

Abstract
The nationwide statistical analysis of each disease of classical myeloproliferative neoplasm (MPN) in Korea has not been reported yet. To this end, we have analyzed incidence rates, survival rates and treatment pattern of polycythemia vera (PV), primary myelofibrosis (MF) and essential thrombocythemia (ET) using Korea National Cancer Incidence Database (KNCIDB) and Health Insurance Review and Assessment Service (HIRA) database. Between 2003 and 2011, a total of 4,342 new cases of MPN were reported to the KNCIDB. ET was the most common, followed by MF and PV. The crude incidence rates for PV, MF, and ET have increased during the period, reaching 0.40, 0.15, and 0.84 per 100,000, respectively. Five-year relative survival rate of all MPN patients was 89.3%, with lowest relative survival rate with MF (53.1%). The prevalence of each disease estimated from HIRA data also increased during the study period. Notably, ET was found to be most prevalent. The prescription rate of hydroxyurea and phlebotomy to PV, MF and ET patients remained constant over the period, and the prescription rate of hydroxyurea was higher in patients with age over 60 years. This is the first Korean nationwide statistics of MPN, using central registry data. This set of data can be utilized to compare the Korean MPN status to international data and guidelines.
Keywords: Myeloproliferative Neoplasm, Incidence, Prevalence, Survival, Korea
Graphical Abstract
INTRODUCTION
Myeloproliferative neoplasms (MPN) are clonal hematopoietic stem cell disorders characterized by proliferation of one or more of the myeloid lineage cells. With recent expansion of understanding, there has been reclassification of the disease category since the first description of the concept of ‘myeloproliferative disorders (MPD)’ in the 1950s (1). A most recent revision of the classification of the diseases in this category has been issued by the World Health Organization (WHO) in 2008 (2) to include chronic myelogenous leukemia, chronic neutrophilic leukemia, polycythemia vera (PV), primary myelofibrosis (MF), essential thrombocythemia (ET), chronic eosinophilic leukemia, mastocytosis and other unclassifiable MPNs. Of the diseases in the MPN category, the classical Philadelphia chromosome-negative MPNs include PV, MF and ET. Reported worldwide incidence of the classical MPNs combined is approximately 0.5-6/100,000, annually, with peak incidence at the 5th to 7th decades of life (3,4,5,6,7,8). However, there have been more recent changes especially regarding accuracy and frequency of the diagnosis of the classical Philadelphia chromosome-negative MPN, owing to the discovery and clinical utilization of mutations in Janus kinase 2 (JAK2) (9) and Calreticulin (CALR) (10,11).
The Korean data for the hematologic malignancies (12) and the myeloid malignancies (13) have been previously published. During 1999 to 2012, myeloid malignancies took 1.7% of all cancer incidences, and MPNs took 33.8% of the myeloid malignancies. But the incidence and survival for each of disease of the MPN among Korean patients have not been reported.
The Ministry of Health and Welfare, Korea, initiated a nationwide hospital-based cancer registry called the Korea Central Cancer Registry (KCCR) as early as 1980. The registry collected 80%–90% of cancer cases annually from more than 180 training hospitals throughout the country. In 1999, the KCCR expanded cancer registration to cover the entire population under the Population-Based Regional Cancer Registry program. Details of the history, objectives and activities of the KCCR have been documented (14). Official registration of MPN at KCCR, employing the International Classification of Diseases for Oncology 3rd edition (ICD-O-3) (15) began in 2003. The Health Insurance Review and Assessment Service (HIRA) of Korea collects the claims data of the National Health Insurance, and offers clinical information including diagnosis, treatment, and prescription data for clinical research. The claims data covered approximately 46 million patients per year which is approximately 90% of the total population in Korea and included claims from almost 80,000 healthcare service providers, as of year 2011 (16).
The objectives of this report are to estimate and report the nationwide statistics of the classical MPN including PV, MF and ET from 2003 to 2011, using the Korea National Cancer Incidence Data Base (KNCIDB) and HIRA data.
MATERIALS AND METHODS
Data sources
Incidence data of MPN from year 2003 to 2011 were obtained from the KNCIDB. MPN included the following classification with ICD-O-3 morphology code: PV (M9950/3), MF (M9961/3), and ET (M9962/3). For survival analysis, passive follow-up was performed until 31 December 2012, using mortality database from Statistics Korea.
Number of cases of each diagnosis registered to HIRA of Korea during the same period was also obtained, and the prevalence of each disease was estimated. Drugs (hydroxyurea, interferon-α and danazol) and phlebotomy prescription data, which were available from HIRA for the period between year 2007 and 2011, were gathered to analyze the treatment pattern for the MPN.
