

Abstract
College students are at high risk for engaging in heavy episodic drinking and for experiencing sexual assault. Further, drinking to cope with anxiety motives are associated with sexual assault history and drinking, and thus should be examined when targeting both sexual assault and drinking in college populations. The current study examined the effectiveness of decreasing coping with anxiety drinking motives among underage heavy episodic drinking college women (n = 264). Results indicate that the web-based combined alcohol use and sexual assault risk reduction intervention was effective at decreasing drinking to cope with anxiety motives among those with stronger drinking to cope with anxiety motives at baseline. However, the alcohol-only and sexual assault-only intervention were not. Decreases in drinking motives were associated with decreases in heavy episodic drinking. This suggests that alcohol interventions in college populations may not be effectively targeting drinking motives and this preliminary study provides evidence indicating that targeting alcohol and sexual assault together may decrease drinking to cope motives among a high risk population.
Keywords: alcohol use, drinking to cope with anxiety, sexual assault, college, heavy episodic drinking
Approximately 20% of women experience sexual assault while in college (Krebs, Lindquist, Warner, Fisher, & Martin, 2007). Engaging in heavy episodic drinking (HED) increases one's risk for experiencing a sexual assault (Parks, Hsieh, Bradizza, & Romosz, 2008) and approximately 30% of underage college women engage in HED (White, et al., 2015), defined as drinking 2 or more drinks in a period of 2 hours or less for women (NIAAA, 2004). Because of the high rates of both sexual assault and HED among college women and their high degree of comorbidity, it is imperative to decrease risk for both sexual assault and HED among college women. College women may engage in HED in order to cope with anxiety symptoms they experience following sexual assault (Cooper, 1994; Fossos et al., 2011; Smith, Smith & Grekin, 2014; Ullman & Najdowski, 2009). Engaging in HED for any reason, including drinking to cope with anxiety symptoms, is problematic on college campuses because it can increase one's risk for further victimization (Parks et al., 2008). Therefore, it is crucial to provide college women with information regarding factors that may increase sexual assault risk and provide them with tools to reduce their risk. College women who are under the age of 21 are at the highest risk for experiencing a sexual assault in college (Bureau of Justice Statistics, 2006; Humphrey & White, 2000) and rates of HED are steadily increasing for women under the age of 21 (Grucza, Norberg, & Bierut, 2009).
The current study presents findings from a randomized controlled trial designed to assess the effectiveness of a web-based intervention targeting both alcohol use and sexual assault risk among heavy episodic drinking college women who are under the age of 21. The current study extends a randomized controlled trial that found a combined web-based intervention targeting both alcohol use and sexual assault risk was most effective at reducing frequency of HED among women with more severe sexual assault histories (Author, 2015). This paper extends previous findings by examining drinking to cope with anxiety motives as a potential mechanism to understand the effect of this intervention on frequency of engaging in heavy episodic drinking.
Sexual Assault and Alcohol Use
Women with a sexual assault history are more likely to engage in alcohol use than those without such histories (Gidycz et al., 2007; Grayson & Nolen-Hoeksema, 2005; Lindgren et al., 2012). According to the self-medication hypothesis, women with sexual assault histories are likely engaging in alcohol use to cope with anxiety symptoms associated with the trauma. In fact, women with a sexual assault history do report engaging in alcohol use to reduce distress associated with the assault (Cooper, 1994; Fossos et al., 2011; Smith, Smith, & Grekin, 2014; Ullman & Nadjowski, 2009). Using this maladaptive coping strategy is particularly problematic in college populations if it leads to problematic drinking, such as engaging in HED.
HED is prospectively associated with an array of negative consequences, including sexual assault (Parks et al., 2008; Testa & Livingston, 2009). HED can increase risk for sexual assault for several reasons. First, perpetrators may target women who are engaging in HED. Second, men misperceive women's behavior while drinking as more sexual than when sober (Abbey, Zawacki, & McAulsan, 2000; George, Lehman, Cue, & Martinez, 1997). Third, consuming alcohol at high levels decreases one's ability to perceive sexual assault risk and use effective resistance strategies (Norris et al., 2006; Stoner et al., 2007; Testa, Livingston, & Collins, 2000) due to both cognitive and physiological impairments. Due to the high rates of engaging in HED on college campuses and the high risks of doing so, it is imperative to teach underage college women skills to drink in a way that decreases their risk of experiencing harm if they choose to use alcohol. That is not to say that women are to blame for their assault because of consuming alcohol. The fault of the assault lies solely with the perpetrator.
