

Abstract
Background
Acupuncture is considered a complementary and alternative medicine in many countries. The purpose of this study was to report the pattern of acupuncture use and associated factors in patients with stroke.
Methods
We used claims data from Taiwan’s National Health Insurance Research Database and identified 285001 new-onset stroke patients in 2000–2008 from 23 million people allover Taiwan. The use of acupuncture treatment after stroke within one year was identified. We compared sociodemographics, coexisting medical conditions, and stroke characteristics between stroke patients who did and did not receive acupuncture treatment.
Results
The use of acupuncture in stroke patients increased from 2000 to 2008. Female gender, younger age, white-collar employee status, higher income, and residence in areas with more traditional Chinese medicine (TCM) physicians were factors associated with acupuncture use in stroke patients. Ischemic stroke (odds ratio [OR] 1.21, 95 % confidence interval [CI] 1.15–1.28), having no renal dialysis (OR 2.76, 95 % CI 2.45–3.13), receiving rehabilitation (OR 3.20, 95 % CI 3.13–3.27) and longer hospitalization (OR 1.23, 95 % CI 1.19–1.27) were also associated with acupuncture use. Stroke patients using rehabilitation services were more likely to have more acupuncture visits and a higher expenditure on acupuncture compared with stroke patients who did not receive rehabilitation services.
Conclusions
The application of acupuncture in stroke patients is well accepted and increasing in Taiwan. The use of acupuncture in stroke patients is associated with sociodemographic factors and clinical characteristics.
Keywords: Acupuncture, Complementary and alternative medicine, Stroke, Traditional Chinese medicine, Use
Background
With the increasing use of complementary and alternative medicine (CAM) worldwide [1], the 1-year prevalence of CAM use in the United States and United Kingdom were found to be as high as 33.2 % and 26.3 %, respectively [2, 3]. The estimated out-of-pocket cost for CAM was $33.9 billion in the USA in 2007 [4]. Acupuncture is considered a subtype of traditional Chinese medicine (TCM) [5], which has been used for at least 2000 years in China, and it has gained attention in the United States since 1971. Currently, it is widely used in many countries [1, 5]. A cross-sectional survey showed that at least 1.5 % of adults had used acupuncture in the past 12 months in the United States in 2007 [6].
Stroke remains the leading cause of adult disabilities worldwide, with an estimated direct medical cost of $20.6 billion in the United States in 2010 [7]. The 1-year cost of stroke ranges from $7,342 to $146,149 per patient in several countries [8]. Pneumonia, urinary tract infection, pain, dysphagia, depression, and recurrent stroke are common complications after stroke [9–11].
Acupuncture has been accepted in stroke rehabilitation in many countries, and the treatment is relatively safe and effective in improving post-stroke chronic symptoms, such as disability, shoulder pain, and dysphagia [5, 12–15]. In the United States, acupuncture was used more frequently in stroke compared with non-stroke patients [16]. A previous study also showed the high use of TCM among stroke patients in Taiwan [17]. However, limited information is available on the pattern of use of acupuncture in stroke patients.
Using the National Health Insurance Research Database, we conducted a nationwide, population-based cohort study to evaluate the pattern of acupuncture use in stroke patients. Another purpose of this study was to report the factors associated with acupuncture use among adult stroke patients.
Methods
Source of data
Since 1996, all medical claims of insured beneficiaries have been documented in the National Health Insurance Research Database, which was established by Taiwan’s National Health Research Institute. Information available for this study included gender, birth date, disease codes, health care rendered, medicines prescribed, diagnoses at admission and discharge, and medical institutions and physicians providing services. This study employed the All Stroke Database, which consisted of all prevalent and incident stroke patients across Taiwan between 2000 and 2008 [17–19].
Ethical statement
Insurance reimbursement claims used in this study were obtained from Taiwan’s National Health Insurance Research Database, which is available for academic access. This study was conducted in accordance with the Helsinki Declaration. To protect personal privacy, the electronic database was decoded with patient identifications scrambled for further public access for research. Although the National Health Research Institute regulations do not require informed consent due to the use of decoded and scrambled patient identification, this study was approved by Taiwan’s National Health Research Institute (NHIRD-100-122) and the Institutional Review Board of E-DA Hospital, Kaohsiung, Taiwan (2014012) [17–19].
Study design and population
We identified 285001 newly diagnosed, hospitalized stroke patients aged ≥20 years between 2000 and 2008 as our eligible study subjects from 23 million people allover Taiwan. Those with a previous stroke according to a physician’s diagnosis were excluded until 1996. To confirm that all stroke patients in our study were incident cases, only new-onset stroke cases were included. The outcome of this study was the prevalence of acupuncture use in people with a new diagnosis of stroke in the first year. This study compared sociodemographic factors, coexisting medical conditions, and stroke characteristics between stroke patients who used and did not use acupuncture.