Analysis
Crude incidence rates (CR) of each MPN were calculated, by dividing the total number of events by the total number of person-year of observation and multiplying 100,000 to the product. CRs were calculated for total population and also for each sex and age groups. Age-standardized incidence rates (ASR) were defined as weighted average of crude age-specific rates, using the mid-year estimated population of Korea in year 2000 as the standard population. Changes in the annual ASRs of cancer incidence were examined by calculating the annual percentage change over a time period as (exp[b] – 1) × 100, where b is the slope of the regression of log ASR for a given calendar year (17).
The survival analysis was done with incidence data registered to KNCIDB and vital status of each patient, followed through December 2012. The survival of each case were determined by the time difference between the date of diagnosis and the date of documented death, censored at the date of loss to follow-up or closing date for follow-up. Relative survival rates were calculated using life table method.
Using the data of number of cases registered to HIRA, we estimated prevalence for each diagnoses. We also used the prescription data for hydroxyurea and phlebotomy, which were available from HIRA. Data on prescription pattern of anagrelide were not available, due to article 9, paragraph 1, No. 7 of the Act on disclosure of public sector information. The patterns of prescription per diagnosis and age groups were analyzed using these data collected from HIRA. All statistical analyses were done with SAS (version 9.2; SAS Institute Inc, Cary, NC, USA).
Ethics statement
The present study protocol was exempted by the institutional review board of Seoul National University Bundang Hospital (Reg. No. X-1603-340-902).
RESULTS
Incidence
Between 2003 and 2011, a total of 4,342 new cases of MPN were reported to the KNCIDB. ET was the most frequent MPN with 2,200 new cases during the period, followed by PV with 1,582 new cases. MF was the least frequent, with 560 new cases. Relative frequencies of MPN per diagnosis in 2011 are depicted in Fig. 1.
Fig. 1.

Relative frequency of MPN incidence in Korea, 2011. (A) Men. (B) Women.
The numbers and the trends of CRs and ASRs from 2003 to 2011 are presented in Table 1. The CR of all three diseases in the category combined was 1.40 per 100,000 in 2011, with those of each PV, MF and ET being 0.40/100,000, 0.15/100,000 and 0.84/100,000, respectively. Crude incidence rates of total MPN were higher in men than in women (P = 0.005). PV and MF were more frequent in men than in women (P < 0.001 and P = 0.004, respectively for PV and MF), and ET was more frequent in women than in men (P = 0.004). The ASR of total MPN ranged from 0.45 to 0.94. The annual percentage change of ASR of total MPN was 9.9%, on the increase. The increase in ASR was most significant in ET, with an annual percentage change of 14.6%.
Table 1. Trends in crude incidence rates and age-standardized incidence rates of myeloproliferative neoplasm in Korea by incidence from 2003 to 2011.
| MPN type | Sex | Year | APC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | ||||
| MPN total | Total | Cases | 260 | 288 | 406 | 402 | 476 | 538 | 628 | 643 | 701 | |