Due to this bidirectional association between sexual assault history and HED, it is imperative to target sexual assault risk and HED within the same intervention content. When targeting HED in a group at high risk for sexual assault, it is important to teach protective strategies to reduce both HED and sexual assault risk and to provide individuals with resources that aims to reduce maladaptive coping strategies such as drinking to cope with sexual assault. Targeting HED and sexual assault risk in an integrated manner may explicitly link the association between HED and sexual assault for college women. This explicit link between HED and sexual assault risk combined with teaching protective behavioral strategies (which include alternative coping strategies when sad or anxious) could reduce college women's drinking to cope, thereby reducing drinking behavior.
Brief Interventions for College Students
Brief alcohol interventions are typically used to reduce problematic alcohol use among college students. These interventions typically include personalized feedback regarding one's use compared to their peer's use to correct any misperceptions based on perceived drinking norms (e.g., Dimeff et al., 1999). Further, these alcohol interventions include didactic information regarding blood alcohol content, alcohol expectancies, alcohol-related consequences, and strategies to reduce use or to reduce alcohol-related consequences while using. These interventions are effective in reducing drinking and related harms even when presented in a web-based format (Cronce & Larimer, 2011; Dimeff, Baer, Kivlahan, & Marlatt, 1999; Miller et al., 2013; Scott-Sheldon, Carey, Elliot, Garey, & Carey, 2014). Brief interventions targeting alcohol use have been shown to effectively reduce incapacitated sexual assault experiences among college women (Clinton-Sherrod et al., 2011; Testa et al., 2010). Further, a web-based intervention targeting both alcohol use and sexual assault risk among college students has been shown to be effective at reducing frequency of heavy episodic drinking, reducing sexual assault severity, and reducing frequency of incapacitated sexual assaults (Author, 2015). However, it is not known if this brief web-based intervention is effective at reducing drinking to cope with anxiety.
Current Study
The current study extends previous findings of a randomized controlled trial on the effectiveness of a brief web-based intervention targeting alcohol use and sexual assault risk among college students. Previous findings indicated that the combined intervention was more effective at decreasing heavy episodic drinking for women with more severe adolescent/adult sexual assault histories compared to those with less severe histories (Author, 2015). It may be that women with more severe adolescent/adult sexual assault histories are at greater risk of drinking to cope with anxiety related to their sexual assault histories. Therefore, the current study extends this previous work by examining the effects of the intervention on drinking to cope with anxiety motives. Consistent with the previous findings, it was hypothesized that individuals with more severe histories of adolescent/adult sexual assault would have greater decreases in drinking to cope motives in the combined alcohol use and sexual assault risk reduction intervention condition. The combined alcohol use and sexual assault intervention will be compared to an assessment only control to determine effectiveness. Further, an alcohol use only intervention and sexual assault only intervention will be compared to an assessment only control to determine if the effect of either or both components is/are more effective than the assessment only condition. Drinking to cope with anxiety was not examined in the previous study; therefore, this manuscript extends previous findings using secondary data analysis of a randomized controlled trial.
Method
Participants
College women were recruited from introductory psychology courses at a university to participate in a study on “drinking and sexual behaviors.” Recruitment was completed by having an online posting to individuals in these courses and if they were interested, they participated in a screening survey. A total of 264 women1 (M = 18.77 years old, SD = .76 years) were eligible and enrolled in the study (39.17% of those screened). Participants were eligible if they a) were female, b) engaged in HED at least once in the past month, and c) were between the ages of 18 and 20. The majority of participants identified as White (57.60%) and the remainder identified as Asian American/Pacific Islander (20.50%), multiracial (14.10%), Black/African American (3.90%), other ethnicity/race (2.90), Native American (1.00%), and Hispanic/Latina (9.50%). The majority of participants were freshman (61.10%), not members of a sorority (65.00%), living on campus or in a sorority house (71.90%), and were not in serious relationship (71.50%). Descriptive information pertaining to study variables can be found in Table 1.
Table 1.
Descriptives for and Correlations between Study Variables.
