

Abstract
Background
Universal goniometer (UG) is commonly used as a standard method to evaluate range of motion (ROM) as part of joint motions. It has some restrictions, such as involvement of both hands of the physician, leads to instability of hands and error. Nowadays smartphones usage has been increasing due to its easy application.
Objectives
The study was designed to compare the smartphone inclinometer-based app and UG in evaluation of ROM of elbow.
Materials and Methods
The maximum ROM of elbow in position of flexion and pronation and supination of forearm were examined in 60 healthy volunteers with UG and smartphone. Data were analyzed using SPSS (ver. 16) software and appropriate statistical tests were applied, such as paired t-test, ICC and Bland Altman curves.
Results
The results of this study showed high reliability and validity of smartphone in regarding UG with ICC > 0.95. The highest reliability for both methods was in elbow supination and the lowest was in the elbow flexion (0.84).
Conclusions
Smartphones due to ease of access and usage for the physician and the patient, may be good alternatives for UG.
Keywords: Range of Motion, Elbow Joint, Smartphone, Goniometry
1. Background
The evaluation of permanent impairment has important role for damage determination and employability (1). ‘Impairment’ according to the sixth edition of manual American medical association (AMA) is defined as any changes in normal situation or function of a body parts or organs. These changes can be evaluated by the medical criteria (2). Nowadays, for determination of joint impairments, such as elbow joint, several devices and techniques are used, such as linear measures of distances by a ruler or tape, palpation, observation estimations, photography, goniometer and digital tools (3).
Goniometer, due to low cost, portability and reliability, was used for measurement of joints range of motions (ROM) and considered as a standard method for ROM determination. One of the limitations of this technique is that the physicians should use their two hands for the examinations and in this case, keeping stable of the limbs is too difficult and can lead to some problems in reading the angles. Digital instruments are light and portable for joint movement measurement (electrical inclinometer) and its usage is similar to goniometer. The only drawback for this device is its higher cost compared to goniometer (4).
Another application was electronic inclinometer (inclinometer application on a smartphone). In this case, the phone is placed on the angle along the horizontal line shown by its application and then the angle will be evaluated (5).
The use of smartphone as a digital inclinometer has significant benefits, such as availability, appreciable cost of inclinometer applications; and easy measurement due to the commercial band which fixes the device in considered places. So during the examinations, examiners do not need both hands, and also it enables the patients to evaluate their process of healing and the efficacy of treatment by themselves at home (5).
2. Objectives
The purpose of this study was to compare two methods of universal goniometer (UG) and smartphone inclinometer application reliability, commonly used to determine elbow joint maximum ROM.
3. Materials and Methods
This study was designed to compare the use of digital tools and UG (standard and common technique) in the measuring of elbow joint maximum ROM. The sixty subjects participated in this study, with the age range of 22 - 72 years. Inclusion criteria for this study were healthy subjects without having chronic orthopedic disorders, such as old fractures, articular pain or discomfort.
3.1. Instruments
For evaluation, two techniques including UG and smartphone were used. The UG had a 360° conveyor (1° accuracy, European Product) and two 12-cm arms and a smartphone (HTC model) with Android operating system and equipped with Bubble inclinometer-based app (model 12‐1056, Fabrication Enterprises; White Plains, New York) was used in the present study (Figure 1).
Figure 1. Instruments.

A, Smartphone (HTC) with Android operating system and equipped with Bubble software; B, The plastic goniometer with 360° conveyor (1° accuracy, European Product).
3.2. Measurements
This study was double blinded and assessors and statistical analyser were not aware of the detail of study. The elbow of dominant hand was chosen for determining the ROM as a big extremity joint and the range of active movements was measured. At the elbow joint, flexion, supination and pronation of forearm movements were studied. Each movement was measured three times with two methods by each forensic medicine specialist. Then all the data were record in data sheets. Three forensic medicine specialists were trained to evaluate the ROM of elbow by the two devices including UG and smartphone and active movements of elbow joint were matched between these specialists. The UG was considered as a clinical standard technique.
