

PRESENTATION
Medical records of a 46-year-old woman with bilateral myopia, gyrate atrophy, and history of night blindness were reviewed. The patient underwent macular hole surgery in the left eye 3 years back. The surgery consisted of pars plana vitrectomy (PPV), induction of posterior vitreous detachment (PVD), internal limiting membrane (ILM) peeling, and fluid-air exchange. She had serum ornithine level of 784 nmole/ml and a best-corrected visual acuity (BCVA) of 1/60 (with correcting lens of −7.25D) in the left eye preoperatively with early posterior subcapsular cataract and a large macular hole (diameter :1254 μm; Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA, USA) with round localized neurosensory retinal detachment at the posterior pole. At month 3 after the operation, 6/60 vision (with correcting lens of -8.00-1.00×100) in the left eye was documented, which remained unchanged. Six months after the operation, she underwent cataract surgery with implantation of a posterior chamber intraocular lens in the capsular bag in the left eye.
At the last follow up examination, 3 years after PPV, intraocular pressure in both eyes was normal, and there was no squint. BCVA was 6/9 in the right eye (with correcting lens of -9.00-3.00×90) and 6/60 in the left eye (with correcting lens of −3D). Fundus examination showed typical coalescent areas of scalloped chorioretinal atrophy in both eyes [Figures 1 and 2]. Right eye had central macular thickness of 151 μm in optical coherence tomography (OCT, Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA, USA) without any evidence of cystic spaces. There was a macular hole in the left eye without surrounding detachment with minimum diameter of 1142 μm, base diameter of 1401 μm, and maximal height of 296 μm [Figure 3].
Figure 1.
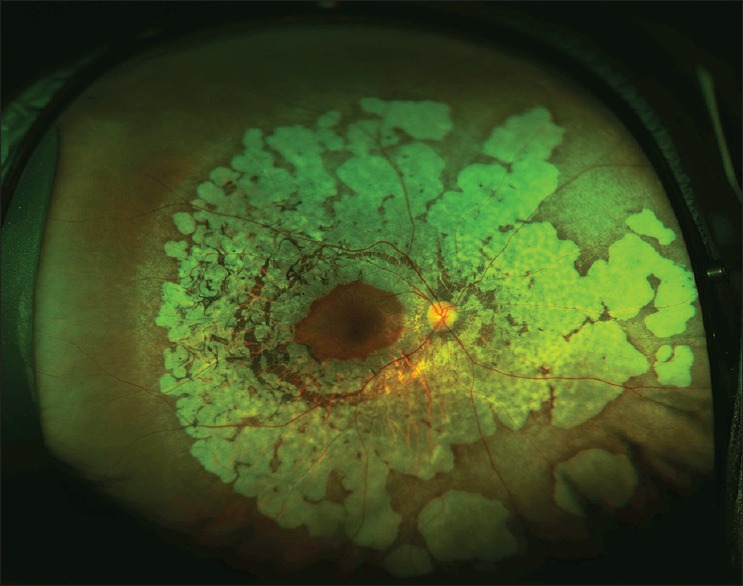
Ultrawide field imaging (Optos, Inc, Marlborough, MA, USA) of the right eye shows typical fundus picture of gyrate atrophy of the choroid and retina.
Figure 2.
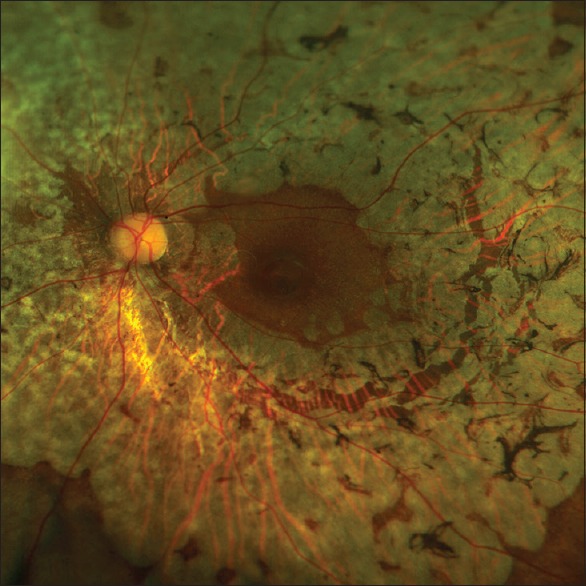
Optomap Resmax′ photo shows open macular hole in the left eye 3 years after surgery.
Figure 3.