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | -- | |||||||||||
| 2.Dummy Code 1: Comparing Assessment group to Alcohol-Only group | −.071 | -- | ||||||||||
| 3. Dummy Code 2: Comparing Assessment group to Sexual Assault-Only group | .067 | −.248* | -- | |||||||||
| 4. Dummy Code 3: Comparing Assessment group to Combined group | −.019 | −.248* | −.245* | -- | ||||||||
| 5. History of Child Abuse | .023 | −.022 | −.045 | .035 | -- | |||||||
| 6. Severity of Adult Sexual Assault | .123† | .041 | .068 | −.053 | .094 | -- | ||||||
| 7. Sorority | −.123† | −.003 | −.019 | .004 | −.149* | .075 | -- | |||||
| 8. Readiness to Change | .114 | .047 | .085 | −.023 | .041 | .269*** | .099 | -- | ||||
| 9. Baseline Drinking to Cope | .067 | −.004 | .040 | −.066 | .120† | .212** | −.070 | .147*. | -- | |||
| 10. Follow-up Drinking to Cope | −.044 | .055 | −.129† | −.084 | .084 | .120 | .004 | .053 | .586*** | -- | ||
| 11. Baseline Heavy Episodic Drinking | −.077 | .001 | −.010 | −.071 | .007 | .162* | .370*** | .139* | .047 | .053 | -- | |
| 12.Follow-up Heavy Episodic Drinking | −.054 | −.049 | −.046 | −.003 | −.186* | .218** | .265*** | .120* | .133* | .209** | .527*** | -- |
| Mean (SD) or % in category (N) | 18.77 (.76) | 40.5% (N=107) assessment, 20.1% alcohol-only (N=53) | 19.7% (52) Sexual Assault-Only | 19.7% (N=52) Combined | 13.1% (N=86) | 5.44 (10.71) | 37.8% (N=100) | .264 (.61) | 2.01 (.75) | 1.80 (.79) | 2.49 (1.39) | 1.92 (1.43) |
Notes: N=264
p<.l
p<.05
p<01
p<.001.
Measures
Adolescent/Adult Sexual Assault
Adolescent/adult sexual assault history was assessed using the Sexual Experiences Survey (Koss et al., 2007). Participants were asked about coerced sexual experiences after their 14th birthday using behaviorally specific questions including experiences perpetrated by verbal coercion, incapacitation, threats of physical force, and physical force were assessed. Adolescent/adult sexual assault experiences included sexual contact, sexual coercion, attempted penetration, and completed penetration. Participants indicated the number of times that a tactic or multiple tactics were used up to 3 times. Adolescent/adult sexual assault severity was determined using a 63-point scale (Davis et al., 2014) for each time point with high scores indicating more severe sexual assault experiences and scores of 0 indicating no adolescent/adult sexual assault. This scoring procedure takes into account both frequency of experiences (0 to 3) and severity of experiences. A severity score was calculated by multiplying each experience type by the frequency and then summing all of the experiences for a total of up to 63 points.
Membership in a Sorority
Participants were asked whether they were currently a member of a sorority. Answer choices were either 0 (“No”) or 1 (“Yes”).
Readiness to Change
Participants were asked 12 questions about their thoughts on changing their alcohol use habits from the “Readiness to Change” questionnaire for brief interventions (Rollnick, Gold, & Hall, 1992; e.g. I don't think I drink too much). Answer choices ranged from 1 (strongly disagree) to 5 (strongly agree). A mean score of these 12 items was used to measure individuals’ readiness to change, with higher scores indicating less readiness to change (α = .69; current sample).
Heavy Episodic Drinking
Frequency of HED was assessed at two time points: baseline and at 3-month follow-up using the following question: “How often did you have 4 or more drinks containing any kind of alcohol within a 2 hour period.” For the baseline assessment participants answered this question based on the past month and for the follow-up period they answered the question based on the past 3 months. Answer choices ranged from 0 times in the past month to five to six times a week or more (range: 0-7; skew: .570, −.856).
Drinking to Cope Motives
Participants were asked questions from the Drinking Motives Questionnaire – Revised Short-Form (Grant et al., 2007) with answer choices ranging on a 5-point scale (1 = almost never or never, 2 = some of the time, 3 = half of the time, 4 = most of the time, and 5 = almost always or always). Participants answered this questionnaire at baseline and at the 3-month follow-up. At baseline, participants were asked how often in the past 12 months they drank based on 5 items from the coping-anxiety subscale (e.g. “to reduce my anxiety” and “to forget my worries”; α = .83; current sample). At follow-up, participants were asked the same questions but during the time frame of the past 3 months (α = .84; current sample).