Criteria and definition
We defined stroke according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM 430–438). Coexisting medical conditions included diabetes mellitus (ICD-9-CM 250), hypertension (ICD-9-CM 401–405), hyperlipidemia (ICD-9-CM 272.0–272.4), and myocardial infarction (ICD-9-CM 410 and 412). According to the administration codes (D8, D9) from reimbursement claims, regular renal dialysis (including hemodialysis and/or peritoneal dialysis) was also considered a coexisting medical condition among stroke patients in this study. We classified the frequency of acupuncture visits into quartiles. Stroke patients in the highest quartile of acupuncture visits were defined as high acupuncture users. Medical expenditures on acupuncture were also classified into quartiles. Stroke patients who were in the highest quartile of acupuncture expenditure were considered high acupuncture expenditure patients.
As Taiwan has 359 townships and city districts, we calculated the population density (persons/km2) of each of these administrative units. Based on the population density, these units were stratified into tertiles to designate areas of low, moderate, and high urbanization. We calculated the density of traditional Chinese physicians (traditional Chinese physicians/10,000 persons) based on the number of traditional Chinese physicians per 10,000 residents in each administrative unit. The first, second, and third tertiles were considered areas with low, moderate, and high physician densities, respectively. Based on the Ministry of Health and Welfare criteria, low income status was defined as qualification for waived medical co-payments.
Statistical analysis
To observe the trend of acupuncture use, the annual prevalence of stroke patients using acupuncture treatment was calculated from 2000 to 2008. We used chi-square tests to compare the difference in sociodemographics, coexisting medical conditions, and characteristics of hospitalization between stroke patients who did and did not use acupuncture. Univariate and multivariate logistic regression analyses were performed to calculate crude and adjusted odds ratios (ORs) and 95 % confidence intervals (CIs) that measured the relationships between acupuncture use and associated characteristics in stroke patients. These characteristics included sex, age, income status, occupation, urbanization, density of traditional Chinese physicians in the area, disease history, use of rehabilitation, type of stroke, and in-hospital characteristics. All analyses were performed using Statistical Analysis Software version 9.1 (SAS Institute Inc., Cary, North Carolina, USA). A two-sided probability value of <0.05 was considered statistically significant.
Results
The prevalence of acupuncture use among stroke patients increased from 12 % in 2000 to 17 % in 2008 (p < 0.0001) (Fig. 1). A higher incidence of acupuncture use was found in men, younger patients, higher income people, white-collar employees, residents living in highly urbanized areas, and areas with more TCM physicians.
Fig. 1.
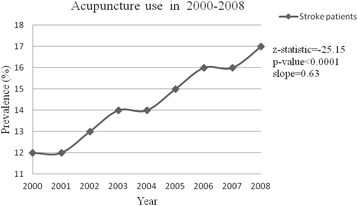
Prevalence of Acupuncture use among stroke patients in Taiwan from 2000–2008 (*Cochran-Armitage Trend Test)
The multivariate logistic regression analysis yielded the ORs of factors associated with acupuncture use in stroke patients (Tables 1 and 2), including female gender (OR 1.04, 95 % CI 1.01–1.06), age 30–39 years (OR 4.05, 95 % CI 3.77–4.36), very high income status (OR 1.55, 95 % CI 1.47–1.65), white-collar employee status (OR 1.16, 95 % CI 1.12–1.20), residence in highly urbanized areas (OR 1.44, 95 % CI 1.37–1.52), residence in areas with more TCM physicians (OR 1.43, 95 % CI 1.39–1.48), and use of other types of rehabilitation (OR 3.20, 95 % CI 3.13–3.27). Acupuncture users also experienced greater incidences of hypertension (OR 1.18, 95 % CI 1.15–1.21) and hyperlipidemia (OR 1.30, 95 % CI 1.26–1.35) but lower incidences of myocardial infarction (OR 1.18, 95 % CI 1.09–1.28) and renal dialysis (OR 2.76, 95 % CI 2.45–3.13). Ischemic stroke (OR 1.21, 95 % CI 1.15–1.28) and longer hospitalization (OR 1.23, 95 % CI 1.19–1.27) were also associated with acupuncture use.
Table 1.
