

Abstract
Sickle cell disease, the most common hemoglobin disorder, affects major organ systems with symptoms of pain, anemia and a multitude of chronic conditions. For adolescents, the disease adversely affects school attendance, academic progress and social activity. To effectively study the relationship among school attendance and other factors like demographics and academic performance, studies have relied on self-reporting and school records, all of which have some bias. In this study we design and prototype a system, called SickleSAM (Sickle cell School attendance and Activity Monitoring system), for automatically monitoring school attendance and daily activity of adolescents with sickle cell disease. SickleSAM intends to remove human bias and inaccuracies. The system uses built-in GPS to collect data which will be recorded into a cloud database using Short Messaging Service technology. SickleSAM is developed by Georgia Institute of Technology in conjunction with Children's Healthcare of Atlanta (CHOA). System effectiveness is being evaluated using a trial of 10 adolescents with the disease.
Introduction
Sickle cell disease (SCD) is a genetic disorder where approximately 5% of the world's population carries trait genes for hemoglobin disorders, mainly sickle-cell disease and thalassaemia. Over 300,000 babies worldwide are born each year with these disorders[1] and in America alone there are 50,000 people, primarily of African descent, living with the disease [2]. Patients suffering from this disease experience acute pain episodes and infections in addition to other chronic conditions like anemia, cardiac, pulmonary, renal and brain complications. SCD management hence entails frequent hospitalizations and care, especially during sickle cell crisis [3].
The medical field has made great advances in reducing mortality from SCD, but much work remains to be done in improving quality of life for patients. There is evidence that increase in the number of pain episodes and their severity adversely affect school attendance [4]. There is also evidence that school absenteeism and frequent hospitalization maybe a causal factor for lower performance in school [5]. School absenteeism is also seen as a factor which negatively influences social interactions [6]. Though school attendance and activity management form a major part of academic transition, their relationship with other factors like demographic, and socio-economic variables is not adequately studied [6]. Adolescents with SCD have a high risk of school absenteeism, yet it remains a largely unexplored domain [7].
Studies which have been performed in this area are largely dependent on self reported attendance values or parent reported attendance values [6][8][9]. These studies inherently suffer from misreporting and non-compliance issues. This is of particular significance with adolescent populations. A study by Schwartz et al. requested attendance data from schools after obtaining parental compliance [7]. However this in turn limits the number of participants on the basis of the schools approached. Another study by Schatz et al. used both parental reporting and school records for obtaining the correlation between school absenteeism and academic attainment in SCD patients [10]. A correlation was found but differences in values were also seen due to differing school policies in data retrieval.
In order to address these issues we propose a solution that automatically retrieves school and other location information using a mobile phone. Mobile phones are an especially useful research device in the adolescent population. Studies reveal that about 68% of 6th_12th graders carry cell phones [11]. Many others would prefer carrying a phone but cannot afford it. Our system makes use of the built-in phone GPS to automatically track and send location information to the cloud database using Short Messaging Service (SMS). This eliminates inherent biases of self reporting, parental reporting or school policies. The system uses low cost technologies which are highly scalable in nature. Our system will be tested with patient consent and with parental assent, but does not require effort from the patients beyond carrying the phone with the application installed.
System Design And Implementation Methods
A. Use Cases
The use cases are represented using Unified Modeling Language (UML). There are four actors identified: caregivers, patients, monitoring system and the cloud database (SickleREMOTE) [8]. The caregivers can use the system to ensure that the patient activity is as expected using the system. They can also set triggers in the system which sends an alert in the event the patient missed school consecutively for a set number of days. Patients can view their own activity when desired. The SickleREMOTE system serves as a backend which collects and stores the received data and performs further analysis.
Figure 1 shows 6 use cases for these actors.
Set Location: Each caregiver has a username and password to set and change the locations of the patient's home, school and hospital. This location will be stored locally. Based on the address, location coordinates would be obtained and used for comparison purposes.
View Results: The patients and the caregivers can at any point of time view their own activity results, i.e. the amount of time spent at home, school or hospital on a given day.
Get Location from Coordinates: The monitoring
system obtains the geo-position and then assigns a location based on the previously stored coordinates of home, school and hospital.
Store Location Obtained: The location information along with the time stamp is stored on the device.