Procedure and Intervention Conditions
A total of 264 were eligible to participate in the study and prior to completing the baseline assessment/screening survey, participants were randomized to receive either a full assessment (n = 211) or minimal assessment control condition (n = 53) stratified by sexual assault history. After completing the baseline assessment, those who completed the full assessment were then randomly assigned stratified based on sexual assault history to a full assessment only control condition (n = 54), an alcohol-only intervention condition (n = 53), a sexual assault risk reduction-only intervention condition (n = 52), or a combined alcohol and sexual assault risk reduction condition (n = 52). The alcohol-only intervention was an already developed and tested personalized feedback intervention (Neighbors et al., 2010) which included content from web-based version of BASICS (Dimeff, Baer, Kivlahan, Marlatt, 1999) which provides a personalized summary of drinking and related consequences, moderation education, alcohol expectancies, and other didactic information using the spirit of motivational interviewing. The sexual assault risk reduction-only program included personalized feedback components regarding campus- and state-specific definitions and prevalence of sexual assault, risk factors for sexual assault, and education regarding risk perception, resistance strategies, barriers to resistance, and resources if assaulted. The combined alcohol and sexual assault risk reduction program included integrated content from both interventions (for more details regarding interventions, see Author, 2015). Participants received extra course credit for participating in the baseline assessment. Participants then completed a follow-up survey 3 months later and received an e-gift card of $25 for their participation.
Three dummy coded variables were created to compare these four groups of participants. For all three dummy codes, the assessment only group was the reference group. The first dummy code compared the assessment group to the alcohol only intervention group, and the second dummy code compared the assessment only group to the sexual assault risk reduction-only condition. Finally, the third dummy code compared the assessment only group to the combined alcohol and sexual assault risk reduction groups.
Data Analytic Plan
In order to test the hypothesized effects, a path model was estimated using MPlus Version 7 using the Model Indirect command (Muthen & Muthen, 1998-2011). Mplus used the Full Information Maximum Likelihood (FIML) estimator, which produces less bias compared to other techniques (e.g. list wise deletion, pairwise deletion, and mean imputation; Enders, 2001). Emerging adult age, membership in a sorority (dichotomous), readiness to change, and earlier levels of the outcomes (i.e. heavy episodic drinking and drinking to cope) were used as covariates. Main effects of dummy codes 1, 2, and 3, as well as childhood sexual abuse and history of adolescent/adult sexual assault were entered as predictors of follow-up drinking to cope. Additionally, interactions between the dummy codes and each of the other predictors and covariates were initially entered into the model. In general, non-significant interactions were trimmed. However, if a significant interaction (p<.05) between one dummy code and a predictor or covariate was detected, the interactions between the other two dummy codes and that construct were also retained in the final study model. Significant interactions were probed using simple slope analyses (Aiken & West, 1991). This approach involved examining the simple slopes one standard deviation above the mean, at the mean, and one standard deviation below the mean on the moderator. Finally, drinking to cope at follow-up was used to predict follow-up heavy episodic drinking. The indirect effects of the interventions on heavy episodic drinking through drinking to cope was also be examined.
Covariates to be examined in the model will include age, sorority membership, readiness to change, and sexual assault history. Readiness to change (Grossbard et al., 2016) and sexual assault history (Author, 2015) have both been shown to affect changes in drinking from brief alcohol interventions with college students. Further, there are differences of perceived normative drinking patterns in sorority houses compared to other locations (Lewis et al., 2011) and perceived norms were a central piece of the alcohol intervention. Finally, age is important to consider in the analyses because sexual assault and drinking patterns differ based on age (Bureau of Justice Statistics, 2006; Grucza, Norberg, & Bierut, 2009; Humphrey & White, 2000).
Power Analyses
Power analyses were conducted using G*Power 3 (Faul, Erdfelder, Lang & Buchner, 2007) in order to determine the effect sizes that the analyses will be able to detect. Given that power changes based on the size of the sample and the number of predictors, power analyses for the proposed study were conducted for the 10 main covariate and predictor effects, as well interactions between the three dummy codes and each of the seven other covariates/predictors (i.e. 21 interactions potentially tested) on drinking to cope. Given the sample size (n=264), there is sufficient power (>.99) to detect medium effects (f2 =.15) and large effects (f2 =.35). The power to detect small effects was .25, which is below the minimum power value of .80, suggested by Cohen (1988). Additionally, power analyses for the effect of drinking to cope on heavy episodic drinking indicate that there is sufficient power (>.99) to detect medium effects (f2=.15) and large effects (f2 =.35), but power to detect small effects was .63, which is again below the minimum power value of .80, suggested by Cohen. Therefore, we conclude that we have power to detect medium and large effects.