Comparison of sociodemographic characteristics between stroke patients with and without acupuncture treatment in 2000–2008
| Acupuncture use | p-value | OR | (95 % CI)* | ||||
|---|---|---|---|---|---|---|---|
| No (N = 242213) | Yes (N = 42788) | ||||||
| Sex | n | (%) | n | (%) | <0.0001 | ||
| Women | 101,397 | (85.5) | 17,225 | (14.5) | 1.04 | (1.01–1.06) | |
| Men | 140,816 | (84.6) | 25,563 | (15.4) | 1.00 | (reference) | |
| Age, years | <0.0001 | ||||||
| 20–29 | 1819 | (83.1) | 369 | (16.9) | 3.44 | (3.04–3.89) | |
| 30–39 | 5680 | (78.9) | 1517 | (21.1) | 4.05 | (3.77–4.36) | |
| 40–49 | 20,319 | (79.3) | 5298 | (20.7) | 3.79 | (3.60–4.00) | |
| 50–59 | 39,190 | (79.6) | 10,054 | (20.4) | 3.56 | (3.39–3.73) | |
| 60–69 | 58,684 | (82.6) | 12,374 | (17.4) | 3.05 | (2.91–3.18) | |
| 70–79 | 74,891 | (87.8) | 10,424 | (12.2) | 2.04 | (1.95–2.13) | |
| ≥ 80 | 41,630 | (93.8) | 2752 | (6.2) | 1.00 | (reference) | |
| Mean ± SD | 67.4 ± 13.3 | 62.5 ± 12.5 | <0.0001 | ||||
| Income | <0.0001 | ||||||
| Very low | 13,611 | (86.1) | 2203 | (13.9) | 1.00 | (reference) | |
| Low | 71,645 | (85.4) | 12,283 | (14.6) | 1.23 | (1.16–1.30) | |
| Moderate | 42,567 | (84.9) | 7565 | (15.1) | 1.31 | (1.24–1.38) | |
| High | 88,550 | (87.1) | 13,152 | (12.9) | 1.30 | (1.23–1.38) | |
| Very high | 25,840 | (77.3) | 7585 | (22.7) | 1.55 | (1.47–1.65) | |
| Occupation | <0.0001 | ||||||
| White collar | 73,946 | (82.0) | 16,188 | (18.0) | 1.16 | (1.12–1.20) | |
| Blue collar | 115,906 | (86.5) | 18,067 | (13.5) | 1.00 | (reference) | |
| Other | 52,361 | (86.0) | 8533 | (14.0) | 1.06 | (1.02–1.11) | |
| Urbanization | <0.0001 | ||||||
| Low | 17,323 | (90.3) | 1858 | (9.7) | 1.00 | (reference) | |
| Moderate | 93,336 | (87.4) | 13,509 | (12.6) | 1.21 | (1.15–1.28) | |
| High | 131,554 | (82.8) | 27,421 | (17.3) | 1.44 | (1.37–1.52) | |
| Density of TCM | <0.0001 | ||||||
| Low | 64,074 | (88.8) | 8117 | (11.2) | 1.00 | (reference) | |
| Moderate | 121,661 | (84.6) | 22,199 | (15.4) | 1.17 | (1.14–1.21) | |
| High | 56,478 | (81.9) | 12,472 | (18.1) | 1.43 | (1.39–1.48) | |
| Mean ± SD | 1.6 ± 1.2 | 1.8 ± 1.3 | <0.0001 | ||||
*Logistic regression model included sociodemographics and medical conditions; Hosmer-Lemeshow goodness of fit, p-value = 0.0006; c-statistic = 0.71; CI, confidence interval; OR, odds ratio; TCM, traditional Chinese medicine
Table 2.
Medical conditions of stroke patients with and without acupuncture treatment in 2000–2008
| Acupuncture | |||||||
|---|---|---|---|---|---|---|---|
| No (N = 285329) | Yes (N = 47832) | p-value | OR | (95 % CI)* | |||
| Rehabilitation | <0.0001 | ||||||
| No | 166,526 | (90.7) | 17,087 | (9.2) | 1.00 | (reference) | |
| Yes | 75,687 | (74.7) | 25,701 | (25.3) | 3.20 | (3.13–3.27) | |
| Diabetes | <0.0001 | ||||||
| No | 172,698 | (85.2) | 29,983 | (14.8) | 1.00 | (reference) | |
| Yes | 69,515 | (84.4) | 12,805 | (15.6) | 1.00 | (0.98–1.03) | |
| Hypertension | <0.0001 | ||||||
| No | 93,695 | (86.0) | 15,290 | (14.0) | 1.00 | (reference) | |
| Yes | 148,518 | (84.4) | 27,498 | (15.6) | 1.18 | (1.15–1.21) | |
| Hyperlipidemia | <0.0001 | ||||||
| No | 219,658 | (85.4) | 37,503 | (14.6) | 1.00 | (reference) | |
| Yes | 22,555 | (81.0) | 5285 | (19.0) | 1.30 | (1.26–1.35) | |
| MI | <0.0001 | ||||||
| No | 236,962 | (84.9) | 42,037 | (15.1) | 1.18 | (1.09–1.28) | |
| Yes | 5251 | (87.5) | 751 | (12.5) | 1.00 | (reference) | |
| Dialysis | <0.0001 | ||||||
| No | 238,140 | (84.9) | 42,500 | (15.1) | 2.76 | (2.45–3.13) | |
| Yes | 4073 | (93.4) | 288 | (6.6) | 1.00 | (reference) | |
| Type of Stroke | <0.0001 | ||||||
| Hemorrhage | 53,950 | (83.4) | 10,714 | (16.6) | 1.02 | (0.96–1.08) | |
| Ischemia | 173,573 | (85.2) | 30,155 | (14.8) | 1.21 | (1.15–1.28) | |
| Other | 14,690 | (88.5) | 1919 | (11.6) | 1.00 | (reference) | |
| LOS, days | <0.0001 | ||||||
| 1–5 | 84,534 | (87.4) | 12,172 | (12.6) | 1.00 | (reference) | |
| 6–9 | 63,969 | (85.9) | 10,499 | (14.1) | 1.06 | (1.03–1.09) | |
| 10–14 | 34,261 | (83.8) | 6605 | (16.2) | 1.16 | (1.12–1.20) | |
| 15–19 | 16,537 | (82.7) | 3465 | (17.5) | 1.22 | (1.17–1.28) | |
| ≥20 | 43,092 | (81.1) | 10,047 | (18.9) | 1.23 | (1.19–1.27) | |
| Mean ± SD | 12.8 ± 17.5 | 14.9 ± 17.0 | <0.0001 | ||||
*Logistic regression model included sociodemographics and medical conditions; Hosmer-Lemeshow goodness of fit, p-value = 0.001; c-statistic = 0.71; CI, confidence interval; LOS, length of stay; MI, myocardial infarction; OR, odds ratio
The average number of acupuncture visits in stroke patients was higher in males than in females (6.5 ± 7.8 vs. 6.4 ± 7.7, p < 0.001) (Tables 3 and 4). Stroke patients who had a low income, were white-collar employees, lived in highly urbanized areas and areas with more traditional Chinese physicians, used rehabilitation services, suffered from hemorrhagic stroke or ischemia, or had a longer hospitalization made more acupuncture visits. Patients who had more acupuncture treatment visits also had a higher expenditure on acupuncture.