Send Data to the cloud Server: Once a day the time spent at each location is sent to SickleREMOTE via SMS. Locations are referred to by generic labels. GPS coordinates are never sent from the device.
Receive and Store Data: The system is designed to work with SickleREMOTE, which will be used to receive the data collected in the form of SMS. The data stored on the server will be made available to the respective healthcare practitioners.
Figure 1.
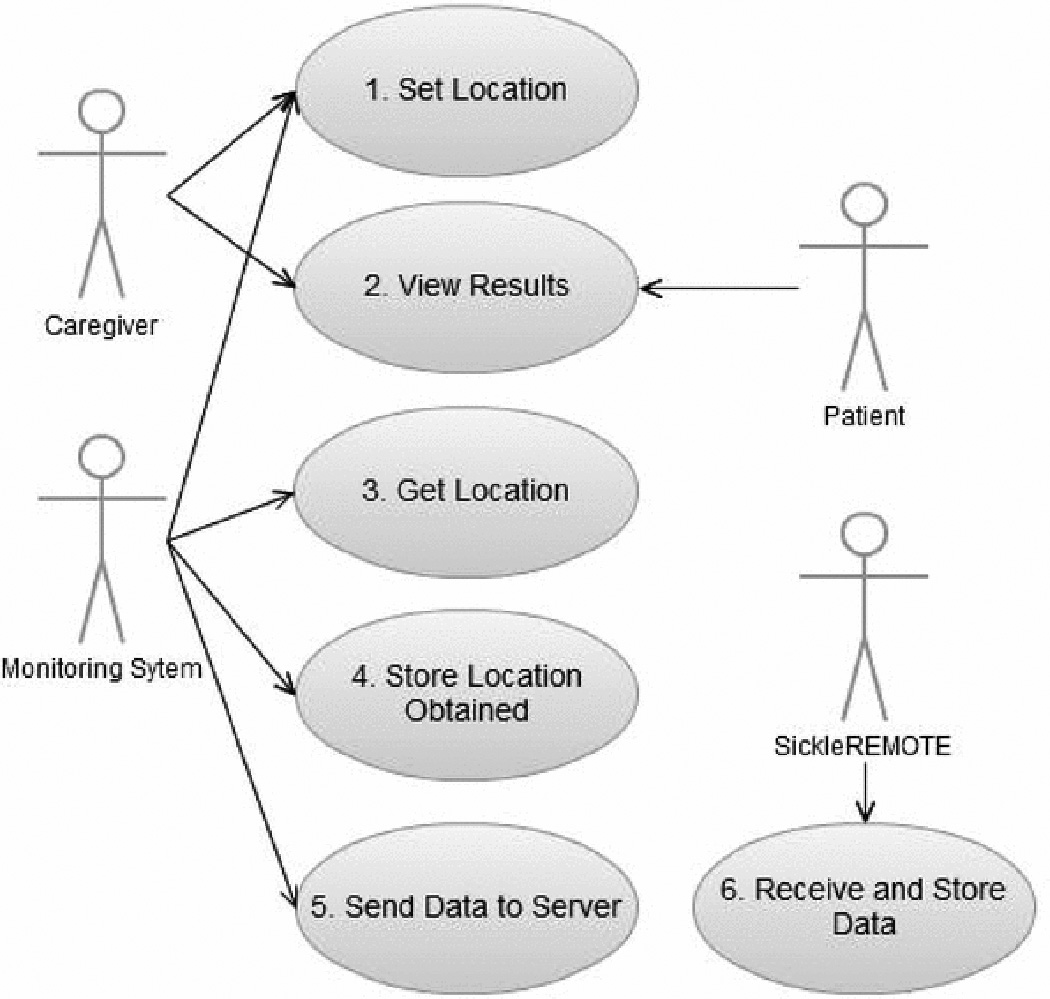
Actors and use cases in school attendance monitoring. Caregivers include parents, school teachers, healthcare personnel and caretakers. Patients are adolescents with SCD. The monitoring system refers to SickleSAM.
The highlight of SickieSAM is that the system requires no effort on the side of the users other than initial setup of mappings between GPS coordinates and location labels. The system is capable of monitoring the location and displaying the results to the user as and when needed.