| CR | 0.54 | 0.59 | 0.83 | 0.82 | 0.97 | 1.09 | 1.26 | 1.29 | 1.40 | |||
| ASR | 0.50 | 0.53 | 0.73 | 0.71 | 0.81 | 0.89 | 0.99 | 0.99 | 1.05 | 9.9* | ||
| Men | Cases | 135 | 152 | 212 | 214 | 261 | 282 | 310 | 337 | 380 | ||
| CR | 0.56 | 0.63 | 0.87 | 0.87 | 1.06 | 1.14 | 1.25 | 1.35 | 1.52 | |||
| ASR | 0.55 | 0.62 | 0.83 | 0.82 | 0.96 | 1.01 | 1.07 | 1.13 | 1.23 | 10.0* | ||
| Women | Cases | 125 | 136 | 194 | 188 | 215 | 256 | 318 | 306 | 321 | ||
| CR | 0.52 | 0.56 | 0.80 | 0.77 | 0.88 | 1.04 | 1.28 | 1.23 | 1.28 | |||
| ASR | 0.45 | 0.47 | 0.66 | 0.63 | 0.67 | 0.80 | 0.94 | 0.87 | 0.91 | 9.8* | ||
| PV | Total | Cases | 118 | 125 | 165 | 149 | 196 | 178 | 221 | 228 | 202 | |
| CR | 0.24 | 0.26 | 0.34 | 0.30 | 0.40 | 0.36 | 0.45 | 0.46 | 0.40 | |||
| ASR | 0.23 | 0.23 | 0.30 | 0.26 | 0.34 | 0.30 | 0.35 | 0.35 | 0.31 | 4.9* | ||
| Men | Cases | 70 | 77 | 100 | 101 | 131 | 114 | 131 | 138 | 115 | ||
| CR | 0.29 | 0.32 | 0.41 | 0.41 | 0.53 | 0.46 | 0.53 | 0.55 | 0.46 | |||
| ASR | 0.28 | 0.31 | 0.39 | 0.38 | 0.49 | 0.41 | 0.45 | 0.46 | 0.37 | 4.6* | ||
| Women | Cases | 48 | 48 | 65 | 48 | 65 | 64 | 90 | 90 | 87 | ||
| CR | 0.20 | 0.20 | 0.27 | 0.20 | 0.27 | 0.26 | 0.36 | 0.36 | 0.35 | |||
| ASR | 0.17 | 0.16 | 0.22 | 0.15 | 0.20 | 0.19 | 0.25 | 0.23 | 0.23 | 4.7* | ||
| MF | Total | Cases | 37 | 38 | 53 | 51 | 67 | 77 | 88 | 73 | 76 | |
| CR | 0.08 | 0.08 | 0.11 | 0.10 | 0.14 | 0.16 | 0.18 | 0.15 | 0.15 | |||
| ASR | 0.07 | 0.07 | 0.09 | 0.09 | 0.11 | 0.12 | 0.13 | 0.11 | 0.11 | 7.2* | ||
| Men | Cases | 20 | 23 | 28 | 29 | 34 | 45 | 49 | 47 | 47 | ||
| CR | 0.08 | 0.09 | 0.11 | 0.12 | 0.14 | 0.18 | 0.20 | 0.19 | 0.19 | |||
| ASR | 0.08 | 0.10 | 0.11 | 0.11 | 0.12 | 0.16 | 0.16 | 0.16 | 0.15 | 8.5* | ||
| Women | Cases | 17 | 15 | 25 | 22 | 33 | 32 | 39 | 26 | 29 | ||
| CR | 0.07 | 0.06 | 0.10 | 0.09 | 0.13 | 0.13 | 0.16 | 0.10 | 0.12 | |||
| ASR | 0.06 | 0.05 | 0.08 | 0.07 | 0.10 | 0.10 | 0.10 | 0.08 | 0.07 | 4.7 | ||
| ET | Total | Cases | 105 | 125 | 188 | 202 | 213 | 283 | 319 | 342 | 423 | |
| CR | 0.22 | 0.26 | 0.39 | 0.41 | 0.43 | 0.57 | 0.64 | 0.69 | 0.84 | |||
| ASR | 0.20 | 0.23 | 0.34 | 0.36 | 0.36 | 0.47 | 0.51 | 0.53 | 0.64 | 14.6* | ||
| Men | Cases | 45 | 52 | 84 | 84 | 96 | 123 | 130 | 152 | 218 | ||
| CR | 0.19 | 0.21 | 0.34 | 0.34 | 0.39 | 0.50 | 0.52 | 0.61 | 0.87 | |||
| ASR | 0.19 | 0.22 | 0.33 | 0.33 | 0.35 | 0.44 | 0.45 | 0.51 | 0.71 | 15.8* | ||
| Women | Cases | 60 | 73 | 104 | 118 | 117 | 160 | 189 | 190 | 205 | ||
| CR | 0.25 | 0.30 | 0.43 | 0.48 | 0.48 | 0.65 | 0.76 | 0.76 | 0.82 | |||
| ASR | 0.21 | 0.25 | 0.36 | 0.40 | 0.36 | 0.51 | 0.58 | 0.55 | 0.60 | 13.6* | ||
CR, crude rate; ASR, age-standardized rate; APC, annual percentage change; MPN, myeloproliferative neoplasm; PV, polycythemia vera; MF, primary myelofibrosis; ET, essential thrombocythemia.
*The annual percent change is statistically significantly different from zero (P < 0.05).
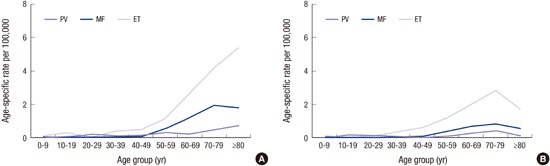
Higher incidence of MPN was seen in older age groups, with highest incidence in the age group of 60 to 69 years. ASR on the other hand, showed increasing tendency with increasing age. The ASRs by age groups in 2011 were shown in Fig. 2.
Fig. 2.