All the specialists had measured all the factors of study in all patients. The data sheets were used to collect the data. The subjects were examined in three separate rooms with same facilities after a brief interview about the process of the study. The observers were blinded during the study. At first, the acromion process, lateral epicondyle of the humerus and the middle part of wrist were identified and the longitudinal axes of arm and forearm were determined. Then the elbows and forearms were located in the neutral position and UG was placed on the lateral epicondyle and stable arm was placed toward the acromion process. Also, the smartphone was set on the zero point of horizontal line along the elbow. The subject was asked to flex his/her elbow and the angle was evaluated by the moving arm of UG and placing phone along the subject arm.
For supination and pronation evaluations by smartphone, the wrist strap was used. In the sitting position, the subject arm was located along the body and the forearm was placed between these two positions and the palm was toward the body and thumb was located at 90˚ status. The opposite hand was fixed at 90˚ abduction status on a wall to prevent any lateral replacing of the body. The Smartphone was located at the zero point of vertical gravity of the hand of subjects. Then the subjects move their forearm to the entire angle of the pronation and supination positions, and the related angle was recorded.
For supination and pronation evaluations by goniometer, a pen was gripped in the subject hand to detect the axis better and the fixed arm was located on this axis. There was one hour rest for subjects after first evaluation by goniometer and the second one by smartphone.
3.3. Statistical Analysis
The data was analyzed by SPSS (ver. 16) statistical software. For evaluation of the agreement with two methods, paired t-test and intra-class correlation (ICC) was used (6). The validity and reliability of the measurements of our three examiners were examined by, testing the inter-rater reliability and for each instrument ICC test and two-way random effects were used. The results of this model were reported on ICC and 95% confidence interval (95% CI).
In the second step, paired t-test was used for comparison of mean values of these two instruments. This test can measure the concurrent validity for the instrument. Also, the correlation was used for evaluation of validity of methods. At the end of study, agreement examination of two methods was evaluated by ICC test, two-way mixed effects model or absolute agreement and bland-altman.
4. Results
The mean age was 42.25 ± 11.39 years. The number of males was 47 and females were 13. In Table 1, validity and reliability of values measured by three physicians for UG were shown. According to one-way random average measures, the results showed that the reliability of measuring between each of the three physicians and for each of the three movements was high and for the elbow joint supination was the highest.
Table 1. The Comparison of the Measurements Reliability by Goniometer and Smartphone Between Three Physicians (Inter-Rater Reliability).
| Movement Type | ICC | 95% CI |
|---|---|---|
| Goniometer | ||
| Elbow Flexion | .77 | 0.64 - 0.85 |
| Elbow pronation | .79 | 0.69 - 0.87 |
| Elbow supination | .91 | 0.86 - 0.94 |
| Smartphone | ||
| Elbow Flexion | .95 | 0.93 - 0.97 |
| Elbow pronation | .98 | 0.97 - 0.98 |
| Elbow supination | .98 | 0.97 - 0.98 |
The reliability of measured variables by the three physicians for smartphone was shown in Table 2. The reliability of measuring for all movements was very high.
Table 2. The Comparison of the Validity of Smartphone and Goniometer in Each Movement.
| Movement Type/Methods | Mean ± SD | P Value | Correlation |
|---|---|---|---|
| Elbow flexion | .07 | .73 | |
| Goniometer | 136.15 ± 2.3 | ||
| Smartphone | 136.55 ± 2.49 | ||
| Elbow pronation | .25 | .84 | |
| Goniometer | 73.54 ± 4.35 | ||
| Smartphone | 73.95 ± 5.04 | ||
| Elbow supination | .28 | .92 | |
| Goniometer | 67.15 ± 7.09 | ||
| Smartphone | 67.55 ± 7.59 |
The concurrent validity for two methods and each movement was used in Table 3. The concurrent validity in all movements of the two methods was high.
Table 3. The Comparison of the Absolute Agreement of Smartphone and Goniometer in Each Movement.
| Movement Type | ICC | 95% CI |
|---|---|---|
| Elbow flexion | .84 | 0.73 - 0.9 |
| Elbow pronation | .90 | 0.84 - 0.94 |
| Elbow supination | .96 | 0.93 - 0.97 |
The agreements of results were shown in Table 3.
According to two-way random average measures, of the absolute agreement of both smartphone and goniometer in each movement was evaluated. In addition, the Bland-Altman test for each three movements was shown in Figure 2A - C.
Figure 2. The Agreement of the Elbow.