B. System Implementation
SickieSAM (Figure 2) is designed for automatically monitoring the activity of patients. The activity monitoring is done by measuring the location of the patient via GPS.
Figure 2.
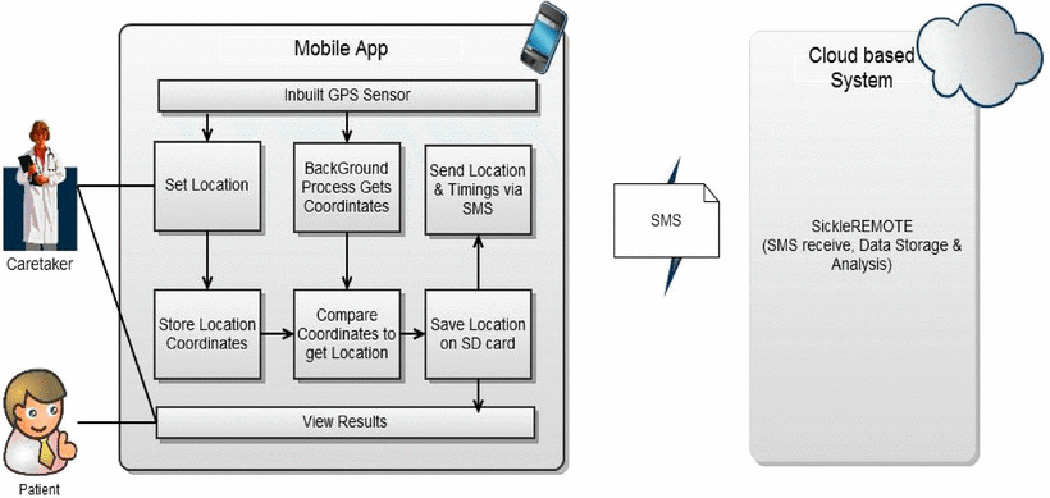
System Architecture for School Attendance Monitoring System
The major components of the system are an Android based mobile app, SMS communication and cloud database.
Mobile App: The mobile app is divided into modules which are used for location collection, setting the location and storing the location coordinates, comparing current coordinates with stored location, storing the current location with time-stamp, sending the pertinent data to the cloud database and data visualization.
Location Collection
The location is sensed using the phone's built-in GPS sensor. The geo-position obtained is then processed to obtain location information. This is done every 15 minutes if the battery level is greater than 25%, else once in 1 hr. The frequency was set such that an optimum between frequency resolution and battery life was achieved.
Setting location and storing the location coordinates
The app does not store or transmit the patient's current location coordinates. This is done in an effort to maintain the patient's privacy. The app merely transmits the information as home, school, hospital or others. In order to achieve this, the coordinates of these locations are locally stored on the mobile device. The app retrieves the location coordinates based on the address entered. This function of setting the location is restricted to the caregivers and is password protected.
Comparing current coordinates with stored location
The current gco-location is obtained from the GPS. It is compared with pre-stored values of location coordinates. If the distance between one of the pre-stored locations and the current location was found to be less than a configurable threshold than the system attributes the current location to the pre-stored location. This is written to a file on the local storage if the coordinates have changed from the previous value. The location and timestamp values are written to the local storage. In the event the GPS does not get a fix, the value is stored as no range.
Sending data to the cloud database
Relevant data, i.e. the time spent at each location is sent to the cloud database (SickleREMOTE).
SMS Communication: The time spent at each stored location is sent to the cloud using SMS one a day at 11:55 PM automatically. The time was chosen since information is sent once every 24hrs using date as the marker and it has to be done before 12 AM since the date changes after that. The format of the message is machine readable by SickleREMOTE and the data is introduced into the cloud database. The location data consists of 4 categories as shown in Table I and the timings are given in seconds. Table I shows the SMS where the patient spends 6 hrs in school, 2 hrs in hospital, 13 hrs at home and 3 hrs in other locations. The SMS means of communication was preferred over Wi-Fi due its availability in every situation.
Cloud database: The SMS message sent from the mobile app is read by SickleREMOTE, a cloud database implemented using Google App Engine and uses Google Docs for data storage. SickleREMOTE has the ability to automatically parse the SMS and store the received data in the cloud database. The use of standard interfaces i.e. Google Docs allows for a stable and user friendly system with minimal learning curve.