Age-specific incidence rates of MPN in Korea, 2011. (A) Men. (B) Women.
Survival
Five-year relative survival rates of the patients who were diagnosed with the three diagnosis of MPN from 2003 to 2011 were 89.3%, with lowest relative survival rate in patients with MF (53.1%) and highest relative survival rate in patients with PV (97.7%). The relative survival rate of ET was 92.2%. The relative survival rates of patients with MPN between 2003 and 2011 are summarized in Table 2.
Table 2. Relative survival rates with myeloproliferative neoplasm in Korea, 2003-2011.
| Sex | Diseases | No. of cases | Relative survival, % |
|---|---|---|---|
| Total | MPN total | 4,200 | 89.3 |
| PV | 1,534 | 97.7 | |
| MF | 533 | 53.1 | |
| ET | 2,133 | 92.2 | |
| Men | MPN total | 2,200 | 88.2 |
| PV | 950 | 97.9 | |
| MF | 302 | 48.5 | |
| ET | 948 | 90.9 | |
| Women | MPN total | 2,000 | 90.4 |
| PV | 584 | 97.3 | |
| MF | 231 | 59.0 | |
| ET | 1,185 | 93.2 |
MPN, myeloproliferative neoplasm; PV, polycythemia vera; MF, primary myelofibrosis; ET, essential thrombocythemia.
Prevalence estimates by cases registered to HIRA
The prevalence data of each diagnosis are summarized in Table 3. ET was the most prevalent, and MF the least. The general tendency of prevalence according to diagnosis, sex or age groups were similar to that seen with incidence of KNCIDB data. The total number of cases registered has increased approximately 3.2 fold, during the 9 years of observation from 2003 to 2011.
Table 3. Trends in prevalence of myeloproliferative neoplasm in Korea from 2003 to 2011, estimated with number of cases registered to Health Insurance Review and Assessment Service of Korea.
| MPN type | Sex | Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | |||
| MPN total | Total | Cases | 2,284 | 2,737 | 3,180 | 3,696 | 3,942 | 4,293 | 4,883 | 5,295 | 7,241 |
| CR | 6.04 | 7.10 | 7.99 | 9.10 | 9.62 | 9.99 | 11.03 | 11.67 | 12.56 | ||
| ASR | 5.48 | 6.28 | 6.89 | 7.70 | 7.89 | 7.94 | 8.46 | 8.65 | 9.02 | ||
| Men | Cases | 1,216 | 1,456 | 1,686 | 1,932 | 2,088 | 2,239 | 2,546 | 2,721 | 3,603 | |
| CR | 4.99 | 5.92 | 6.82 | 7.82 | 8.37 | 8.92 | 10.07 | 10.82 | 14.11 | ||
| ASR | 4.48 | 5.22 | 5.82 | 6.50 | 6.75 | 6.94 | 7.54 | 7.78 | 10.00 | ||
| Women | Cases | 1,068 | 1,281 | 1,494 | 1,764 | 1,854 | 2,054 | 2,337 | 2,574 | 3,638 | |
| CR | 4.42 | 5.27 | 6.11 | 7.20 | 7.50 | 8.25 | 9.33 | 10.21 | 14.34 | ||
| ASR | 4.05 | 4.73 | 5.34 | 6.21 | 6.25 | 6.70 | 7.36 | 7.84 | 10.84 | ||
| PV | Total | Cases | 1,188 | 1,364 | 1,516 | 1,673 | 1,749 | 1,824 | 2,006 | 2,114 | 2,304 |
| CR | 2.45 | 2.79 | 3.08 | 3.40 | 3.52 | 3.65 | 3.99 | 4.18 | 4.53 | ||
| ASR | 2.24 | 2.48 | 2.67 | 2.90 | 2.91 | 2.92 | 3.09 | 3.15 | 3.28 | ||
