

Abstract
Statement of Problem:
Many methods are reported in literature to determine freeway space (FWS), but they yield dissimilar measurements.
Purpose:
Recording FWS of patients during prosthetic rehabilitation is one of the important steps in dentistry. The purpose of this study is to evaluate the ability to predict FWS using lateral profile photographs (LPPs) in edentulous participants.
Materials and Methods:
Fifty-three participants in the age range of 20–27 years who met the inclusion criteria were recruited. LPP were taken for all participants using standard protocol and duplicate copy obtained; on which three soft tissue reference points, porion (Stp), gnathion (Stgn), and gonion (Stg) (Stg prenoted on the face) were marked and joined to form an angle Stp-Stg-Stgn. This angle was correlated with the mean FWS obtained using 3 methods, swallowing, phonetics, and no command. Simple linear regression model was used to develop a prediction formula for FWS using Stp-Stg-Stgn angle as the independent variable.
Results:
The angle Stp-Stg-Stgn had a significant negative correlation with FWS (r = −0.76, P < 0.001). Using simple linear regression analysis, the following formula was obtained: FWS (in millimeters) = 11.405 − 0.072 × (Stp-Stg-Stgn angle in degrees).
Conclusion:
Within the limitations of this study, considering the usage of LPP as a method to determine the FWS can be recommended.
Keywords: Anatomical landmarks, soft tissue, vertical dimension at rest
INTRODUCTION
Rest position, also called as interocclusal rest position or freeway space (FWS), has been defined as the neutral position attained by the mandible as it is involuntarily suspended by the reciprocal coordination of the elevator and depressor masticatory muscles with the maxillary and mandibular teeth separated. It is the primary prerequisite for comfort and optimum function of partial or complete dentures, as it is expressed as a gap that occurs in the vertical dimension separating the position which the mandible assumes in space when it is at rest, and its spatial position when the teeth are brought into contact.[1] Encroaching upon the normal space leads to constant undue stimulus to the stretch reflex of the masticatory muscles which promotes excessive muscle contractions and in turn affects teeth, periodontium, supporting tissues, masticatory muscles, and temporomandibular joint. This finally results in the establishment of proper FWS at the expense of the alveolar bone. On the other hand, providing too much space leads to the serious disadvantage of masticatory muscles.[1] Hence, when designing dentures, the previously occurring precise level should be redefined and in the case of inexistence of records, the reintroduction of contact is totally subjected to empirical principles.
Though FWS seems easily accessible, it is one of the controversial topics in prosthetic dentistry. It is the basic introductory step in jaw relations on which further complicated ones, like vertical dimension and centric relation, are contingent upon.[2] Hence, the knowledge about the precise level at which this lost dimension previously occurred is very important as the correct horizontal relation depended on the correct vertical relations, and any alteration in these dimensions can affect the stomatognathic system.[3] Numerous researches have tried to develop an exact technique, either mechanically or physiologically or using a combination of both, so as to determine proper vertical dimension and FWS, but with controversial interpretations.[4,5,6,7,8,9] This indicates constant reevaluation, revision of the concept, need for further research to explore the ways that can help in easy and precise determination of FWS as any denture designed should coincide with the functional equilibrium.
The amount of FWS in any individual is mainly an expression of muscle function, its equilibrium and gravity.[10,11] When the tension created by the muscles of mastication that elevate the mandible above is in equilibrium with the tension of the musculature that depress the mandible from below and gravity, then the mandible will be theoretically at rest. However, it is also reported that the FWS is not coinciding with the minimal muscle activity.[12] Thus, with the exclusion of muscular activity as a means of determining the extent of FWS, the only alternative is the identification of another anatomical feature, the nature of which will also be subject to modification by the effect of the muscle force and unaffected by the changes caused due to loss of teeth. As proposed by the Wolff's law, the muscular functional forces not only influence the FWS but also are responsible for shaping of the internal bone.[13] Based on this concept, the correlation between FWS and structure of the lower facial skeleton has been studied. One study done on the relationship with the form of the lower face found a negative correlation of FWS with the anterior lower facial height and positive with the posterior lower facial height;[14] whereas another cephalometric study done on the relationship with the gonial angle found a statistically significant negative correlation.[1] Thus, the only anatomical feature proved to correlate with FWS and confirm to all the requirements is the gonial angle of the mandible.[1] As the soft tissue profile of an individual depends on the bony structure, this study was planned to evaluate the correlation of the FWS and corresponding soft tissue gonial angle formed on the lateral profile of edentulous individuals in photographs.