Data Visualizations: The system allows both the user and caregivers to locally view the results on the device in the form of a pie-chart. The day can be chosen from a drop down list. The pie-chart gives the proportion of time spent at each of the above mentioned location groups in a day. For the purposes of data visualization, the time is calculated from 12 AM till the time at which the user checks the results and the percentages appropriately plotted.
TABLE.
SMS Format and Example
| Forma t | LOC* id&1oc1=time1&1oc2=time2&1oc3=time3&loc4=time4&nosig nal=time5 |
| Exam pie | LOC*test&HOME=46800&SCH0=21600*HOSP=7200&OT HE=10800&NSIG=0 |
Additionally the caregivers can use SickleREMOTE's interface based on Google visualization packages to log on and view the results.
Results
A. System interfaces
Figure 3 shows the interface which is meant for the caregivers. The caregiver can access the “Location setting” screen in Figure 3 only when the password is correct. The view results screen displays the relative time spent in each location as a pie-chart. In Figure 4 the patient has spent 60% of his/her time at home, 25% of the time duration at school, 5% of the time at the hospital and the rest in other places.
Figure 3.
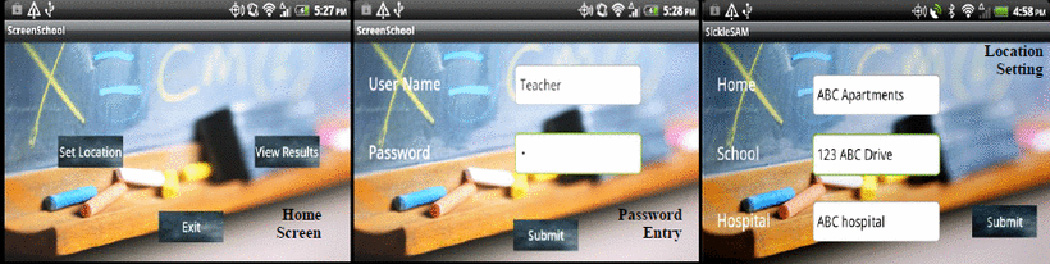
Caregiver Screens (a) Home screen to enter the location setting/view results screen (b) Authentication screens (c) Location setting screens to set the coordinates of location
Figure 4.
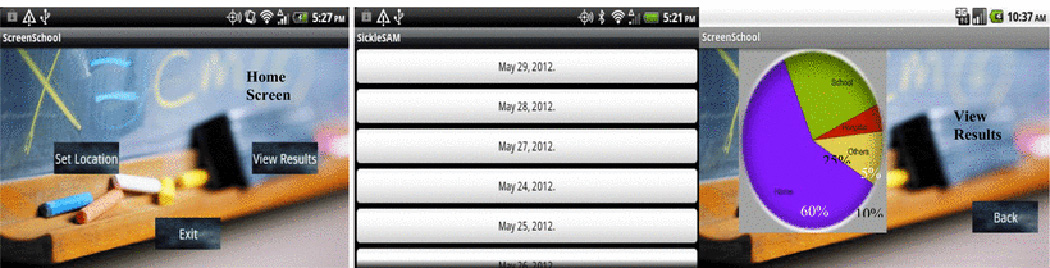
Patient Screen (a) Home screen to enter the location setting/view results screen (b) File List (c) View results screen to see the results
B. Battery Life Analysis
Figure 5 shows the comparisons in battery life with the app with location sampling every 1 min, every 5 min, every 15 min and every 1 hr. The battery life improves as the sampling interval increases. The sampling interval is adjustable according to battery life. This was chosen to arrive at balance between the sampling interval and resolution of location information.
Figure 5.