| Men | Cases | 688 | 813 | 907 | 1,033 | 1,096 | 1,138 | 1,243 | 1,285 | 1,386 | |
| CR | 2.82 | 3.31 | 3.67 | 4.18 | 4.39 | 4.53 | 4.92 | 5.16 | 5.43 | ||
| ASR | 2.55 | 2.92 | 3.16 | 3.53 | 3.60 | 3.61 | 3.78 | 3.80 | 3.91 | ||
| Women | Cases | 500 | 551 | 609 | 640 | 653 | 686 | 763 | 829 | 918 | |
| CR | 2.07 | 2.27 | 2.49 | 2.61 | 2.64 | 2.76 | 3.05 | 3.29 | 3.62 | ||
| ASR | 1.88 | 2.02 | 2.15 | 2.23 | 2.17 | 2.19 | 2.34 | 2.45 | 2.59 | ||
| MF | Total | Cases | 375 | 488 | 609 | 750 | 851 | 905 | 1,065 | 1,180 | 1,322 |
| CR | 0.77 | 1.00 | 1.24 | 1.52 | 1.71 | 1.81 | 2.12 | 2.33 | 2.60 | ||
| ASR | 0.69 | 0.88 | 1.06 | 1.27 | 1.38 | 1.41 | 1.59 | 1.70 | 1.83 | ||
| Men | Cases | 216 | 266 | 317 | 370 | 417 | 442 | 546 | 597 | 659 | |
| CR | 0.89 | 1.08 | 1.28 | 1.50 | 1.67 | 1.76 | 2.16 | 2.35 | 2.58 | ||
| ASR | 0.78 | 0.93 | 1.06 | 1.20 | 1.30 | 1.30 | 1.53 | 1.61 | 1.72 | ||
| Women | Cases | 159 | 222 | 292 | 380 | 434 | 463 | 519 | 583 | 663 | |
| CR | 0.66 | 0.91 | 1.19 | 1.55 | 1.76 | 1.86 | 2.07 | 2.31 | 2.61 | ||
| ASR | 0.60 | 0.82 | 1.04 | 1.33 | 1.45 | 1.51 | 1.62 | 1.77 | 1.93 | ||
| ET | Total | Cases | 721 | 885 | 1,055 | 1,273 | 1,342 | 1,564 | 1,812 | 2,001 | 3,615 |
| CR | 1.48 | 1.81 | 2.15 | 2.59 | 2.70 | 3.13 | 3.60 | 3.96 | 7.10 | ||
| ASR | 1.36 | 1.60 | 1.88 | 2.21 | 2.24 | 2.51 | 2.81 | 2.99 | 5.33 | ||
| Men | Cases | 312 | 377 | 462 | 529 | 575 | 659 | 757 | 839 | 1,558 | |
| CR | 1.28 | 1.53 | 1.87 | 2.14 | 2.31 | 2.63 | 2.99 | 3.31 | 6.10 | ||
| ASR | 1.15 | 1.37 | 1.60 | 1.77 | 1.85 | 2.03 | 2.23 | 2.37 | 4.37 | ||
| Women | Cases | 409 | 508 | 593 | 744 | 767 | 905 | 1,055 | 1,162 | 2,057 | |
| CR | 1.69 | 2.09 | 2.43 | 3.04 | 3.10 | 3.63 | 4.21 | 4.61 | 8.11 | ||
| ASR | 1.57 | 1.89 | 2.15 | 2.65 | 2.63 | 3.00 | 3.40 | 3.62 | 6.32 | ||
CR, crude rate; ASR, age-standardized rate; MPN, myeloproliferative neoplasm; PV, polycythemia vera; MF, primary myelofibrosis; ET, essential thrombocythemia.
Treatment trends
Hydroxyurea and phlebotomy prescription data available for years 2007 to 2011 are summarized in Table 4. In PV, an average of 61.3% of patients received hydroxyurea, while an average of 39.6% of patients received phlebotomy during the period. In MF, 58.7% received hydroxyurea, and 8.1% phlebotomy; in ET, 61.1% received hydroxyurea and 1.3% phlebotomy. In all diagnoses, the prescription rate of hydroxyurea was higher in older population. However, 20%-40% of patients under 40 years of age were recorded to have been prescribed hydroxyurea (Fig. 3). Over the years, prescription rate for each treatment was kept relatively constant.
Table 4. Trends in prescription of drugs and phlebotomy in myeloproliferative neoplasm (%).