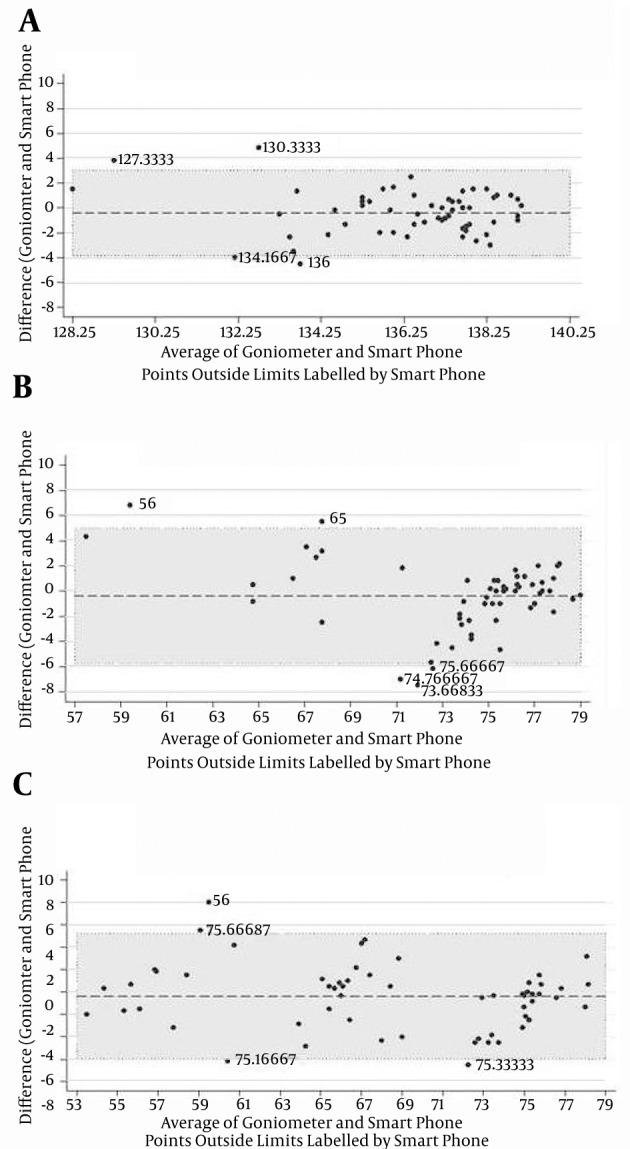
A, flexion, agreement for flexion elbow measurement. 4.60 = 6.679 (outside the limits of agreement. Mean difference -0.408. 95% limits of agreement (-3.856. 3.040). 95% limits of difference (-0.862, 0.046). Averages lies between 128.250 and 139.083. Points outside limits labled by smart phone; B, pronation, agreement for pronation elbow measurements. 5.60 = 8.3% outside limits of agreement. Mean difference: -0.408. 95% limits of agreement (-5.775. 4.959).95% limits of difference (-1.115, 0.299). Averages lie between 57.500 and 79.000; C, supination measurement by goniometer as a standard method and smartphone. Agreement for supination elbow measurements. 4.60 = 6.67% outside the limits of agreement. Mean difference: -0.400, 95% limits of agreements: (-5.989. 5.189). 95%limits of difference: (-1.136. 0.336). Averages lie between 53.500 and 78.167.
As specified, in the four cases (6.67%), the evaluated ROM of flextion and suppination and in five cases (8.33%) pronation movement are outside of the agreement range. Due to the placement of confidence interval difference in the distance of confidence interval agreement, the results measured by smartphone had significant agreement with UG.
5. Discussion
Several studies have been conducted to determine the ROM of the elbow joint (7-10). There are a few reports on the comparison of smartphone and UG in the measurement of ROM of dominant hand elbow joint as a great joint in the upper limb.
UG and digital methods are similar in the terms of education, portability and light weight. However, both hands should be used in determining the ROM of the elbow join by goniometric method. So not only it is more difficult but also some errors may happen during different measurements.
For example, the initial state of the center of rotation and the long axis of the limb was visually estimated. This can lead to the measurement errors (11, 12). The results showed that both the methods of smartphone and UG had higher agreements on all movement evaluations. The measurements taken by smartphone were similar to UG. Further, the results showed that the difference between the measurements made by the three physicians in the method of smartphone was less than UG. (Tables 1 and 2) These findings indicated high validity and reliability of smartphone for evaluation of elbow joint ROM.