Table 3.
Post-stroke visits and expenditure on acupuncture treatment within one year in stroke patients in 2000–2008 by sociodemographics
| Medical visits | Medical expenditure | ||||
|---|---|---|---|---|---|
| n | Mean ± SD | p-value | Mean ± SD | p-value | |
| Sex | 0.0155 | 0.0264 | |||
| Women | 17,225 | 6.4 ± 7.7 | 212 ± 258 | ||
| Men | 25,563 | 6.5 ± 7.8 | 219 ± 271 | ||
| Age | 0.0342 | <0.0001 | |||
| 20–29 | 369 | 6.4 ± 7.0 | 219 ± 272 | ||
| 30–39 | 1517 | 6.8 ± 7.8 | 240 ± 302 | ||
| 40–49 | 5298 | 6.7 ± 8.2 | 226 ± 279 | ||
| 50–59 | 10,054 | 6.5 ± 7.7 | 217 ± 267 | ||
| 60–69 | 12,374 | 6.4 ± 7.6 | 210 ± 254 | ||
| 70–79 | 10,424 | 6.4 ± 7.7 | 216 ± 263 | ||
| ≥80 | 2752 | 6.2 ± 7.9 | 208 ± 267 | ||
| Income | <0.0001 | <0.0001 | |||
| Very low | 12,172 | 5.0 ± 6.5 | 168 ± 220 | ||
| Low | 10,499 | 5.7 ± 7.1 | 187 ± 234 | ||
| Moderate | 6605 | 6.7 ± 7.9 | 217 ± 262 | ||
| High | 3465 | 7.6 ± 8.4 | 246 ± 276 | ||
| Very high | 10,047 | 8.5 ± 8.9 | 295 ± 321 | ||
| Occupation | <0.0001 | <0.0001 | |||
| White collar | 16,188 | 6.9 ± 8.0 | 229 ± 276 | ||
| Blue collar | 18,067 | 6.1 ± 7.4 | 203 ± 253 | ||
| Other | 8533 | 6.6 ± 7.9 | 219 ± 269 | ||
| Urbanization | <0.0001 | <0.0001 | |||
| Low | 1858 | 5.2 ± 6.8 | 173 ± 229 | ||
| Moderate | 13,509 | 6.0 ± 7.4 | 202 ± 259 | ||
| High | 27,421 | 6.8 ± 8.0 | 226 ± 270 | ||
| Density TCM | <0.0001 | <0.0001 | |||
| Low | 8117 | 5.9 ± 7.2 | 198 ± 250 | ||
| Moderate | 22,199 | 6.5 ± 7.8 | 215 ± 263 | ||
| High | 12,472 | 6.7 ± 7.9 | 230 ± 279 | ||
TCM, traditional Chinese medicine
Table 4.