MATERIALS AND METHODS
Ethical clearance for the study was obtained from the Institutional Ethical Committee. The participants within the age range of 20–27 years with a full complement of teeth, well-balanced face, Class I skeletal, molar and canine relationship, no acute or previous temporomandibular disorder, and those who were willing to participate were selected. Individuals with previous orthodontic treatment, those with facial asymmetries, caries, history of extractions, temporomandibular joint problems, or having occlusal prematurities were excluded. Out of the screened 400 potential participants, 53 met the criteria and written consent was obtained from them, before inclusion in the study.
Lateral profile photography
The lateral profiles were taken following the standards of extraoral photography using Nikon D3300 SLR camera.[15] The participants were instructed to stand straight with their head in natural position achieved by asking them to look into the mirror hung on the wall at their eye level. After confirming that the line drawn from the outer canthus of the eye and upper edge of the ear was parallel to the floor, photographs were taken from a distance of 5 feet [Figure 1].
Figure 1.

Participant standing straight by looking into mirror hung on wall at eye level
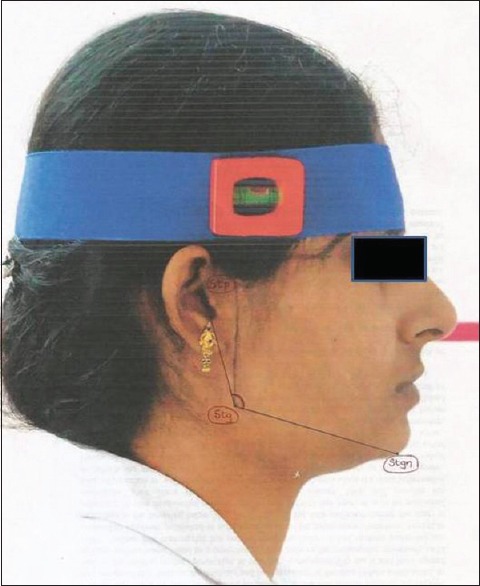
Soft tissue reference points
The following points were considered in this study:
Point corresponding to porion (Stp): The most superiorly positioned point on the external opening of the auditory meatus
Skin gnathion (Stgn): The point where the anterior curve in the outline of the chin merges into the body of the mandible
Gonion (Stg): A point on the curvature of the angle of the mandible formed by the ascending ramus and the inferior border of the mandible.
Procedure
The participant was positioned in a chair comfortably, and a line connecting the outer canthus of the eye and superior edge of the ear was drawn. The point gonion was palpated by the left thumb and without leaving the finger from the face a perpendicular line was drawn using a set square from the line drawn on the face half way to the tip of the thumb and was extended to the lower border of the mandible after leaving the finger [Figure 2a–c]. Now, the participant was instructed to stand for the photograph after which duplicate was obtained by cropping it to the dimension 8 inches × 10 inches. All the soft tissue reference points were marked on the duplicate photograph and joined to form an angle (Stp-Stg-Stgn) which was measured [Figure 3].
Figure 2.
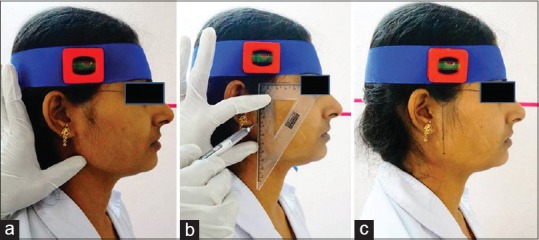
(a-c) Marking point gonion on face of participant
Figure 3.

Lateral profile photograph of participant
Reproducibility of the Stp-Stg-Stgn on the face
To test the reproducibility of this angle on the face, 15 participants were randomly selected among 53 subjects enrolled in present investigation and lateral cephalograms were obtained after placing lead markers on soft tissue corresponding to porion, gonion, and gnathion areas [Figure 4]. By tracing these points on acetate paper, the angle formed between them was calculated.
Figure 4.
Scanned carbon copy of lateral photograph with marked Stp-Stgn-Stg angle
Freeway space determination
Three methods, swallowing, phonetics, and no commands, were employed to determine the rest position of the mandible. The mean value of the above-mentioned methods was calculated and considered as the FWS of that particular person.
Reliability of photographs and freeway space determination
To test the reliability of the obtained data, the lateral profile analysis, and FWS determination was repeated, for 5 randomly selected participants, by the same investigator (DV), and by another investigator (KK).