Similar studies were performed in 2012 to compare the UG and inclinometer methods to evaluate the movements of the shoulder joint. The results showed that the reliability and validity of the measurements was performed by smartphone are similar to goniometer measurements (4, 5, 12-14).
In a similar study conducted by Kolber et al. (2012), the elevation of the shoulder joint at the level of scapula (Scaption) was measured. The results indicated a maximum difference of ± 11° found in the measurement of this angle by smartphone and goniometer (15); however, there was less differences in this study.
Mitchell et al. (2014) evaluated the value of active movement measurement of the shoulder joint by two methods of iPhone smartphone and goniometer on 94 female cases. Similar to our results, they reported a high reliability of smartphone in determining the ROM of shoulder (16).
The comparative studies were not limited to shoulder and elbow joints. These studies were conducted for measuring the anterior curve of the spine by the digital inclinometer (Saunders model) (17). Also, Prushansky et al. (2010) showed that there was no significant difference in the measurements of cervical movement recorded from digital instrument and ultrasound methods in healthy subjects. These measurements were taken for the movements around the sagittal and frontal axes. The results showed that the rotational movements, measured by digital instruments, had higher range (18). Yaikwawongs et al. (2009) compared the relaiblity of ROM in the knee joint in two techniques including digital compass goniometer and roentgenographic picture. ICC was calculated 0.973 (19). In other study, Ockendon et al. (2012) repeated this study and the validity of smartphone versus knee goniometer was estimated for five healthy volunteers. The intra-observer correlation was 0.982 for the smartphone (20). Cleffken et al. (2007) compared two methods of digital goniometry and electronic digital inclinometer (EDI 320) in 42 healthy subjects. They showed that active maximum flexion had lower excursions than passive maximum flexion. In addition, passive maximum flexion showed higher levels of reproducibility (19-21).
Jenny et al. (2013) compared the reliability of measuring by smartphone and standard routine method measurements of flexion range of knee joint in 10 patients with TKA. The measurements were performed six times for each method (i.e., totally 12 times). They showed that the smartphone usage after TKA was one of the most reliable ways of measuring (22).
Another goniometry for knee joint is photographic-based goniometry. Here, the photos were taken of the knee transferred from the camera to the computer and were interpreted by the software. Now, in the smartphones, there is some special software, called Dr Goniometer (Dr G) that automatically performs all the process. Ferriero et al. (2013) compared the DrG software on the smartphone with the conventional photographic-based goniometry in 35 subjects. According to results, intra-rater and inter-rater correlations were always calculated more than 0.958 in this study. The results showed that Dr G software was a reliable method to measure the ROM of knee and is much easier than the conventional method (23). Measurement of ROM of hip joint has important role for evaluation of lower limb injuries.
According to the previous studies, goniometer has high reliability in measuring of ROM of hip joint both in healthy subjects and patients with femoroacetabular impairment. Although this instrument has less reliability compared to the electromagnetic tracking system. According to the recent study, Charlton et al. (2014) evaluated the reliability of smartphone to measure the flexion, rotation, abduction and adduction movement of the hip joint. This study was conducted on 20 healthy young men. The final results showed that the smartphone had good to excellent reliability for most of the movements but it had moderate to good reliability on abduction, adduction and external rotation (6).
In this study, the lowest ICC was for elbow flexion, when using the gonoimeter (0.77). Although the ICC values of smartphone for all the movements are > 0.9, the least value was belonged to the elbow flexion. However, Blonna et al. (2012) evaluated ICC of visual estimation compared to clinical goniometry in 50 elbows. ICC for visually-based goniometry was 0.97 for both extension and flexion estimations of elbow (24).
Another study was conducted to evaluate the fifth metacarpophalangeal joints and that the results showed high value of ICC (> 0.95) (25).
In this study, the results suggest high reliability and validity of smartphone to evaluate the active movement of the elbow of dominant hand. One of the important works in legal and forensic medicine is to determine the degree of impairment. However, the results need to be replicated in future studies by more samples. It seems that easily handling of the smartphones by the patients and physicians and acceptable reliability of this device in measuring of the ROM are some advantages of this method.
5.1. Conclusion
The results of present study indicate high reliability and validity of smartphone inclinometer application in measuring the active movements of dominant hand elbow joint. In legal and forensic medicine, justice is important to determine the amount of impairment which this method could be introduced to their centers.