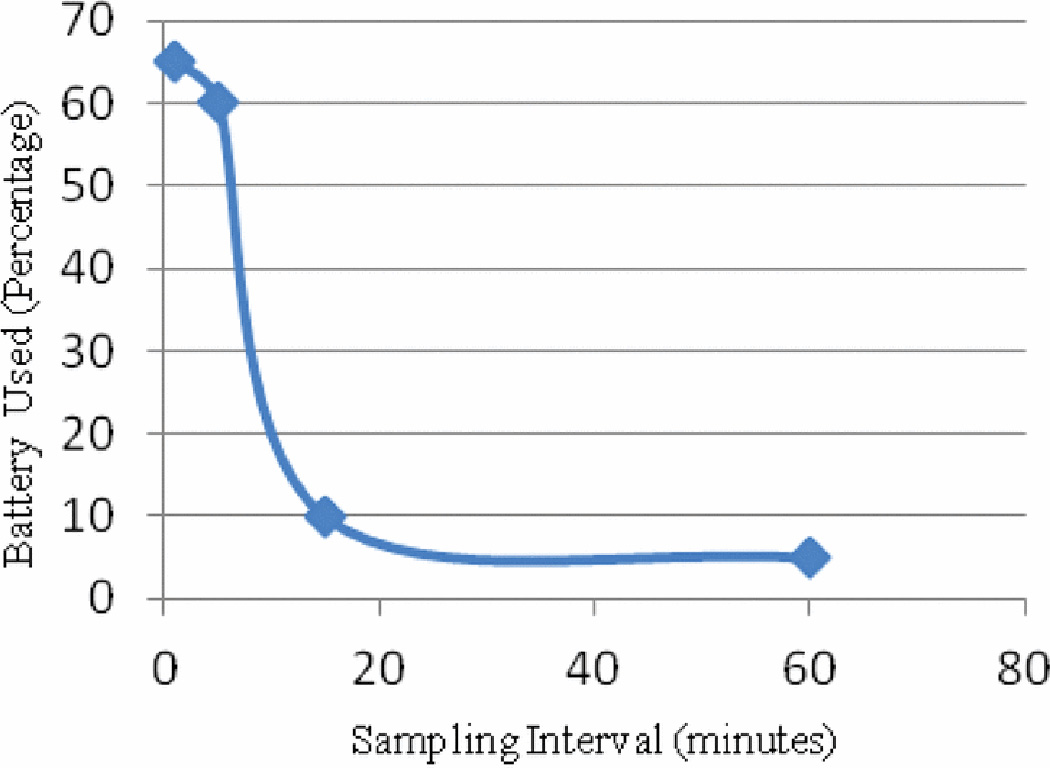
Battery comsumption in percentages with the app running for 12 hrs with each sampling frequency (carried out on HTC verizon with differeing usage patterns)
C. Test experiment design
The system will be tested on 10 children recruited from Children's Healthcarc of Atlanta (CROA) after IRB approval. Adolescents from junior high school and high school will be recruited in numbers of 2–3 per week. The total number of 10 will be will test SickieSAM and will be monitored through conventional methods of self reporting. Once the results are obtained, the data will be analyzed for significant deviations of system reported values from the self reported scores. This will serve to prove the efficacy of the proposed system.
Conclusions And Future Work
The self reporting of school attendance or the use of school records is cumbersome and bogged with inaccuracies that cast doubts on research into patient quality of life. This is of particular significance in SCD management where quantifying these parameters can improve personalized patient treatment and policies for a more disease-friendly educational system. SickieSAM automates the collection of location data required for quality of life research using a mobile phone's inbuilt GPS receiver. SickieSAM is capable of automatically collecting and storing location information to be transmitted to a cloud database once a day. The system provides feedback to patients and caregivers by presenting activity levels through the day with pie-chart visualizations. This knowledge may prove useful for self-management of their disease. SickieSAM gives caregivers novel data about children's activity levels that may advise their treatment recommendations. SickleSAM is ubiquitous and scalable through use of cloud databases and web-based Google Web Toolkit (GWT) visualizations.
We will evaluate the usefulness of the automated school monitoring service for sickle cell disease patients at Children's Hcalthcarc of Atlanta (CROA), after being approved by the institutional review board (IRB) of CROA, Emory University, and Georgia Institute of Technology. In the future, our system will be expanded to include better visualizations with multiple day results on the phones. We also plan to implement a learning algorithm that can automatically assign labels to locations to eliminate manual set-up of location labels. Other measures of activity like acceleration measurement can also be added to the existing platform. Ultimately, we would like to see data from SickieSAM integrated into patient's electronic health record.
