

Abstract
Colonic duplication cysts are rare congenital malformations that predominantly present before the age of 2 years. We report the case of a 74-year-old lady who presented with sudden onset abdominal pain. A computed tomography scan noted a calcified structure adjacent to abnormal loops of bowel. Intraoperative findings revealed an ischaemic loop of small bowel wrapped around a mass in the mesentery adjacent to the sigmoid colon. Final histology revealed a colonic duplication cyst. Colonic duplication cysts are rare entities that most commonly cause obstruction or perforation. We present the very rare case of a colonic duplication cyst causing bowel ischaemia in an elderly female.
Introduction
Gastrointestinal duplication cysts (GIDC) are rare congenital malformations that predominantly present before the age of 2 years. They are infrequently found within the colon with only a small number having been described in adults. Colonic duplication cysts most commonly cause obstruction or perforation. We present the very rare case of a colonic duplication cyst causing bowel ischaemia in an elderly female.
Case Report
A 74-year-old female, with a background history of hypertension and hypothyroidism, presented to the emergency department with a 6-h history of sudden onset generalized abdominal pain. The pain was colicky in nature, associated with nausea and refractory to analgesia. Examination revealed tenderness in the right upper quadrant and epigastrium. Blood tests were normal except for a mild neutrophilia (7.5 × 109/l) and lactate of 2.5 mmol/l. A computed tomography (CT) scan of her abdomen and pelvis was performed which showed abnormal loops of small bowel along the right side of the abdomen with mesenteric fat stranding. A partially calcified structure was noted lying medial to the loops of bowel (Figs 1 and 2). The patient proceeded to have an explorative laparotomy performed. Intraoperative findings revealed an ischaemic loop of small bowel wrapped around a mass in the mesentery adjacent to the sigmoid colon (Fig. 3). The patient underwent a partial small bowel resection with primary anastomosis and en-bloc resection of the mass with the formation of an end colostomy. The final histological revealed a 6 × 4 × 4 cm cystic colonic duplication cyst separate but adjacent to the sigmoid colon. The inner lining of the cyst revealed mucinous epithelium, with mucin contained within. The wall of the cyst was sclerotic with occasional lymphoid aggregates, smooth muscle and neurovascular bundles (Fig. 4). The patient made a good recovery and was discharged home.
Figure 1:

Axial CT scan showing a partially calcified structure adjacent to loops of small bowel.
Figure 2:

Coronal CT scan showing a partially calcified structure adjacent to loops of small bowel.
Figure 3:
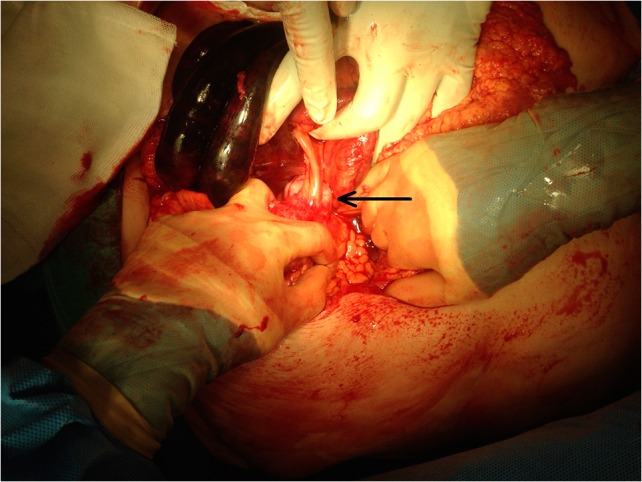
Intraoperative image black arrow pointing to intra-abdominal calcified structure. Ischaemic bowel in top left of image.
Figure 4:
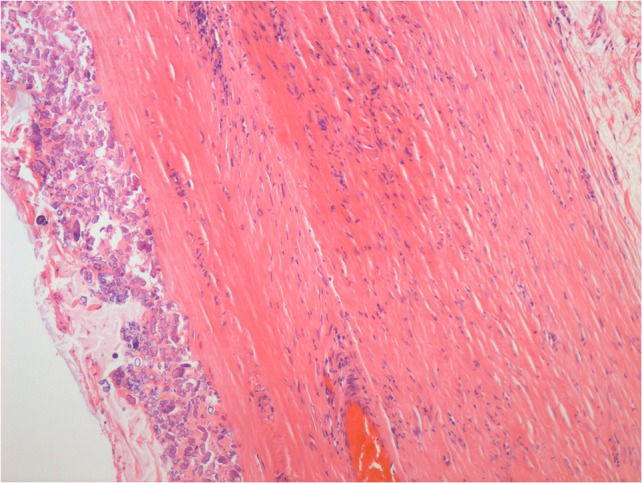
Haemolysin and eosin stain showing occasional lymphoid aggregates, smooth muscle and neurovascular bundles within the duplication cyst.
Discussion
Gastrointestinal duplication cysts are rare congenital malformations the aetiology of which is not fully understood. They are predominantly found in childhood with 67–80% presenting before the age of 2 years [1, 2]. To the best of our knowledge, our case is the latest presentation of a duplication cyst in the literature. They can occur at any point along the gastrointestinal tract from oral cavity to anus with the majority found within the abdominal cavity (75%) [1]. They most commonly involve in the ileum (60%) but can also occur in the stomach, oesophagus and colon. Duplication cysts are found adjacent to or within the GI tract and and consist of two types, cystic duplications (80%) and tubular duplications (20%) [1]. The cysts vary in size and have been reported as large as 20 × 15 cm [3].
Multiple theories have proposed the reason for the development of GIDC, recanalization, split notochord, environmental factors or presence of embryologic diverticula [4–7]. However, no one theory can explain the array of duplications.
Colonic duplication cysts are rare and account for a very small percentage of duplication cysts. The exact percentage is not fully known but one of the largest studies of 73 patients over a 22-year period found that GI duplication cysts accounted for 6.8% [1]. Colonic duplication cysts are often asymptomatic but can present with abdominal pain, vomiting or bleeding. The most common of which is pain and/or obstructive symptoms. Their presentation is often related to the complications they cause, obstruction and perforation. However, our case demonstrates small bowel ischaemia as a rare complication of duplication cyst. In this case, ischaemia resulted from a segment of small bowel becoming adherent to the cyst with resulting vascular compromise.
Colonic duplication cysts can be identified using endoscopic ultrasound, CT or rarely contrast enema. Colonoscopy may identify those that communicate with the wall of the colon. Other case reports describe a cystic gas filled structure that may be identified on plain abdominal X-ray [8]. Preoperative diagnosis is uncommon with most being diagnosed post operatively. This is due the fact that intraoperatively, it is often difficult to differentiate duplication cysts from other causes of mesenteric masses. In our case, diagnosis was only confirmed post-operatively following multidisciplinary involvement. Surgical resection is often only considered in those that are symptomatic, however, some would advocate removal due to the potential to avoid complications including the possibility of neoplastic transformation [9, 10].
In conclusion, GI duplication cysts are rare phenomena that present mainly in the paediatric population. Their presentation is reflective of the complications that they can cause. It is important to include them as a differential diagnosis of an abdominal mass.
Conflicts of interest statement
None declared.
References
- 1.Puligandla PS, Nguyen LT, St-Vil D, Flageole H, Bensoussan AL, Nguyen VH, et al. Gastrointestinal duplications. J Pediatr Surg 2003;38:740–4. [DOI] [PubMed] [Google Scholar]
- 2.Mourra N, Chafai N, Bessoud B, Reveri V, Werbrouck A, Tiret E. Colorectal duplication in adults: report of seven cases and review of the literature. J Clin Pathol 2010;63:1080–3. [DOI] [PubMed] [Google Scholar]
- 3.Sozutek A, Colak T, Dag A, Karak O. Cecal duplication cyst presenting as perforation in an adult patient. Turk J Gastroenterol 2012;23:818–9. [DOI] [PubMed] [Google Scholar]
- 4.Macpherson RI. Gastrointestinal tract duplication: clinical, pathologic, etiologic, and radiologic considerations. Radiographics 1993;13:1063–80. [DOI] [PubMed] [Google Scholar]
- 5.Bremer JL. Diverticula and duplication of intestinal tract. Arch Pathol 1944;38:133–40. [Google Scholar]
- 6.Lewis FT, Thyng FW. The regular occurrence of intestinal diverticula in the embryos of the pig, rabbit and man. Am J Anat 1907;7:505–19. [Google Scholar]
- 7.Ravitch MM. Hind gut duplication: doubling of colon and genital urinary tracts. Ann Surg 1953;137:588–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Domajnko B, Salloum RM Duplication cyst of the sigmoid colon. Gastroenterol Res Pract 2009;2009:918401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.D'Journo XB, Moutardier V, Turrini O, Guiramand J, Lelong B, Pesenti C, et al. Gastric duplication in an adult mimicking mucinous cystadenoma of the pancreas. J Clin Pathol 2004;57:1215–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blank G, Konigsrainer A, Sipos B, Ladurner R. Adenocarcinoma arising in a cystic duplication of the small bowel: report and review of the literature. World J Surg Oncol 2012;10:55. [DOI] [PMC free article] [PubMed] [Google Scholar]