5.2. Limitations
In this study, healthy volunteer subjects without acute and chronic defects in upper limb joints were evaluated. But it should be noted that if there is any abnormality in the upper extremity, the studies must be repeated. For example, if there is a disruption in the shoulder joint, also some measurements in the elbow joint will be affected. In this study, we had to inform subjects about process of procedures. SO, the blindness of study could be affected.
Aging as a confounding factor can affect the results. In this study, the maximum age was 57 years. However, the subjects were recommended for training before the measurements.
Also, in this study gender effects, as a confounding factor, on the reliability of measurements was not considered. According to the cultural problems, the number of female subjects was less in this study.
5.3. Suggestions
According to the results and present study limitations, it is suggested that in the future, studies can be conducted for different age and gender groups at different days to eliminate any confounding factors and systemic error.
Footnotes
Authors’ Contribution:Study concept and design: Behnam Behnoush, Arash Okazi; acquisition of data: Arash Okazi; analysis and interpretation of data: Nasim Tavakoli, Tahmineh Mokhtari; drafting of the manuscript: Elham Bazmi, Mohammad Hossein Pourgharib Shahi; critical revision of the manuscript for important intellectual content: Behnam Behnoush, and Arash Okazi; administrative, technical, and material support: Arash Okazi; study supervision: Behnam Behnoush.
References
- 1.Ghanjal A. Comparison of permanent impairment measuring methods. Iran J Mil Med Spring. 2010;12(1):13–8. [Google Scholar]
- 2.Rondinelli RD, Genovese E, Brigham C, American Medical Associaacion . Guides to the evaluation of permanent impairment. American Medical Association; 2008. [Google Scholar]
- 3.Morrey BF, Sanchez-Sotelo J. The elbow and its disorders. Elsevier Health Sciences; 2009. [Google Scholar]
- 4.Kolber MJ, Hanney WJ. The reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer: a technical report. Int J Sports Phys Ther. 2012;7(3):306–13. [PMC free article] [PubMed] [Google Scholar]
- 5.Shin SH, Ro du H, Lee OS, Oh JH, Kim SH. Within-day reliability of shoulder range of motion measurement with a smartphone. Man Ther. 2012;17(4):298–304. doi: 10.1016/j.math.2012.02.010. [DOI] [PubMed] [Google Scholar]
- 6.Charlton PC, Mentiplay BF, Pua YH, Clark RA. Reliability and concurrent validity of a Smartphone, bubble inclinometer and motion analysis system for measurement of hip joint range of motion. J Sci Med Sport. 2015;18(3):262–7. doi: 10.1016/j.jsams.2014.04.008. [DOI] [PubMed] [Google Scholar]
- 7.Chapleau J, Canet F, Petit Y, Laflamme GY, Rouleau DM. Validity of goniometric elbow measurements: comparative study with a radiographic method. Clin Orthop Relat Res. 2011;469(11):3134–40. doi: 10.1007/s11999-011-1986-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Armstrong AD, MacDermid JC, Chinchalkar S, Stevens RS, King GJ. Reliability of range-of-motion measurement in the elbow and forearm. J Shoulder Elbow Surg. 1998;7(6):573–80. doi: 10.1016/s1058-2746(98)90003-9. [DOI] [PubMed] [Google Scholar]
- 9.Petherick M, Rheault W, Kimble S, Lechner C, Senear V. Concurrent validity and intertester reliability of universal and fluid-based goniometers for active elbow range of motion. Phys Ther. 1988;68(6):966–9. doi: 10.1093/ptj/68.6.966. [DOI] [PubMed] [Google Scholar]
- 10.van de Pol RJ, van Trijffel E, Lucas C. Inter-rater reliability for measurement of passive physiological range of motion of upper extremity joints is better if instruments are used: a systematic review. J Physiother. 2010;56(1):7–17. doi: 10.1016/s1836-9553(10)70049-7. [DOI] [PubMed] [Google Scholar]