Acknowledgments
This research has been supported by grants from The Health Systems Institute (HSI) of Georgia Tech and Emory University, National Institutes of Health (NIH) (U54CA119338, 1RC2CA148265), Georgia Cancer Coalition (Distinguished Cancer Scholar Award to Professor MDW), Georgia Research Alliance, Hewlett-Packard (HP) and Microsoft Research.
Contributor Information
Janani Venugopalan, Email: jvenugopalan3@gatech.edu, Wallace H. Coulter Department of Biomedical Engineering Department, Georgia Institute of Technology and Emory University, Atlanta, GA 30332 USA.
Clark Brown, Email: Clark.Brown@choa.org, Children's Healthcare of Atlanta and Department of Pediatrics, Emory University School of Medicine, Atlanta, GA 30322, USA.
Chihwen Cheng, Email: cwcheng83@gatech.edu, Electrical and Computer Engineering Department of Georgia Institute of Technology, Atlanta, GA 30332, USA.
Todd H. Stokes, Email: todd.stokes@bme.gatech.edu, Wallace H. Coulter Department of Biomedical Engineering Department, Georgia Institute of Technology and Emory University, Atlanta, GA 30332 USA.
May D. Wang, Email: maywang@bme.gatech.edu, Wallace H. Coulter Department of Biomedical Engineering Department, Georgia Institute of Technology and Emory University, Atlanta, GA 30332 USA.
REFERENCES
- 1.W.H. Organization. Sickle-cell disease and other haemoglobin disorders. Fact Sheet, ed. 2011
- 2.Steiner CA, Miller JL. In: Sickle Cell Disease Patients in U.S. Hospitals, 2004. H. C. a. U. P. (HCUP), editor. 2006. Dec, [PubMed] [Google Scholar]
- 3.Schnog JB, Duits AJ, Muskiet FA, ten Cate H, Rojer RA, Brandjes DP. Sickle cell disease; a general overview. Neth J Med. 2004 Nov;62:364–374. [PubMed] [Google Scholar]
- 4.Eaton ML, Have JS, Armstrong FD, Pegelow CH, Thomas M. Hospitalizations for Painful Episodes: Association with School Absenteeism and Academic Performance in Children and Adolescents with Sickle Cell Anemia. Issues in Comprehensive Pediatric Nursing. 1995;18:1–9. doi: 10.3109/01460869509080953. [DOI] [PubMed] [Google Scholar]
- 5.Berg C, Edwards DF, King A. Executive function performance on the children's kitchen task assessment with children with sickle cell disease and matched controls. Child Neuropsychology. 2011:1–17. doi: 10.1080/09297049.2011.613813. [DOI] [PubMed] [Google Scholar]
- 6.Gil KM, Carson JW, Porter LS, Ready J, Valrie C, Redding-Lallinger R, Daeschner C. Daily Stress and Mood and Their Association With Pain, Health-Care Use, and School Activity in Adolescents With Sickle Cell Disease. Journal of Pediatric Psychology. 2003 Jul 1;28:363–373. doi: 10.1093/jpepsy/jsg026. 2003. [DOI] [PubMed] [Google Scholar]
- 7.Schwartz LA, Radcliffe J, Barakat LP. Associates of school absenteeism in adolescents with sickle cell disease. Pediatr Blood Cancer. 2009 Jan;52:92–96. doi: 10.1002/pbc.21819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cheng C, Brown C, New T, Stokes TH, Dampier C, Wang MD. SickleREMOTE: A Two-Way Text Messaging System for Pediatric Sickle Cell Disease Patients; International Conference on Biomedical and Health Informatics Hong Kong, Shenzhen; 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Edwards LY, Edwards CL. Psychosocial treatments in pain management of sickle cell disease. J Natl Med Assoc. 2010 Nov;102:1084–1094. doi: 10.1016/s0027-9684(15)30737-9. [DOI] [PubMed] [Google Scholar]
- 10.Schatz J. Brief Report: Academic Attainment in Children With Sickle Cell Disease. Journal of Pediatric Psychology. 2004 Dec 1;29:627–633. doi: 10.1093/jpepsy/jsh065. 2004. [DOI] [PubMed] [Google Scholar]
- 11.Kent SJC Obringer. Cell Phones in American High Schools: A National Survey. Journal of Technology Studies. 2007;33:41–47. [Google Scholar]