Statistical analysis
All statistical analyses were performed using SPSS 17.0 software (version 17.0, SPSS, Chicago, IL, USA). Cohen's kappa was employed to measure the reliability of lateral profile analysis and FWS (both intra-rater and inter-rater). The normality of the data was tested using Shapiro–Wilk test and all the data were found to be normally distributed. The reproducibility of the angle Stp-Stg-Stgn on the face was tested using Pearson correlation test. The correlation between the angle, Stp-Stg-Stgn, and FWS was also determined using Pearson correlation test and for predicting the FWS from the considered angle, simple linear regression analysis was carried out. Again, the predicted FWS values and actual measured values were correlated using Pearson correlation test.
Sample size determination
Based on the findings of our pilot study on 18 participants, with the level of significance set at 0.05, power of 80%, a minimal sample size of 50 was determined.
RESULTS
The mean age of the 53 participants (20 male and 33 female) was 22.4 (age range of 20–27 years). The mean Stp-Stg-Stgn angle was found to be 129.13 ± 6.74 (minimum: 114; maximum: 147). The mean ± standard deviation (SD) of FWS obtained through swallowing, phonetics, and no command methods were 1.87 ± 0.58, 2.3 ± 0.59, and 2.1 ± 0.70, respectively, (phonetics > no commands > swallowing). The range of the FWS obtained through the above-mentioned three methods was found to be between 1.24 and 3.67 mm (mean ± SD: 2.09 ± 0.64).
The intra-rater and inter-rater reliability of the lateral profile analysis were found to be 0.99 and 0.95, respectively (angle variation of 2–3°), whereas those for FWS were 0.92 and 0.89, respectively. The correlation between Stp-Stg-Stgn marked on the face and on the radiograph was found to be r = 0.906, P < 0.001***; thus the determination coefficient was r2= 82% [Figure 5]. Thus, a strong positive correlation was observed between the two. The correlation between Stp-Stg-Stgn and FWS was found to be r = –0.76, P < 0.001***; thus the determination coefficient was r2= 57.8% [Figure 6]. A strong negative correlation which was statistically significant was found between the considered angle and FWS. Hence, a linear regression equation was determined to predict FWS with the considered angle as a predictor. The equation determined was calculated as, y = a + bx where “y” is the dependent variable, i.e. FWS, “x” is the independent variable, i.e. Stp-Stg-Stgn, “a” is the y-intercept, and “b” is the slope of regression. Calculation resulted in the following formula, y = 11.405 − 0.072x. Thus, the formula determined was FWS (in millimeters) = 11.405 − 0.072 × (Stp-Stg-Stgn angle in degrees). Based on this new equation, the predicted values of FWS were calculated which gave a mean ± SD value of 2.11 ± 0.48. The difference between the predicted and actual were again correlated which gave a strong positive correlation coefficient of 0.847 [Figure 7].
Figure 5.
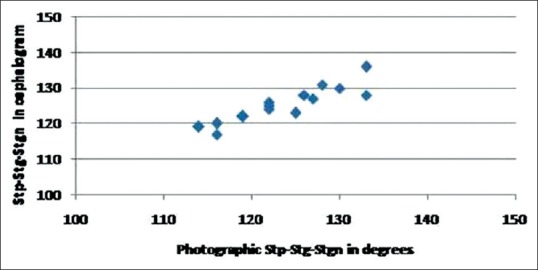
Correlation of Stp-Stgn-Stg angle in photograph and cephalogram
Figure 6.
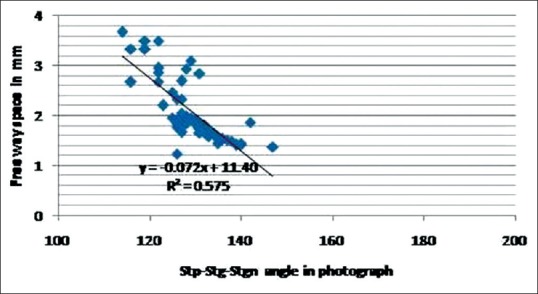
Correlation of Stp-Stgn-Stg angle in photograph and freeway space
Figure 7.