Post-stroke visits and expenditure on acupuncture treatment within one year in stroke patients in 2000–2008 by medical condition
| Medical visits | Medical expenditure | ||||
|---|---|---|---|---|---|
| n | Mean ± SD | p-value | Mean ± SD | p-value | |
| Rehabilitation | <0.0001 | <0.0001 | |||
| No | 17,087 | 4.8 ± 6.3 | 157 ± 206 | ||
| Yes | 25,701 | 7.6 ± 8.4 | 256 ± 292 | ||
| Diabetes mellitus | 0.02 | 0.01 | |||
| No | 29,983 | 6.5 ± 7.8 | 218 ± 268 | ||
| Yes | 12,805 | 6.3 ± 7.7 | 211 ± 259 | ||
| Hypertension | 0.77 | 0.93 | |||
| No | 15,290 | 6.5 ± 7.8 | 216 ± 269 | ||
| Yes | 27,498 | 6.5 ± 7.7 | 216 ± 263 | ||
| Hyperlipidemia | 0.35 | 0.98 | |||
| No | 37,503 | 6.5 ± 7.8 | 216 ± 266 | ||
| Yes | 5285 | 6.4 ± 7.6 | 216 ± 259 | ||
| MI | 0.14 | 0.15 | |||
| No | 42,037 | 6.5 ± 7.8 | 216 ± 266 | ||
| Yes | 751 | 6.1 ± 7.0 | 204 ± 240 | ||
| Renal dialysis | 0.0002 | <0.0001 | |||
| No | 42,500 | 6.5 ± 7.8 | 217 ± 266 | ||
| Yes | 288 | 5.1 ± 6.1 | 161 ± 220 | ||
| Length of stay, days | <0.0001 | <0.0001 | |||
| 1–5 | 12,172 | 5.0 ± 6.5 | 168 ± 220 | ||
| 6–9 | 10,499 | 5.7 ± 7.1 | 187 ± 234 | ||
| 10–14 | 6605 | 6.7 ± 7.9 | 217 ± 262 | ||
| 15–19 | 3465 | 7.6 ± 8.4 | 246 ± 276 | ||
| ≥20 | 10,047 | 8.5 ± 8.9 | 295 ± 321 | ||
| Type of Stroke | <0.0001 | <0.0001 | |||
| Hemorrhage | 10,714 | 7.4 ± 8.5 | 253 ± 296 | ||
| Ischemia | 30,155 | 6.3 ± 7.5 | 207 ± 256 | ||
| Other | 1919 | 4.7 ± 6.3 | 154 ± 200 | ||
MI, myocardial infarction
Discussion
Our study found that the prevalence of acupuncture use among stroke patients significantly increased from 2000 to 2008 in Taiwan, and the sociodemographic characteristics were highly correlated with recent acupuncture use. In contrast to the previous report that was based on a cross-sectional sample [17], this study included all of Taiwan’s stroke patients and evaluated the patterns of acupuncture use.
The incidence of acupuncture use in the general population has been reported in the United States as 4.1 % in 2002 and 6.8 % in 2007 [6, 20]. The increasing use of acupuncture was investigated in the western countries [6, 20]. However, Chinese herbal medicine is not common in western countries. In Taiwan, Chinese herbal medicine and acupuncture were covered in the traditional Chinese medicine which is commonly used. Frequent use of acupuncture treatment was found in people with chronic diseases, such as osteoarthritis [21], cancer [22], and stroke [16]. The use of CAM is a trend, and it is not surprising that our study found that the use of acupuncture in stroke patients increased from 12 % in 2000 to 17 % in 2008. Demographic factors, such as age and sex, are associated with the patient’s choice of acupuncture [20, 23]. Compared with men, women were more likely to use acupuncture in this study. Several surveys also showed similar findings, namely, women had a higher use of TCM than men [17, 24]. Younger stroke patients were more likely to use acupuncture than older patients in this study. The association between young or middle age and acupuncture use was investigated in previous studies [17, 20, 23, 24]. The finding of better functional outcomes in younger stroke patients is not unexpected, as they had more home support and motivation [25]. A previous study suggested that young people seek more effective ways to improve their well-being and health and to relieve disease symptoms [26]. It is reasonable that younger stroke patients had a higher tendency to use acupuncture and to have a higher acupuncture expenditure than older patients in this study.
The increasing use of TCM is somewhat related to the growth of the number of TCM physicians in Taiwan [17]. A previous investigation reported that the density of TCM increased from 1.39 physicians per 10,000 residents in 1996 to 1.78 physicians per 10,000 residents in 2001 [27]. Our results also showed that the prevalence of acupuncture use in stroke patients increased with the increasing density of TCM physicians. High urbanization was associated with TCM use in a previous survey [17, 24]. Because acupuncture is a subtype of TCM, it is not surprising that we found in the present study that people who lived in an urbanized area were more likely to use acupuncture.
Economic growth is a determinant of physician supply and utilization of medical services [28]. In Taiwan, TCM has become an increasingly popular form of medicine, particularly after the implementation of the National Health Insurance in the medical care system since 1995. In this study, the frequency of acupuncture use and related insurance-paid expenditure were higher in stroke patients with a low income than in those without a low income. Co-payment is considered an important factor in the use of medical services [29]. According to the Ministry of Health and Wealth [17–19], patients with low-income status who do not need to pay a co-payment when receiving medical services may have more medical visits for acupuncture treatment than stroke patients with higher incomes.
Among the stroke patients, diabetes, hypertension, hyperlipidemia, myocardial infarction, and kidney insuffucuency were common coexisting medical conditions that were also considered comorbidities in this study [30]. Acupuncture treatment can lower blood pressure [31, 32]. Moreover, evidence-based studies have shown acupuncture’s beneficial effects in addressing physical illness in stroke patients [12–14, 33]. We found that patients with comorbidities of hypertension or hyperlipidemia were more likely to undergo acupuncture treatment. People with more chronic diseases were likely to use TCM, which was confirmed in previous surveys [17, 24].
