2%, 16/54), and ID (11.6%, 5/43). The methods for requesting TDM were as follows: use of an existing TDM order code (51.2%, 22/43), consulting the department in charge (39.5%, 17/43), automatically linked to codes of drug level measurement (7.0%, 3/43), and automatically linked to codes of antibiotic prescription (2.3%, 1/43).
Table 4. Therapeutic drug monitoring (TDM).
| Drug monitoring | No. (%) of hospitals | P value | |
|---|---|---|---|
| 2012 (n = 20) | 2015 (n = 43) | ||
| Type of antibiotics | |||
| Vancomycin | 20 (100.0) | 42 (97.7) | 1.000 |
| Amikacin | 8 (40.0) | 16 (37.2) | 0.832 |
| Gentamicin | 8 (40.0) | 12 (27.9) | 0.337 |
| Voriconazole | 1 (5.0) | 6 (14.0) | 0.415 |
| Department in charge (multiple response) | |||
| Laboratory medicine | 10 (10.0) | 20 (46.5) | 0.796 |
| Drug department | 14 (70.0) | 16 (37.2) | 0.015 |
| Infectious disease | 4 (20.0) | 5 (11.6) | 0.448 |
| Method of requesting | |||
| TDM order code | 22 (51.2) | ||
| Consulting the department in charge | 17 (39.5) | ||
| Automatically linked to codes of drug level measurement | 3 (7.0) | ||
| Automatically linked to codes of antibiotic prescription | 1 (2.3) | ||
DISCUSSION
Although the importance of antimicrobial stewardship is being emphasized in many countries, research on such programs is limited in Korea. This is the third nationwide survey of ASPs in Korea followed by the surveys in 2006 and 2012. The survey enabled us to evaluate the changes in ASPs in Korean hospitals. Despite increasing numbers of ID specialists, there were still 4 hospitals that did not operate ASPs, and the proportion had not changed significantly from 2006 to 2015.
According to Infectious Disease Society of America (IDSA) guidelines, it is essential that the antimicrobial stewardship team include an ID physician and a clinical pharmacist with ID training, and that both of these individuals be recompensed appropriately for their time. They also recommend to include a clinical microbiologist, an information systems specialist, an infection control professional, and a hospital epidemiologist in the ASP team (8). Since clinical pharmacists are not readily available in Korea, ID specialists have to fulfill the core role of leading the committee (5). Most hospitals with 500-800 beds in this study employ one ID specialist for antibiotic stewardship, and there is no proper reward for all the activities involved in ASPs in the domestic medical insurance system. Therefore, systematic support from the government is imperative (5,8) as well as further adoption of the automated algorithm method for preauthorization-of-antibiotic-use programs (9,10).
The hospitals adopt a variety of strategies for antimicrobial stewardship; however, they are rather reluctant to perform other activities rather than the preauthorization-of-antibiotics-use program. In terms of education and guidelines for appropriate antibiotic use, many papers reported the importance of education and feedback: Wilf-Miron et al. (11) showed that the volume of antibiotic prescription by primary physicians who received peer group interventions was reduced, and Davey et al. (12) demonstrated the effect of restrictions on antibiotic use was compromising gradually with the passage of time. According to a study in Korea, one of the main factors leading to prescription of inappropriate antibiotic combinations is a lack of knowledge; hence bad habits can be corrected by education and feedback (13).
Activities promoting reduction on antibiotic consumption sector were even more limited. Most hospitals failed to have proper strategies, and only 18.0% had formulary restrictions on antibiotics. One bright point concerned the number of available antibiotics in each hospital: there was a marked decline in the number of antibiotics in use, and this was more prominent for per oral antibiotics (hospitals with more than 60 antibiotics: 55.7%, 24/43 in 2006; 22.5%, 6/37 in 2012; 22.6%, 12/53, P < 0.001). Many experts suggested designating individual drugs or selected formulary agents within a drug class in order to reduce the number of antibiotics with overlapping actions, as a strategy to prevent drug abuse and misuse (14,15). Although only few hospitals (18.0%, 9/50) have adopted a formulary restriction strategy compared to American hospitals (88.0% in 2010) (16), this decline indicates that hospitals have changed their policy with respect to the minimum number of required antibiotics.