| MPN type | Sex and age | Prescription | 2007 | 2008 | 2009 | 2010 | 2011 | |
|---|---|---|---|---|---|---|---|---|
| PV | Sex | Total | Hydroxyurea | 58.6 | 62.2 | 61.1 | 62.2 | 62.3 |
| Phlebotomy | 39.7 | 39.3 | 39.1 | 40.0 | 39.9 | |||
| Men | Hydroxyurea | 47.7 | 51.4 | 51.1 | 51.9 | 52.2 | ||
| Phlebotomy | 43.2 | 43.6 | 43.6 | 46.3 | 44.9 | |||
| Women | Hydroxyurea | 76.9 | 80.2 | 61.1 | 62.2 | 62.3 | ||
| Phlebotomy | 33.7 | 32.1 | 31.7 | 30.0 | 32.2 | |||
| Age group, yr | Age < 40 | Hydroxyurea | 21.7 | 28.0 | 21.6 | 20.9 | 20.4 | |
| Phlebotomy | 46.0 | 44.6 | 48.9 | 46.8 | 52.2 | |||
| 40 ≤ age < 60 | Hydroxyurea | 49.6 | 54.2 | 52.9 | 52.2 | 53.0 | ||
| Phlebotomy | 50.2 | 50.0 | 47.9 | 50.4 | 49.3 | |||
| Age ≥ 60 | Hydroxyurea | 74.0 | 75.1 | 73.4 | 75.7 | 74.3 | ||
| Phlebotomy | 29.7 | 30.3 | 31.5 | 32.1 | 32.1 | |||
| MF | Sex | Total | Hydroxyurea | 54.6 | 55.0 | 61.1 | 59.4 | 63.6 |
| Phlebotomy | 9.3 | 7.0 | 6.6 | 8.6 | 9.2 | |||
| Men | Hydroxyurea | 52.0 | 52.3 | 51.1 | 55.6 | 60.7 | ||
| Phlebotomy | 11.5 | 8.1 | 7.3 | 10.4 | 11.8 | |||
| Women | Hydroxyurea | 57.1 | 57.7 | 77.5 | 63.3 | 66.5 | ||
| Phlebotomy | 7.1 | 5.8 | 5.8 | 6.9 | 6.5 | |||
| Age group, yr | Age < 40 | Hydroxyurea | 27.8 | 30.0 | 35.0 | 30.4 | 40.5 | |
| Phlebotomy | 9.7 | 7.1 | 7.5 | 3.8 | 7.6 | |||
| 40 ≤ age < 60 | Hydroxyurea | 47.1 | 50.2 | 54.3 | 57.0 | 58.0 | ||
| Phlebotomy | 14.5 | 10.9 | 8.3 | 12.7 | 12.7 | |||
| Age ≥ 60 | Hydroxyurea | 62 | 60.2 | 59.2 | 63.7 | 68.4 | ||
| Phlebotomy | 6.7 | 5.2 | 5.7 | 7.2 | 7.6 | |||
| ET | Sex | Total | Hydroxyurea | 60.6 | 61.7 | 62.4 | 63.5 | 57.5 |
| Phlebotomy | 0.7 | 1.9 | 1.3 | 1.9 | 0.9 | |||
| Men | Hydroxyurea | 58.8 | 60.5 | 62.5 | 62.9 | 56.9 | ||
| Phlebotomy | 1.2 | 2.9 | 2.0 | 2.9 | 1.3 | |||
| Women | Hydroxyurea | 61.9 | 62.5 | 62.3 | 63.9 | 57.9 | ||
| Phlebotomy | 0.4 | 1.1 | 0.9 | 1.3 | 0.6 | |||
| Age group, yr | Age < 40 | Hydroxyurea | 25.1 | 28.2 | 31.4 | 34.7 | 23.7 | |
| Phlebotomy | 0.6 | 1.5 | 1.3 | 0.4 | 1.0 | |||
| 40 ≤ age < 60 | Hydroxyurea | 55.7 | 57.5 | 61.0 | 61.9 | 54.8 | ||
| Phlebotomy | 0.6 | 1.8 | 1.8 | 2.0 | 1.4 | |||
| Age ≥ 60 | Hydroxyurea | 72.8 | 72.4 | 70.3 | 70.5 | 67.6 | ||
| Phlebotomy | 0.9 | 1.9 | 1.0 | 2.2 | 0.6 | |||
MPN, myeloproliferative neoplasm; PV, polycythemia vera; MF, primary myelofibrosis; ET, essential thrombocythemia.
Fig. 3.

The proportion of patients with prescription of hydroxyurea and phlebotomy. (A) Polycythemia vera. (B) Primary myelofibrosis. (C) Essential thrombocythemia.
DISCUSSION
This is the first study to have presented the epidemiological data of classical, Philadelphia-chromosome negative MPN in Korean patients, utilizing comprehensive data from the KNCIDB and the HIRA. The incidence of all PV, MF, and ET constantly increased during the years observed, with the most recent crude annual incidence of PV, MF, and ET being 0.40, 0.15, and 0.84 per 100,000, respectively. The prevalence rates have also increased over the years, most recent crude rates being 4.53, 2.60, and 7.10 per 100,000 for each PV, MF, and ET, by the HIRA data.