- 11.Lea RD, Gerhardt JJ. Range-of-motion measurements. J Bone Joint Surg Am. 1995;77(5):784–98. doi: 10.2106/00004623-199505000-00017. [DOI] [PubMed] [Google Scholar]
- 12.Hanney WJ, Kolber MJ, Marshall JS. The reliability of clinical measurements designed to quantify shoulder mobility. Phys Ther Rev. 2011;16(6):413–22. doi: 10.1179/1743288x11y.0000000023. [DOI] [Google Scholar]
- 13.Kolber MJ, Vega F, Widmayer K, Cheng MS. The reliability and minimal detectable change of shoulder mobility measurements using a digital inclinometer. Physiother Theory Pract. 2011;27(2):176–84. doi: 10.3109/09593985.2010.481011. [DOI] [PubMed] [Google Scholar]
- 14.Konor MM, Morton S, Eckerson JM, Grindstaff TL. Reliability of three measures of ankle dorsiflexion range of motion. Int J Sports Phys Ther. 2012;7(3):279–87. [PMC free article] [PubMed] [Google Scholar]
- 15.Kolber MJ, Fuller C, Marshall J, Wright A, Hanney WJ. The reliability and concurrent validity of scapular plane shoulder elevation measurements using a digital inclinometer and goniometer. Physiother Theory Pract. 2012;28(2):161–8. doi: 10.3109/09593985.2011.574203. [DOI] [PubMed] [Google Scholar]
- 16.Mitchell K, Gutierrez SB, Sutton S, Morton S, Morgenthaler A. Reliability and validity of goniometric iPhone applications for the assessment of active shoulder external rotation. Physiother Theory Pract. 2014;30(7):521–5. doi: 10.3109/09593985.2014.900593. [DOI] [PubMed] [Google Scholar]
- 17.Czaprowski D, Pawlowska P, Gebicka A, Sitarski D, Kotwicki T. Intra- and interobserver repeatability of the assessment of anteroposterior curvatures of the spine using Saunders digital inclinometer. Ortop Traumatol Rehabil. 2012;14(2):145–53. doi: 10.5604/15093492.992283. [DOI] [PubMed] [Google Scholar]
- 18.Prushansky T, Deryi O, Jabarreen B. Reproducibility and validity of digital inclinometry for measuring cervical range of motion in normal subjects. Physiother Res Int. 2010;15(1):42–8. doi: 10.1002/pri.443. [DOI] [PubMed] [Google Scholar]
- 19.Yaikwawongs N, Limpaphayom N, Wilairatana V. Reliability of digital compass goniometer in knee joint range of motion measurement. J Med Assoc Thai. 2009;92(4):517–22. [PubMed] [Google Scholar]
- 20.Ockendon M, Gilbert RE. Validation of a novel smartphone accelerometer-based knee goniometer. J Knee Surg. 2012;25(4):341–5. doi: 10.1055/s-0031-1299669. [DOI] [PubMed] [Google Scholar]
- 21.Cleffken B, van Breukelen G, Brink P, van Mameren H, Olde Damink S. Digital goniometric measurement of knee joint motion. Evaluation of usefulness for research settings and clinical practice. Knee. 2007;14(5):385–9. doi: 10.1016/j.knee.2007.07.004. [DOI] [PubMed] [Google Scholar]
- 22.Jenny JY. Measurement of the knee flexion angle with a Smartphone-application is precise and accurate. J Arthroplasty. 2013;28(5):784–7. doi: 10.1016/j.arth.2012.11.013. [DOI] [PubMed] [Google Scholar]
- 23.Ferriero G, Vercelli S, Sartorio F, Munoz Lasa S, Ilieva E, Brigatti E, et al. Reliability of a smartphone-based goniometer for knee joint goniometry. Int J Rehabil Res. 2013;36(2):146–51. doi: 10.1097/MRR.0b013e32835b8269. [DOI] [PubMed] [Google Scholar]
- 24.Blonna D, Zarkadas PC, Fitzsimmons JS, O'Driscoll SW. Accuracy and inter-observer reliability of visual estimation compared to clinical goniometry of the elbow. Knee Surg Sports Traumatol Arthrosc. 2012;20(7):1378–85. doi: 10.1007/s00167-011-1720-9. [DOI] [PubMed] [Google Scholar]
- 25.de Carvalho RM, Mazzer N, Barbieri CH. Analysis of the reliability and reproducibility of goniometry compared to hand photogrammetry. Acta Ortop Bras. 2012;20(3):139–49. doi: 10.1590/S1413-78522012000300003. [DOI] [PMC free article] [PubMed] [Google Scholar]