In this study, we found that stroke patients who used acupuncture were more likely to simultaneously undergo conventional medical rehabilitation. Previous reports showed a high use of CAM in stroke survivors in many countries [16, 34]. Medical pluralism, such as adopting more than one medical system or the use of both conventional medicine and CAM for health and illness, is also common in Taiwan [35, 36].
Stroke patients with longer hospitalizations were more likely to undergo acupuncture treatment. Stroke patients who had a longer length of hospital stay may have more neurological impairment [37], so they may require more or longer rehabilitation for stroke. Our study showed that the frequency of acupuncture visits and related expenditure were higher in stroke patients after a longer length of hospital stay.
The incidence of ischemia is higher than that of other stroke subtypes [38]; however, subarachnoid hemorrhage resulted in a higher re-admission rate or mortality than ischemic stroke, and patients with a subarachnoid hemorrhage used more medical resources following stroke admission [39]. Conventional therapy with acupuncture treatment for acute ischemic stroke for four weeks has been shown to improve self-care ability and quality of life compared with sham acupuncture [40]. In this study, patients with ischemic stroke were more likely to use acupuncture than those with a subarachnoid hemorrhage. The frequency of acupuncture visits and related expenditures were higher in ischemic stroke patients.
This study had some limitations. First, we used retrospective medical claims data from health insurance claims data that lacked detailed patient information on clinical risk scores (e.g., National Institute of Health Stroke Scale score, Barthel index, and Rivermead index) and lifestyle, physical, psychiatric, and biochemical measures. We were unable to determine whether these factors were causally related to acupuncture use. Second, our study used ICD-9-CM codes claimed by physicians for the diagnosis of stroke without clarifying the severity of disease. Third, information on folk therapy was not available in the National Insurance Research Database. In addition, in-come measurement and out-come measurements of stroke patients are unavailable in this study, which are valuable indicators for efficacy of acupuncture treatment. It is also one of our study limitations. Finally, this study was based on cross-sectional analyses of acupuncture use in stroke patients. Understanding the benefit of acupuncture in stroke patients requires further cohort studies.
Conclusions
In conclusion, the application of acupuncture in stroke patients is well accepted and increasing in Taiwan. The use of acupuncture in stroke patients is associated with sociodemographic factors and clinical characteristics.
Acknowledgments
This study is based in part on data obtained from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or National Health Research Institutes.
Funding
This study was supported in part by Shuang Ho Hospital, Taipei Medical University (104TMU-SHH-23), Taiwan’s Ministry of Science and Technology (MOST105-2629-B-038-001, MOST104-2314-B-038-027-MY2, MOST103-2320-B-214-010-MY2), Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-133019).
Availability of data and material
All data supporting the study is presented in the manuscript or available upon request from the corresponding author of this manuscript (Chun-Chuan Shih) at Email: hwathai@seed.net.tw.
Authors’ contributions
All authors contributed substantially toward the design of the study, the analysis and interpretation of the data, drafting and revising the manuscript. All authors approved the final version.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
All authors have read and agreed to all the contents for publication.
Ethics approval and consent to participate
This study was approved by Taiwan’s National Health Research Institute (NHIRD-100-122) and the Institutional Review Board of E-DA Hospital, Kaohsiung, Taiwan (2014012).
Abbreviations
- CAM
Complementary and alternative medicine
- CI
Confidence interval
- ICD-9-CM
International classification of diseases, 9th revision, clinical modification
- OR
Odds ratio
- TCM
Traditional Chinese medicine
Footnotes
Dr. Chien-Chang Liao has equal contribution with the first author; Prof. Jaung-Geng Lin has equal contribution with the corresponding author.
Contributor Information
Shu-Wen Weng, Email: aaaa6712@gmail.com.
Ta-Liang Chen, Email: tlc@tmu.edu.tw.
Chun-Chieh Yeh, Email: b8202034@gmail.com.
Chien-Chang Liao, Email: jacky48863027@yahoo.com.tw.
Hsin-Long Lane, Email: imcold0404@hotmail.com.
Jaung-Geng Lin, Email: jglin@mail.cmu.edu.tw.
Chun-Chuan Shih, Phone: 886-7-615-1100, Email: hwathai@seed.net.tw.