Classical MPNs are rare diseases, but as the disease courses are generally long and as the diseases can cause debilitating symptoms and complications, the optimal diagnosis and management is important in enhancing public health. Current guidelines for diagnosis follow the suggestion published by WHO (18) and use blood cell counts, bone marrow results and JAK2 V617F mutation results for diagnosis. More recently, CALR mutation was discovered in JAK2 negative MF and ET patients (10,11), assisting more accurate diagnosis of MPN. Treatment options include low dose aspirin, phlebotomy, and cytoreductive therapy with hydroxyurea, anagrelide, and interferon-α for PV and ET. The classical therapy for MF was bone marrow transplantation. Recently drugs targeting JAK2 mutation has shown very promising results for classical MPN (19,20).
The epidemiological data of classical MPN reported in other countries were generally in similar range with our data, although variable. A US epidemiological study using the North American Association of Central Cancer Registries (NAACCR) and the Surveillance, Epidemiology, and End Results (SEER) Program data reported incidence rates of PV, MF, and ET at 0.79, 0.25, and 0.53 per 100,000 (7). HAEMACARE, a European cancer registry-based project to improve the standardization and availability of population-based data on hematologic malignancies, reported crude incidence rate of MPN excluding chronic myeloid leukemia, at 2.24 per 100,000 (8). A meta-analysis of incidence and prevalence data for classical MPNs published in 2014, suggested the combined annual incidence rates for PV, MF, and ET as 0.84, 0.47, and 1.03 per 100,000, respectively (6). The meta-analysis report included extensive data of which publication dates ranged from 1946 to 2012. Geographically, the study was intended to include all studies without geographical limits and included one Japanese study, but was analyzed using mostly the US and European data. But even considering the racial and geographical difference, the pooled data showed high heterogeneity, showing heterogeneity in data even from similar geographic regions.
The heterogeneity of data between reports and the constant increasing pattern of incidence/prevalence of our data may be owing to a number of factors. The most important cause is the still growing understanding of the disease, and the development of diagnostic tools and disease classifications, accordingly. WHO classification and diagnostic guidelines for MPN has been re-issued in year 2008, and the discovery of JAK2 mutation has led to increased recognition of diseases in the MPN category and to more accurate diagnosis. The discovery of CALR mutation may even lead to further increase in the number of MPN diagnosis in the future. Another attributable factor is that the systemic registrations of the disease category have only recently begun in many countries. MPN have been officially registered in Korea cancer registry since 2003, and since 2001 in the USA. Other additional factors may include the increase in average life span and improved access to healthcare over the years.
This study is the first to present the Korean nationwide epidemiological data of each disease in the classical MPN category. The statistics are important information for clinicians, researchers as well as administrators, on understanding epidemiological characteristics and establishing future strategies on managing MPNs in Korea. The statistics can be utilized to compare the Korean status to international data and guidelines. Continued systemic registration and periodic report is warranted, to improve the accuracy of the data in association with the improvement in the diagnostic accuracy.
ACKNOWLEDGMENT
The content is solely the responsibility of the authors and does not represent the official views of the Korea Central Cancer Registry and Health Insurance Review and Assessment Service. The authors had full responsibility for the design of the study, the analysis and interpretation of the data, and the writing of the manuscript.
Footnotes
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Research conception & design: Bang SM. Data processing and statistical analysis: Lim Y, Lee JO. Data analysis and interpretation: Lim Y. Drafting of the manuscript: Lim Y. Critical revision of the manuscript: Lee JO, Bang SM. Approval of final manuscript: all authors.