Results
Correlations
Tables 1 provides the zero-order Pearson (between two continuous variables), Tetrachoric (two dichotomous variables), and Biserial (dichotomous and continuous variables) correlations for constructs included in the final study model. In terms of relations between covariates and predictors, those who experienced greater severity of adult sexual assault were likely to endorse more frequent drinking to cope and heavy episodic drinking at baseline. Additionally, those in a sorority were less likely to report a history of child abuse. Finally, those who reported greater readiness to change were less likely to have experienced more severe adult sexual assault.
In terms of relations between covariates/predictors and outcomes, experiencing child sexual abuse was significantly associated with less heavy episodic drinking at follow-up. Those who experienced greater severity of adult sexual assault were more likely to endorse more heavy episodic drinking at follow-up. Those in a sorority were more likely to engage in heavy episodic drinking at baseline and follow-up. Additionally, those who reported greater readiness to change drank less to cope at baseline, and engaged in less heavy episodic drinking at baseline and follow-up. Finally, baseline drinking to cope was associated with follow-up drinking to cope as well as with follow-up heavy episodic drinking, and baseline heavy episodic drinking was associated with follow-up heavy episodic drinking.
Establishing Temporal Precedence between Drinking to Cope and Heavy Episodic Drinking
Because we were interested in examining predictors of drinking to cope, and in turn the impact of drinking to cope on heavy episodic drinking (and have these constructs measured at two time points), it was important to first test whether prospective and/or bidirectional relations existed among these variables. Therefore, a cross-lagged model examining baseline drinking to cope and heavy episodic drinking as predictors of follow-up drinking to cope and heavy episodic drinking was estimated. Main effects of the dummy codes comparing treatment conditions, child sexual abuse history, sexual assault severity, and young adult age were entered as covariates in this model. Interestingly, over and above baseline heavy episodic drinking, baseline drinking to cope prospectively increased risk for heavy episodic drinking at follow-up (b=.21, p<.05). However, over and above baseline drinking to cope, heavy episodic drinking was not associated with drinking to cope at follow-up (b=.014, NS). Therefore, we conclude that drinking to cope has prospective effects on heavy episodic drinking, but no support was found for the reverse. In the mediational models that follow, we estimate predictors of follow-up drinking to cope (controlling for baseline drinking to cope and heavy episodic drinking), and in turn its effect on follow-up heavy episodic drinking.
Final Study Model
Goodness of fit was determined by comparing results from the model with standards for acceptability (i.e. Hu & Bentler, 1999). The final model (described below) showed good fit to the data: RMSEA=.024, CFI=.991, SRMR=.016. Table 2 provides the standardized model results, and results are depicted in Figure 1.
Table 2.
Results of Path Model (N=264) Predicting Drinking to Cope and HED.
| Predictor | Follow up Drinking to Cope | Follow up Heavy Episodic Drinking | ||||
|---|---|---|---|---|---|---|
| B | SE | R squared (.1=small, .3=medium, .5=large) | B | SE | R squared (.1=small, .3=medium, .5=large) | |
| Dummy Code 1: Comparing Assessment group to Alcohol-Only group | .064 | .066 | .004 | −.073 | .058 | .005 |
| Dummy Code 2: Comparing Assessment group to Sexual Assault-Only group | .171 | .100 | .029 | −.005 | .064 | .000 |
| Dummy Code 3: Comparing Assessment group to Combined group | −.025 | .061 | .006 | −.045 | .064 | .002 |
| Baseline Heavy Episodic Drinking | .018 | .071 | .000 | .517*** | .059 | .267 |
| Baseline Drinking to Cope | .749*** | .109 | .561 | -- | -- | |
| Severity of Adult Sexual Assault | .029 | .066 | .001 | -- | -- | |
| Age | −.051 | .058 | .003 | -- | -- | |
| Sorority | .041 | .070 | .002 | -- | -- | |
| Readiness to Change | −.037 | .050 | .001 | -- | -- | |
| History of Child Abuse | .020 | .091 | .000 | -- | -- | |
| D1 × Baseline Cope | −.014 | .085 | .000 | -- | -- | |
| D2 × Baseline Cope | −.136 | .097 | .018 | -- | -- | |
| D3 × Baseline Cope | −.190* | .087 | .036 | -- | -- | |
| Follow Up Drinking to Cope | -- | -- | -- | .184** | .053 | .039 |
Note.
p<.05
p<.01
p<.001. B =Standardized regression coefficient. SE= Standard error.