At present most hospitals in Korea focus on preauthorization-of-antibiotic-use programs for carrying out ASPs. Studies have shown a decrease in antibiotic consumption as a result of such programs (9,17), and antimicrobial resistant patterns of pathogens improved when certain types of antibiotic were prescribed less (18,19). However, the scope of preauthorization programs necessarily varied depending on the number of antibiotics under control and the type of antibiotic control program (control of unnecessary combinations of antibiotics, length of antibiotic use for specific diseases, the purpose of antibiotic use, etc.). Considering the lack of ID specialists and the even fewer clinical pharmacists with ID training in hospitals, the scope of preauthorization-of-antibiotic-use is inevitably limited in most hospitals in Korea.
In general, ASPs in Korea achieved an improvement in several areas over a number of years; for example, a remarkably higher rate of computerization and increased number of antibiotics which require preauthorization. However, a major part of antibiotic use is not under control. According to a recent report, the total consumption of antibiotics for systemic use increased from 21.68 (DDD per 1,000 people per day) in 2008 to 23.12 (DDD per 1,000 people per day) in 2012, and the trend of increased use was more prominent for 3rd generation cephalosporins and fluoroquinolone, which did not require preauthorization (20). In fact, antibiotics which were controlled in most hospitals, such as carbapenems, glycopeptides, colistin, linezolid and tigecycline, represented a small proportion of the total consumption of systemic antibiotics (0.65%, 0.151/23.12 DDD per 1,000 people per day in 2012) (20).
We have some limitations in this study. First, the participants were not exactly the same as the previous two studies, which potentially could be a selection bias. Second, we only surveyed ID specialists in this study, and the results may have limitations in terms of representation. Considering the growing number of ID specialists working in the secondary hospitals, we think that the results of this survey represent the present situation of ASP in Korea.
In conclusion, ASPs are operated mainly by ID physicians in most hospitals in Korea, and the programs still depend on preauthorization-of-antibiotic-use. The most important requirements for appropriate operation of ASPs in Korea are reinforcement of manpower capable of performing ASPs, and national-level support.
Footnotes
Funding: This work was supported by a grant from the Korea Healthcare Technology R & D Project, Nationwide surveillance system of multidrug-resistant pathogens for prevention and control of antimicrobial resistance in Korea (HI12C0756), Ministry of Health and Welfare, Republic of Korea.
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conception and coordination of the study: Kim B, Kim J, Kim SW, Pai H. Data review: Kim B, Pai H. Statistical analysis: Kim B. Manuscript preparation: Kim B, Pai H. Critical review of the manuscript: Pai H. Manuscript approval: all authors.
References
- 1.Spellberg B, Guidos R, Gilbert D, Bradley J, Boucher HW, Scheld WM, Bartlett JG, Edwards J, Jr, Infectious Diseases Society of America The epidemic of antibiotic-resistant infections: a call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:155–164. doi: 10.1086/524891. [DOI] [PubMed] [Google Scholar]
- 2.Boucher HW, Talbot GH, Bradley JS, Edwards JE, Gilbert D, Rice LB, Scheld M, Spellberg B, Bartlett J. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:1–12. doi: 10.1086/595011. [DOI] [PubMed] [Google Scholar]
- 3.Giske CG, Monnet DL, Cars O, Carmeli Y. ReAct-Action on Antibiotic Resistance. Clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob Agents Chemother. 2008;52:813–821. doi: 10.1128/AAC.01169-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roberts RR, Hota B, Ahmad I, Scott RD, 2nd, Foster SD, Abbasi F, Schabowski S, Kampe LM, Ciavarella GG, Supino M, et al. Hospital and societal costs of antimicrobial-resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship. Clin Infect Dis. 2009;49:1175–1184. doi: 10.1086/605630. [DOI] [PubMed] [Google Scholar]