References
- 1.Harris PE, Cooper KL, Relton C, Thomas KJ. Prevalence of complementary and alternative medicine (CAM) use by the general population: a systematic review and update. Int J Clin Pract. 2012;66:924–39. doi: 10.1111/j.1742-1241.2012.02945.x. [DOI] [PubMed] [Google Scholar]
- 2.Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1–23. [PubMed] [Google Scholar]
- 3.Hunt KJ, Coelho HF, Wider B, Perry R, Hung SK, Terry R, et al. Complementary and alternative medicine use in England: results from a national survey. Int J Clin Pract. 2010;64:1496–502. doi: 10.1111/j.1742-1241.2010.02484.x. [DOI] [PubMed] [Google Scholar]
- 4.Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine (CAM) and frequency of visits to CAM practitioners: United States, 2007. Natl Health Stat Report. 2009;18:1–14. [PubMed] [Google Scholar]
- 5.Chon TY, Lee MC. Acupuncture. Mayo Clin Proc. 2013;88:1141–6. doi: 10.1016/j.mayocp.2013.06.009. [DOI] [PubMed] [Google Scholar]
- 6.Upchurch DM, Rainisch BW. A sociobehavioral wellness model of acupuncture use in the United States, 2007. J Altern Complement Med. 2014;20:32–9. doi: 10.1089/acm.2012.0120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–292. doi: 10.1161/01.cir.0000441139.02102.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Luengo-Fernandez R, Gray AM, Rothwell PM. Costs of stroke using patient-level data: a critical review of the literature. Stroke. 2009;40:e18–23. doi: 10.1161/STROKEAHA.108.529776. [DOI] [PubMed] [Google Scholar]
- 9.Kumar S, Selim MH, Caplan LR. Medical complications after stroke. Lancet Neurol. 2010;9:105–18. doi: 10.1016/S1474-4422(09)70266-2. [DOI] [PubMed] [Google Scholar]
- 10.Tong X, Kuklina EV, Gillespie C, George MG. Medical complications among hospitalizations for ischemic stroke in the United States from 1998 to 2007. Stroke. 2010;41:980–6. doi: 10.1161/STROKEAHA.110.578674. [DOI] [PubMed] [Google Scholar]
- 11.Ingeman A, Andersen G, Hundborg HH, Svendsen ML, Johnsen SP. In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke. 2011;42:3214–8. doi: 10.1161/STROKEAHA.110.610881. [DOI] [PubMed] [Google Scholar]
- 12.Sze FK, Wong E, Or KK, Lau J, Woo J. Does acupuncture improve motor recovery after stroke? A meta-analysis of randomized controlled trials. Stroke. 2002;33:2604–19. doi: 10.1161/01.STR.0000035908.74261.C9. [DOI] [PubMed] [Google Scholar]
- 13.Wu P, Mills E, Moher D, Seely D. Acupuncture in poststroke rehabilitation: a systematic review and meta-analysis of randomized trials. Stroke. 2010;41:e171–9. doi: 10.1161/STROKEAHA.109.573576. [DOI] [PubMed] [Google Scholar]
- 14.Lee JA, Park SW, Hwang PW, Lim SM, Kook S, Choi KI, et al. Acupuncture for shoulder pain after stroke: a systematic review. J Altern Complement Med. 2012;18:818–23. doi: 10.1089/acm.2011.0457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhao XF, Du Y, Liu PG, Wang S. Acupuncture for stroke: evidence of effectiveness, safety, and cost from systematic reviews. Top Stroke Rehabil. 2012;19:226–33. doi: 10.1310/tsr1903-226. [DOI] [PubMed] [Google Scholar]
- 16.Shah SH, Engelhardt R, Ovbiagele B. Patterns of complementary and alternative medicine use among United States stroke survivors. J Neurol Sci. 2008;271:180–5. doi: 10.1016/j.jns.2008.04.014. [DOI] [PubMed] [Google Scholar]
- 17.Liao CC, Lin JG, Tsai CC, Lane HL, Su TC, Wang HH, et al. An investigation of the use of traditional chinese medicine in stroke patients in Taiwan. Evid Based Complement Alternat Med. 2012;2012:387164. doi: 10.1155/2012/387164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Liao CC, Su TC, Sung FC, Chou WH, Chen TL. Does hepatitis C virus infection increase risk for stroke? A population-based cohort study. PLoS One. 2012;7:e31527. doi: 10.1371/journal.pone.0031527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liao CC, Chang PY, Yeh CC, Hu CJ, Wu CH, Chen TL. Outcomes after surgery in patients with previous stroke. Br J Surg. 2014;101:1616–22. doi: 10.1002/bjs.9639. [DOI] [PubMed] [Google Scholar]
- 20.Burke A, Upchurch DM, Dye C, Chyu L. Acupuncture use in the United States: findings from the National Health Interview Survey. J Altern Complement Med. 2006;12:639–48. doi: 10.1089/acm.2006.12.639. [DOI] [PubMed] [Google Scholar]
- 21.Jong MC, van de Vijver L, Busch M, Fritsma J, Seldenrijk R. Integration of complementary and alternative medicine in primary care: what do patients want? Patient Educ Couns. 2012;89:417–22. doi: 10.1016/j.pec.2012.08.013. [DOI] [PubMed] [Google Scholar]
- 22.Gansler T, Kaw C, Crammer C, Smith T. A population-based study of prevalence of complementary methods use by cancer survivors: a report from the American Cancer Society’s studies of cancer survivors. Cancer. 2008;113:1048–57. doi: 10.1002/cncr.23659. [DOI] [PubMed] [Google Scholar]