Figure 1.
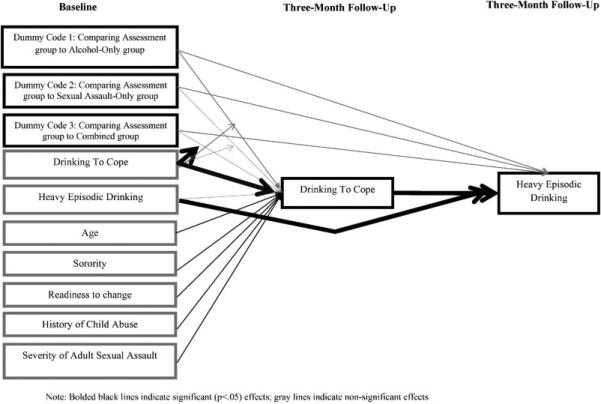
Final Study Model.
Effects on Drinking to Cope
In terms of intervention effects, support was found for the interaction between the combined intervention (i.e. dummy code 3) and baseline drinking to cope. Specifically, the combined intervention reduced drinking to cope at follow-up for those with higher (b=−.155, p<.05) levels of drinking to cope motives at baseline. However, this intervention had no effect on drinking to cope at follow-up for those at the mean (b=−.025, NS) or below the mean on drinking to cope at baseline (b=.105, NS). This interaction is depicted in Figure 2. We found no effects of the alcohol only or sexual assault only interventions, adult sexual assault severity, or childhood sexual abuse.
Figure 2.

Interaction between Condition (Combined versus Assessment) and Baseline Drinking to Cope.
In terms of covariate main effects, more drinking to cope with anxiety at baseline was associated with increased drinking to cope with anxiety at follow-up. No other main effects of covariates were found.
Effects on Follow-up Heavy Episodic Drinking
There were no effects of any of the dummy codes (i.e. interventions) on HED at follow-up. However, more baseline HED was associated with more follow-up HED. Additionally, individuals who endorsed more drinking to cope motives were at greater risk for HED at the follow-up.
Mediational Findings: Predicting Heavy Episodic Drinking
We next examined whether drinking to cope mediated the effect of the interventions on heavy episodic drinking. Because no effects of the alcohol only or the sexual assault only interventions on drinking to cope were found, we did not examine drinking to cope as a mediator of this intervention effect on heavy episodic drinking.
In examining drinking to cope as a mediator of the effect of the combined intervention, however, significant moderated mediation was found. Specifically, follow-up drinking to cope mediated the effect of the combined intervention on heavy episodic drinking for those above the mean on baseline drinking to cope [95% CI: −.250- −.010]. This mediated effect was non-significant at the mean on baseline drinking to cope [95% CI: −0.100-.066] or for those below the mean on baseline drinking to cope [95% CI: −.054-.195].
Discussion
It is essential to provide college women with tools to reduce problematic alcohol use in college due to their increased risk of engaging in HED (Grucza et al., 2009). Further, engaging in HED increases sexual assault risk and even though the assault is solely in the fault of the perpetrator, it is essential to give college women the knowledge and tools available to reduce their risk even if they cannot truly prevent an assault from occurring. The current study provides an extension of previous findings and found support that a web-based combined alcohol use and sexual assault risk reduction program is effective at reducing drinking to cope motives among a subset of underage college women who engage in HED. The current study found that both the combined intervention, but not each intervention separately, was effective at reducing drinking to cope motives for those who had stronger drinking to cope motives at baseline. Stronger drinking to cope motives at follow-up was associated with more frequent heavy episodic drinking. Together, these findings are compelling because they present an intervention that is effective at reducing drinking to cope motives and frequency of HED among college women who are at highest risk: those who endorse strong drinking to cope motives.
Drinking to cope motives decreased among college women with stronger drinking to cope motives for drinking in the combined intervention.