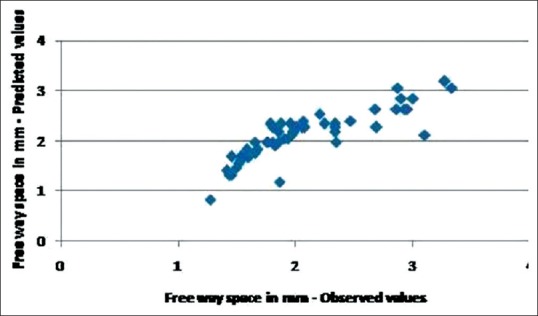
Correlation between freeway space – observed and predicted values
DISCUSSION
The gonial angle was believed to correlate with the function and shape of the muscles of mastication, mainly masseter and medial pterygoid; these muscles insert into the region of the gonial angle and influence the shape of the mandibular base. As the contractile force of these muscles increase, the angle will be more acute and lesser the force the more obtuse it will be. Thus, studies had proved that strong muscle activity correlate with the small anterofacial height and small gonial angle.[16,17,18,19] The FWS and gonial angle were inversely related to each other as proved in a cephalometric study.[1] The radiographic gonial angle, as noted in this study, was correlating well with the Stp-Stg-Stgn angle in the photograph (corresponding soft tissue gonial angle); hence, photograph instead of a cephalogram was opted as a cost-effective alternative for the patient and dentist convenience.
FWS was described in two ways, adaptive and true FWS.[12] The space that exists when the patient is instructed to voluntarily allow the jaw to relax is the adaptive space, whereas the one that is present after the relaxation of the masticatory musculature is the true FWS. However, the clinical rest position was not coincident with minimal muscle activity as proved in electromyographic and kinesiographic studies.[12] The FWS is affected by many factors; opening the mouth for an extended period of time, as it happens during our clinical procedures, and chewing hard substances can have a profound effect. The muscles that control the mandible can also become tense when any type of mechanical recording device is placed in the mouth or on the head.[20] Thus, cephalometry was proposed to be an effective method, as it uses specific and predetermined point of bone references to obtain exact measurements.[1] However, they have certain drawbacks such as picture deformations, superposition of structures, the inaccuracy of cephalometric tracing, and also radiation exposure. This highlights the necessity to explore for some easier ways that help to record the relations without any inconvenience for the patient, as done in this study with profile photographs avoiding the above-mentioned problems. By following the exact protocol, standard appearance can be retained with simple reproduction of a photograph in the same manner at different time intervals.[15] Even minor variations in photography have minimal effect on the points and angles in a photograph as observed in the reliability values of this study. The variation in the angle was in the range of 2–3°, which had a negligible effect on the prediction of FWS. The chubbiness in the cheek area was also not a problem in our study; the point gonion could be easily palpated without any difficulty.
A very strong negative correlation was observed between FWS and the considered angle on the soft tissue profile, which encourages the usage of this method for the determination of the FWS. Though there was a good correlation between the predicted and measured values; on employing the formula for Stp-Stg-Stgn angles >140°, a small value for FWS will be calculated (in this study, the highest angle reported was 147°, for which the FWS calculated was 1.24 mm). This can be attributed to the coefficient of determination which cautions the possibility of inaccuracies in certain cases. Hence, for angle calculations >140°, either more conventional methods to calculate FWS are recommended additionally, or the minimal FWS of 1.5 mm can be considered.