References
- 1.Dameshek W. Some speculations on the myeloproliferative syndromes. Blood. 1951;6:372–375. [PubMed] [Google Scholar]
- 2.Tefferi A, Thiele J, Orazi A, Kvasnicka HM, Barbui T, Hanson CA, Barosi G, Verstovsek S, Birgegard G, Mesa R, et al. Proposals and rationale for revision of the World Health Organization diagnostic criteria for polycythemia vera, essential thrombocythemia, and primary myelofibrosis: recommendations from an ad hoc international expert panel. Blood. 2007;110:1092–1097. doi: 10.1182/blood-2007-04-083501. [DOI] [PubMed] [Google Scholar]
- 3.Johansson P. Epidemiology of the myeloproliferative disorders polycythemia vera and essential thrombocythemia. Semin Thromb Hemost. 2006;32:171–173. doi: 10.1055/s-2006-939430. [DOI] [PubMed] [Google Scholar]
- 4.Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55:595–600. doi: 10.3109/10428194.2013.813500. [DOI] [PubMed] [Google Scholar]
- 5.Mehta J, Wang H, Fryzek JP, Iqbal SU, Mesa R. Health resource utilization and cost associated with myeloproliferative neoplasms in a large United States health plan. Leuk Lymphoma. 2014;55:2368–2374. doi: 10.3109/10428194.2013.879127. [DOI] [PubMed] [Google Scholar]
- 6.Titmarsh GJ, Duncombe AS, McMullin MF, O’Rorke M, Mesa R, De Vocht F, Horan S, Fritschi L, Clarke M, Anderson LA. How common are myeloproliferative neoplasms? A systematic review and meta-analysis. Am J Hematol. 2014;89:581–587. doi: 10.1002/ajh.23690. [DOI] [PubMed] [Google Scholar]
- 7.Rollison DE, Howlader N, Smith MT, Strom SS, Merritt WD, Ries LA, Edwards BK, List AF. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001-2004, using data from the NAACCR and SEER programs. Blood. 2008;112:45–52. doi: 10.1182/blood-2008-01-134858. [DOI] [PubMed] [Google Scholar]
- 8.Sant M, Allemani C, Tereanu C, De Angelis R, Capocaccia R, Visser O, Marcos-Gragera R, Maynadié M, Simonetti A, Lutz JM, et al. Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood. 2010;116:3724–3734. doi: 10.1182/blood-2010-05-282632. [DOI] [PubMed] [Google Scholar]
- 9.Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, Swanton S, Vassiliou GS, Bench AJ, Boyd EM, Curtin N. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365:1054–1061. doi: 10.1016/S0140-6736(05)71142-9. [DOI] [PubMed] [Google Scholar]
- 10.Klampfl T, Gisslinger H, Harutyunyan AS, Nivarthi H, Rumi E, Milosevic JD, Them NC, Berg T, Gisslinger B, Pietra D, et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N Engl J Med. 2013;369:2379–2390. doi: 10.1056/NEJMoa1311347. [DOI] [PubMed] [Google Scholar]
- 11.Nangalia J, Massie CE, Baxter EJ, Nice FL, Gundem G, Wedge DC, Avezov E, Li J, Kollmann K, Kent DG, et al. Somatic CALR mutations in myeloproliferative neoplasms with nonmutated JAK2. N Engl J Med. 2013;369:2391–2405. doi: 10.1056/NEJMoa1312542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Park HJ, Park EH, Jung KW, Kong HJ, Won YJ, Lee JY, Yoon JH, Park BK, Lee H, Eom HS, et al. Statistics of hematologic malignancies in Korea: incidence, prevalence and survival rates from 1999 to 2008. Korean J Hematol. 2012;47:28–38. doi: 10.5045/kjh.2012.47.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Park EH, Lee H, Won YJ, Ju HY, Oh CM, Ingabire C, Kong HJ, Park BK, Yoon JY, Eom HS, et al. Nationwide statistical analysis of myeloid malignancies in Korea: incidence and survival rate from 1999 to 2012. Blood Res. 2015;50:204–217. doi: 10.5045/br.2015.50.4.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shin HR, Won YJ, Jung KW, Kong HJ, Yim SH, Lee JK, Noh HI, Lee JK, Pisani P, Park JG. Nationwide cancer incidence in Korea, 1999~2001; first result using the national cancer incidence database. Cancer Res Treat. 2005;37:325–331. doi: 10.4143/crt.2005.37.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM, Whelan S. International Classification of Diseases for Oncology. 3rd ed. Geneva: World Health Organization; 2000. [Google Scholar]
- 16.Kim L, Kim JA, Kim S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol Health. 2014;36:e2014008. doi: 10.4178/epih/e2014008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, et al. SEER Cancer Statistics Review, 1975–2007. Bethesda, MD: National Cancer Institute; 2010. [Google Scholar]
- 18.Tefferi A, Vardiman JW. Classification and diagnosis of myeloproliferative neoplasms: the 2008 World Health Organization criteria and point-of-care diagnostic algorithms. Leukemia. 2008;22:14–22. doi: 10.1038/sj.leu.2404955. [DOI] [PubMed] [Google Scholar]
- 19.Vannucchi AM, Kiladjian JJ, Griesshammer M, Masszi T, Durrant S, Passamonti F, Harrison CN, Pane F, Zachee P, Mesa R, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015;372:426–435. doi: 10.1056/NEJMoa1409002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Verstovsek S, Mesa RA, Gotlib J, Levy RS, Gupta V, DiPersio JF, Catalano JV, Deininger M, Miller C, Silver RT, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366:799–807. doi: 10.1056/NEJMoa1110557. [DOI] [PMC free article] [PubMed] [Google Scholar]