It is likely that the combined intervention was most effective at reducing drinking to cope because it provided personalized feedback on protective strategies to reduce both HED and sexual assault risk and provided individuals with resources that aims to reduce maladaptive coping strategies such as drinking to cope with sexual assault. Further, the combined intervention was only effective for individuals with high baseline drinking to cope motives. This might be because the information was more applicable to this population and it is possible that if one engaged in drinking to cope more when receiving the intervention, their drinking motives might be more likely to change than those who do not engage in drinking to cope motives at all. Perhaps receiving feedback regarding explicit connections between alcohol use and sexual assault risk somehow disentangled the use of alcohol to cope with anxiety and may have encouraged individuals to engage in overall safer behaviors. It is surprising that there was no effect of the alcohol-only condition on drinking to cope motives at follow-up, suggesting that the interventions targeting both alcohol use and sexual assault risk in this high risk population are perhaps needed in college settings. Future studies should replicate this finding and examine potential mechanisms to explain this finding including assessing potential drinking to cope with sex motives. Additionally, future research should consider incorporating drinking motive-specific feedback which has promising preliminary findings (Blevins & Stephens, 2016) into combined alcohol and sexual assault risk interventions for college women who engage in heavy episodic drinking.
Decreases in drinking to cope with anxiety motives were associated with decreases in frequency of HED among a subset of college women. This suggests that for some, drinking to cope with anxiety motives are a mechanism of change of this combined intervention and it may be possible to strengthen the efficacy of this intervention by more directly targeting drinking motives through drinking motive-specific feedback (Blevins & Stephens, 2016).
Limitations and Future Directions
Several important limitations should be considered when interpreting the results from this study. First, this study examined individuals who engaged in heavy episodic drinking and who were between the ages of 18 and 21. Although this is a high risk group, the findings may not extend to other populations and future research should examine the effects of this intervention in other populations. Second, participants in the combined intervention received twice the amount of the information as in the other intervention conditions, thus the differential effects may be due to dosage. However, despite the dosage effects, it remained clear that among individuals with stronger drinking to cope motives, the interventions with the sexual assault risk reduction content were effective at reducing drinking to cope motives. Third, we had sufficient power to detect medium and large effects, and most of the covariates and predictors exerted small effects. Therefore, it is possible that if we had had a larger sample, we would have been able to detect more significant effects. Fourth, only two time points were assessed in the study. Future research should include more time points to more carefully examine mediation effects. Finally, individuals that participated in this study could be different than individuals who were not interested in participating. It may be that those who were interested were already interested in changing their drinking or their motives for drinking. Therefore, if all college students were mandated to complete this intervention the effects may not remain the same. However, future research should examine potential effects of this intervention on a general population of college students (i.e., incoming college students) to determine if this intervention could be effective as a preventative methods for the general population of college students.
Conclusion
The current study extends previous research by suggesting that a combined alcohol use and sexual assault risk reduction program is not only effective at reducing heavy episodic drinking among women with more severe sexual assault histories (Author, 2015), it also is effective at decreasing drinking to cope with anxiety motives among those who had high motives at baseline. These findings are incredibly promising due to the ease of dissemination of such an intervention. Because it is a web-based intervention, it could be easily disseminated to college campuses and to individuals prior to entering college if future research continues to support its efficacy.
Highlights.
Drinking to cope with anxiety is associated with heavy episodic drinking (HED).
Current study examined alcohol and/or sexual assault (SA) interventions.
Combined alcohol and SA intervention decreased drinking to cope for those with stronger baseline drinking to cope motives.
Drinking to cope mediated effects of combined intervention on HED for those with stronger baseline drinking to cope motives.
Targeting alcohol use alone may not effectively reduce drinking to cope motives.
Acknowledgements
Role of Funding Sources
Data collection and manuscript preparation was supported by grants from the National Institute for Alcohol and Abuse and Alcoholism (F31AA020134 PI: A. K. Gilmore), from the Alcohol and Drug Abuse Institute at the University of Washington, and from the National Institute of Mental Health (T32 MH18869, PIs: Dean G. Kilpatrick, PhD, & Carla Kmett Danielson, PhD). NIAAA and NIMH had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributors
AK Gilmore designed the study, collected the data, conducted preliminary analyses, and drafted the manuscript. KE Bountress analyzed the data and wrote the results and methods section. Both authors contributed to and have approved the final manuscript.