The concept of using Stp-Stg-Stgn angle for the determination of FWS can be generalized to all the population, but the proposed formula in this study cannot separate formulae for people in other geographic regions are recommended. The current study population was limited to angles Class I subjects, and, therefore, it remains indeterminate as to whether or not this method of calculation can be extrapolated to other skeletal classifications. Further investigation would need to be done to substantiate that FWS calculated with the proposed method in the present investigation could demonstrate that it is no different as regards outcome for other angle's classifications as observed in some studies.[12,21]
CONCLUSION
Within the limitations of this study, Stp-Stg-Stgn angle was correlating well with the FWS and hence this new method can be recommended along with other standard ones. Additional studies are also required in this area on edentulous patients. Further studies on photographs as a means of determining the lost facial dimensions can be advocated.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Potgieter PJ, Monteith BD, Kemp PL. The determination of free-way space in edentulous patients: A cephalometric approach. J Oral Rehabil. 1983;10:283–93. doi: 10.1111/j.1365-2842.1983.tb00123.x. [DOI] [PubMed] [Google Scholar]
- 2.Shpuntoff BH, Shpuntoff WA. A study of physiologic rest position and centric position by electromyography. J Prosthet Dent. 1956;6:621–8. [Google Scholar]
- 3.Monteith B. The role of the free-way space in the generation of muscle pain among denture-wearers. J Oral Rehabil. 1984;11:483–98. doi: 10.1111/j.1365-2842.1984.tb00601.x. [DOI] [PubMed] [Google Scholar]
- 4.Silverman MM. The speaking method in measuring vertical dimension. J Prosthet Dent. 1953;3:193–9. doi: 10.1067/mpr.2001.116139. [DOI] [PubMed] [Google Scholar]
- 5.Burnett CA, Clifford TJ. Closest speaking space during the production of sibilant sounds and its value in establishing the vertical dimension of occlusion. J Dent Res. 1993;72:964–7. doi: 10.1177/00220345930720061201. [DOI] [PubMed] [Google Scholar]
- 6.Morrison ML. Phonetics as a method of determining vertical dimension and centric relation. J Am Dent Assoc. 1959;59:690–5. doi: 10.14219/jada.archive.1959.0205. [DOI] [PubMed] [Google Scholar]
- 7.Niswonger ME. The rest position of the mandible and the centric relation. J Am Dent Assoc. 1934;21:1572. [Google Scholar]
- 8.Gillis RR. Establishing vertical dimension in full denture construction. J Am Dent Assoc. 1941;28:430. [Google Scholar]
- 9.Rizzatti A, Ceruti P, Mussano F, Erovigni F, Preti G. A new clinical method for evaluating the closest speaking space in dentulous and edentulous subjects: A pilot study. Int J Prosthodont. 2007;20:259–62. [PubMed] [Google Scholar]
- 10.Eriksson PO. Muscle-fibre composition of the human mandibular locomotor system. Enzyme-histochemical and morphological characteristics of functionally different parts. Swed Dent J. 1982;12:1–44. [PubMed] [Google Scholar]
- 11.Moller E. Evidence that the rest position is subject to servo-control. In: Andreson DJ, Matthews B, editors. Mastication. Bristol: John Wright and Sons; 1976. p. 72. [Google Scholar]
- 12.Konchak PA, Thomas NR, Lanigan DT, Devon RM. Freeway space measurement using mandibular kinesiograph and EMG before and after TENS. Angle Orthod. 1988;58:343–50. doi: 10.1043/0003-3219(1988)058<0343:FSMUMK>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Wolff J. Blakiston's New Gould Medical Dictionary. 1st ed. Philadelphia: Blakiston Company; 1949. [Google Scholar]
- 14.Lindegard B. Variations in human body build. Acta Psychol Neurol. 1953;86:87. [PubMed] [Google Scholar]
- 15.Anic-Milosevic S, Slaj M, Lapter-Varga M. Basic principles for taking extraoral photographs. Acta Stomatol Croat. 2005;39:201–4. [Google Scholar]
- 16.Huumonen S, Sipilä K, Haikola B, Tapio M, Söderholm AL, Remes-Lyly T, et al. Influence of edentulousness on gonial angle, ramus and condylar height. J Oral Rehabil. 2010;37:34–8. doi: 10.1111/j.1365-2842.2009.02022.x. [DOI] [PubMed] [Google Scholar]
- 17.Moller E. The chewing apparatus. An electromyographic study of the action of the muscles of mastication and its correlation to facial morphology. Acta Physiol Scand Suppl. 1966;280:1–229. [PubMed] [Google Scholar]
- 18.Ingervall B, Thilander B. Relation between facial morphology and activity of the masticatory muscles. J Oral Rehabil. 1974;1:131–47. doi: 10.1111/j.1365-2842.1974.tb00771.x. [DOI] [PubMed] [Google Scholar]
- 19.Orthlieb JD, Laurent M, Laplanche O. Cephalometric estimation of vertical dimension of occlusion. J Oral Rehabil. 2000;27:802–7. doi: 10.1046/j.1365-2842.2000.00592.x. [DOI] [PubMed] [Google Scholar]
- 20.Tzakis M, Carlsson GE, Kiliaridis S. Effect of chewing training on mandibular postural position. J Oral Rehabil. 1989;16:503–8. doi: 10.1111/j.1365-2842.1989.tb01371.x. [DOI] [PubMed] [Google Scholar]
- 21.Sakar O, Bural C, Sülün T, Öztas E, Marsan G. Evaluation of the closest speaking space in different dental and skeletal occlusions. J Prosthet Dent. 2013;109:222–6. doi: 10.1016/S0022-3913(13)60048-7. [DOI] [PubMed] [Google Scholar]