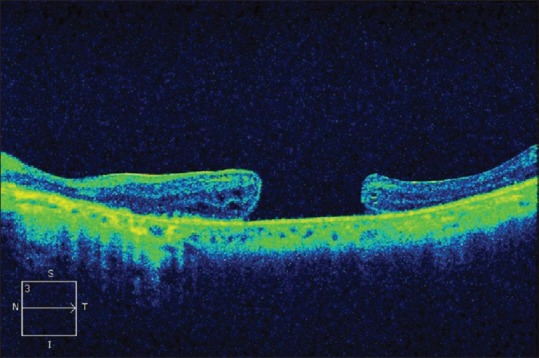
Optical coherence tomogram of the left eye three years after operation shows open macular hole without detachment. Minimum diameter of the macular hole is 1142 μm; base diameter is 1401 μm; and maximal height is 296 μm.
Axial length was 23.83 mm and 23.85 mm in the right and left eyes, respectively. Electroretinogram was extinguished, and Goldmann visual fields were constricted in both eyes. She had been on low dose pyridoxine supplement (15mg/day). In gyrate atrophy, there is reduced activity of ornithine aminotransferase. Pyridoxal phosphate, the active form of pyridoxine is a cofactor for the enzyme. Both low dose (15-18mg/day) and high dose (500-750 mg/day) pyridoxine have been shown to improve the biochemistry and electrophysiology in gyrate atrophy.[1] However, some cases do not respond to the pyridoxine supplement.
DISCUSSION
Ultra-wide field imaging and fluorescein angiography (UWFI and UWFA, Optos, Inc., Marlborough, MA, USA) use scanning laser technology to give a single image of up to 82% or 200° of the retina providing details of peripheral retina.[2] UWFI and UWFA help evaluate the fundus with a single panoramic view in choroidal dystrophies.[3]
Gyrate atrophy is a rare autosomal recessive chorioretinal dystrophy characterized by sharply demarcated circular or oval areas of chorioretinal atrophy in the midperiphery of the fundus which are initially separate and become confluent with time. Macular changes including cystoid macular edema, epiretinal membrane,[4] and choroidal neovascular membrane [5] have been reported in this disease.
Macular hole is a rare finding in gyrate atrophy. The only report of bilateral macular holes with surrounding cuff of subretinal fluid in gyrate atrophy in the indexed peer-reviewed literature has previously been reported by the authors.[6] The pathogenesis of macular hole may involve pathological myopia, vitreomacular traction, coalescence and un-roofing of foveal cysts, contraction of premacular vitreous cortex, and PVD.[7] There was no posterior staphyloma in this case, and PVD had to be induced during macular hole surgery. Cystoid macular edema or cystic spaces in macula due to gyrate atrophy may have led to macular hole formation. This case may also have been an idiopathic macular hole. Surgical closure could not be achieved in our case because of the large initial diameter of the hole. However, macular attachment led to improvement in BCVA after surgery. PPV and ILM peeling may be considered in large macular holes with macular detachment in gyrate atrophy and may improve central vision in these eyes with already compromised peripheral vision. UWFI is useful in documenting retinal pathologies in a single panoramic 200° image.
Acknowledgments
We sincerely acknowledge invaluable support and suggestion by Trina Sengupta Tripathy, without which the manuscript would have been incomplete.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Weleber RG, Kennaway NG. Clinical trial of vitamin B6 for gyrate atrophy of the choroid and retina. Ophthalmology. 1981;88:316–24. doi: 10.1016/s0161-6420(81)35035-0. [DOI] [PubMed] [Google Scholar]
- 2.Witmer MT, Kiss S. Wide-field imaging of the retina. Surv Ophthalmol. 2013;58:143–154. doi: 10.1016/j.survophthal.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 3.Yuan A, Kaines A, Jain A, Reddy S, Schwartz SD, Sarraf D. Ultra-wide-field and autofluorescence imaging of choroidal dystrophies. Ophthalmic Surg Lasers Imaging. 2010;41 Online:e1–5. doi: 10.3928/15428877-20101025-10. [DOI] [PubMed] [Google Scholar]
- 4.Tripathy K, Chawla R, Sharma Y, Gogia V. Ultrawide field fluorescein angiogram in a family with gyrate atrophy and foveoschisis. Oman J Ophthalmol. 2016;9:104–6. doi: 10.4103/0974-620X.184529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Marano F, Deutman AF, Pinckers AJ, Aandekerk AL. Gyrate atrophy and choroidal neovascularization. Arch Ophthalmol. 1996;114:1295. doi: 10.1001/archopht.1996.01100140495035. [DOI] [PubMed] [Google Scholar]
- 6.Sharma YR, Singh DV, Azad RV, Pal N. Gyrate atrophy with bilateral full thickness macular hole. Eye. 2006;20:745–747. doi: 10.1038/sj.eye.6702009. [DOI] [PubMed] [Google Scholar]
- 7.Gaudric A, Tadayoni R. Macular hole. In: Ryan SJ, editor. Retina. 5th ed. London, UK: Saunders/Elsevier; 2013. pp. 1962–78. [Google Scholar]