- 5.MacDougall C, Polk RE. Antimicrobial stewardship programs in health care systems. Clin Microbiol Rev. 2005;18:638–656. doi: 10.1128/CMR.18.4.638-656.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bang JH, Song KH, Park WB, Kim SH, Cho JH, Kim HB, Kim NJ, Oh M, Choe KW. A survey on antimicrobial prescriptions and stewardship programs in Korea. Infect Chemother. 2006;38:316–324. [Google Scholar]
- 7.Kim HI, Kim SW, Chang HH, Kim HB. A survey of antimicrobial stewardship programs in Korean hospitals. Korean J Med. 2014;87:173–181. [Google Scholar]
- 8.Dellit TH, Owens RC, McGowan JE, Jr, Gerding DN, Weinstein RA, Burke JP, Huskins WC, Paterson DL, Fishman NO, Carpenter CF, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159–177. doi: 10.1086/510393. [DOI] [PubMed] [Google Scholar]
- 9.Kim JY, Jo YM, Choi WS, Yoon YK, Jeong HW, Park DW, Sohn JW, Kim YM, Kim MJ. Usefulness of computerized restricted antibiotics use and control program in a tertiary care hospital. Infect Chemother. 2006;38:235–241. [Google Scholar]
- 10.Evans RS, Pestotnik SL, Classen DC, Clemmer TP, Weaver LK, Orme JF, Jr, Lloyd JF, Burke JP. A computer-assisted management program for antibiotics and other antiinfective agents. N Engl J Med. 1998;338:232–238. doi: 10.1056/NEJM199801223380406. [DOI] [PubMed] [Google Scholar]
- 11.Wilf-Miron R, Ron N, Ishai S, Chory H, Abboud L, Peled R. Reducing the volume of antibiotic prescriptions: a peer group intervention among physicians serving a community with special ethnic characteristics. J Manag Care Pharm. 2012;18:324–328. doi: 10.18553/jmcp.2012.18.4.324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, Ramsay CR, Wiffen PJ, Wilcox M. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev. 2013:CD003543. doi: 10.1002/14651858.CD003543.pub3. [DOI] [PubMed] [Google Scholar]
- 13.Song YJ, Kim M, Huh S, Lee J, Lee E, Song KH, Kim ES, Kim HB. Impact of an antimicrobial stewardship program on unnecessary double anaerobic coverage prescription. Infect Chemother. 2015;47:111–116. doi: 10.3947/ic.2015.47.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goff DA, Bauer KA, Reed EE, Stevenson KB, Taylor JJ, West JE. Is the “low-hanging fruit” worth picking for antimicrobial stewardship programs? Clin Infect Dis. 2012;55:587–592. doi: 10.1093/cid/cis494. [DOI] [PubMed] [Google Scholar]
- 15.Stevenson KB, Balada-Llasat JM, Bauer K, Deutscher M, Goff D, Lustberg M, Pancholi P, Reed E, Smeenk D, Taylor J, et al. The economics of antimicrobial stewardship: the current state of the art and applying the business case model. Infect Control Hosp Epidemiol. 2012;33:389–397. doi: 10.1086/664910. [DOI] [PubMed] [Google Scholar]
- 16.Johannsson B, Beekmann SE, Srinivasan A, Hersh AL, Laxminarayan R, Polgreen PM. Improving antimicrobial stewardship: the evolution of programmatic strategies and barriers. Infect Control Hosp Epidemiol. 2011;32:367–374. doi: 10.1086/658946. [DOI] [PubMed] [Google Scholar]
- 17.Oh JT, Kim SW, Son JW, Do BH, Han SW, Shin BC, Park JH, Lee JM, Kim NS. The effect of aminoglycoside restriction on the resistance pattern and mortality of nosocomial bacteremia caused by gram-negative bacilli. Infect Chemother. 2003;35:192–198. [Google Scholar]
- 18.Aubert G, Carricajo A, Vautrin AC, Guyomarc’h S, Fonsale N, Page D, Brunel P, Rusch P, Zéni F. Impact of restricting fluoroquinolone prescription on bacterial resistance in an intensive care unit. J Hosp Infect. 2005;59:83–89. doi: 10.1016/j.jhin.2004.07.016. [DOI] [PubMed] [Google Scholar]
- 19.Allegranzi B, Luzzati R, Luzzani A, Girardini F, Antozzi L, Raiteri R, Di Perri G, Concia E. Impact of antibiotic changes in empirical therapy on antimicrobial resistance in intensive care unit-acquired infections. J Hosp Infect. 2002;52:136–140. doi: 10.1053/jhin.2002.1277. [DOI] [PubMed] [Google Scholar]
- 20.Yoon YK, Park GC, An H, Chun BC, Sohn JW, Kim MJ. Trends of antibiotic consumption in Korea according to national reimbursement data (2008-2012): a population-based epidemiologic study. Medicine (Baltimore) 2015;94:e2100. doi: 10.1097/MD.0000000000002100. [DOI] [PMC free article] [PubMed] [Google Scholar]