- 23.Zhang Y, Lao L, Chen H, Ceballos R. Acupuncture use among American adults: what acupuncture practitioners can learn from National Health Interview Survey 2007? Evid Based Complement Alternat Med. 2012;2012:710750. doi: 10.1155/2012/710750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shih CC, Liao CC, Su YC, Tsai CC, Lin JG. Gender differences in traditional Chinese medicine use among adults in Taiwan. PLoS One. 2012;7:e32540. doi: 10.1371/journal.pone.0032540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Knoflach M, Matosevic B, Rücker M, Furtner M, Mair A, Wille G, et al. Functional recovery after ischemic stroke--a matter of age: data from the Austrian Stroke Unit Registry. Neurology. 2012;78:279–85. doi: 10.1212/WNL.0b013e31824367ab. [DOI] [PubMed] [Google Scholar]
- 26.Chang LC, Huang N, Chou YJ, Lee CH, Kao FY, Huang YT. Utilization patterns of Chinese medicine and Western medicine under the National Health Insurance Program in Taiwan, a population-based study from 1997 to 2003. BMC Health Serv Res. 2008;8:170. doi: 10.1186/1472-6963-8-170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yang CH, Huang YT, Hsueh YS. Redistributive effects of the National Health Insurance on physicians in Taiwan: a natural experiment time series study. Int J Equity Health. 2013;12:13. doi: 10.1186/1475-9276-12-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cooper RA, Getzen TE, Laud P. Economic expansion is a major determinant of physician supply and utilization. Health Serv Res. 2003;38:675–96. doi: 10.1111/1475-6773.00139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kiil A, Houlberg K. How does copayment for health care services affect demand, health and redistribution? A systematic review of the empirical evidence from 1990 to 2011. Eur J Health Econ. 2014;15:813–28. doi: 10.1007/s10198-013-0526-8. [DOI] [PubMed] [Google Scholar]
- 30.Lackland DT, Elkind MS, D’Agostino R, Sr, Dhamoon MS, Goff DC, Jr, Higashida RT, et al. Inclusion of stroke in cardiovascular risk prediction instruments: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43:1998–2027. doi: 10.1161/STR.0b013e31825bcdac. [DOI] [PubMed] [Google Scholar]
- 31.Flachskampf FA, Gallasch J, Gefeller O, Gan J, Mao J, Pfahlberg AB, et al. Randomized trial of acupuncture to lower blood pressure. Circulation. 2007;115:3121–9. doi: 10.1161/CIRCULATIONAHA.106.661140. [DOI] [PubMed] [Google Scholar]
- 32.Wang J, Xiong X, Liu W. Acupuncture for essential hypertension. Int J Cardiol. 2013;169:317–26. doi: 10.1016/j.ijcard.2013.09.001. [DOI] [PubMed] [Google Scholar]
- 33.Geeganage C, Beavan J, Ellender S, Bath PM. Interventions for dysphagia and nutritional support in acute and subacute stroke. Cochrane Database Syst Rev. 2012;10:CD000323. doi: 10.1002/14651858.CD000323.pub2. [DOI] [PubMed] [Google Scholar]
- 34.Shin YI, Yang CY, Joo MC, Lee SG, Kim JH, Lee MS. Patterns of using complementary and alternative medicine by stroke patients at two university hospitals in Korea. Evid Based Complement Alternat Med. 2008;5:231–5. doi: 10.1093/ecam/nem025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Shih SF, Lew-Ting CY, Chang HY, Kuo KN. Insurance covered and non-covered complementary and alternative medicine utilisation among adults in Taiwan. Soc Sci Med. 2008;67:1183–9. doi: 10.1016/j.socscimed.2008.06.011. [DOI] [PubMed] [Google Scholar]
- 36.Shih CC, Su YC, Liao CC, Lin JG. Patterns of medical pluralism among adults: results from the 2001 National Health Interview Survey in Taiwan. BMC Health Serv Res. 2010;10:191. doi: 10.1186/1472-6963-10-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Luengo-Fernandez R, Gray AM, Rothwell PM. Population-based study of determinants of initial secondary care costs of acute stroke in the United Kingdom. Stroke. 2006;37:2579–87. doi: 10.1161/01.STR.0000240508.28625.2c. [DOI] [PubMed] [Google Scholar]
- 38.Tsai CF, Thomas B, Sudlow CL. Epidemiology of stroke and its subtypes in Chinese vs white populations: a systematic review. Neurology. 2013;81:264–72. doi: 10.1212/WNL.0b013e31829bfde3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chang KC, Lee HC, Huang YC, Hung JW, Chiu HE, Chen JJ, et al. Cost-effectiveness analysis of stroke management under a universal health insurance system. J Neurol Sci. 2012;323:205–15. doi: 10.1016/j.jns.2012.09.018. [DOI] [PubMed] [Google Scholar]
- 40.Shen PF, Kong L, Ni LW, Guo HL, Yang S, Zhang LL, et al. Acupuncture intervention in ischemic stroke: a randomized controlled prospective study. Am J Chin Med. 2012;40:685–93. doi: 10.1142/S0192415X12500516. [DOI] [PubMed] [Google Scholar]