Conflict of Interest
All authors declare that they have no conflicts of interest.
Of these 264 women, 207 were retained at follow-up. Because there were no differences between the 207 retained and the 57 not retained on outcomes of interest at baseline (i.e. drinking to cope and heavy episodic drinking), all 264 women were included in analyses.
References
- Abbey A, Zawacki T, McAuslan P. Alcohol's effects on sexual perception. Journal of Studies on Alcohol. 2000;61:688–697. doi: 10.15288/jsa.2000.61.688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aiken L, West S. Multiple Regression: Testing and Interpreting Interactions. Sage; Newbury Park, CA: 1991. [Google Scholar]
- Blevins CE, Stephens RS. The impact of motives-related feedback on drinking to cope among college students. Addictive Behaviors. 2016;58:68–73. doi: 10.1016/j.addbeh.2016.02.024. doi: http://dx.doi.org/10.1016/j.addbeh.2016.02.024. [DOI] [PubMed] [Google Scholar]
- Bureau of Justice Statistics . Criminal victimization in the United States, 2005 statistical tables: National Crime Victimization Survey. US Department of Justice (NCJ215244); 2006. http://www.bjs.gov/content/pub/pdf/cvus05.pdf. [Google Scholar]
- Clinton-Sherrod M, Morgan-Lopez AA, Brown JM, McMillen BA, Cowells A. Incapacitated sexual violence involving alcohol among college women: The impact of a brief drinking intervention. Violence Against Women. 2011;17:135–154. doi: 10.1177/1077801210394272. http://dx.doi.org/10.1177/1077801210394272. [DOI] [PubMed] [Google Scholar]
- Cooper ML. Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychological Assessment. 1994;6:117–128. [Google Scholar]
- Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college student drinking. Alcohol Research: Current Reviews. 2011;34:210–221. [PMC free article] [PubMed] [Google Scholar]
- Davis KC, Gilmore AK, Stappenbeck CA, Balsan MJ, George WH, Norris J. How to score the sexual experiences survey? A comparison of nine methods. Journal of Violence. 2014;4:445–461. doi: 10.1037/a0037494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dimeff LA, Baer JS, Kivlahan DR, Marlatt G. Brief alcohol screening and intervention for college students (BASICS): A harm reduction approach. Guilford Press; New York, NY, US: 1999. [Google Scholar]
- Enders C. The performance of the Full Information Maximum Likelihood Estimator in Multiple Regression Models with Missing Data. Educational and Psychological Measurement. 2001;61:713–740. [Google Scholar]
- Fossos N, Kaysen D, Neighbors C, Lindgren KP, Hove MC. Coping motives as a mediator of the relationship between sexual coercion and problem drinking in college students. Addictive Behaviors. 2011;36:1001–1007. doi: 10.1016/j.addbeh.2011.06.001. doi: 10.1016/j.addbeh.2011.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George WH, Lehman GL, Cue KL, Martinez LJ. Postdrinking sexual inferences: evidence for linear rather than curvilinear dosage effects. Journal of Applied Social Psychology. 1997;27:629–648. [Google Scholar]
- Gidycz CA, Loh C, Lobo T, Rich C, Lynn SJ, Pashdag J. Reciprocal relationships among alcohol use, risk perception, and sexual victimization: A prospective analysis. Journal of American College Health. 2007;56:5–14. doi: 10.3200/JACH.56.1.5-14. [DOI] [PubMed] [Google Scholar]
- Grant VV, Stewart SH, O'Connor RM, Blackwell E, Conrod PJ. Psychometric evaluation of the five-factor Modified Drinking Motives Questionnaire—Revised in undergraduates. Addictive Behaviors. 2007;32:2611–2632. doi: 10.1016/j.addbeh.2007.07.004. [DOI] [PubMed] [Google Scholar]
- Grayson CE, Nolen-Hoeksema S. Motives to drink as mediators between childhood sexual assault and alcohol problems in adult women. Journal of Traumatic Stress. 2005;18:137–145. doi: 10.1002/jts.20021. [DOI] [PubMed] [Google Scholar]
- Grossbard JR, Mastroleo NR, Geisner IM, Atkins D, Ray AE, Kilmer JR, Mallet K, Larimer ME, Turrisi R. Drinking norms, readiness to change, and gender as moderators of a combined alcohol intervention for first-year college students. Addictive Behaviors. 2016;52:75–82. doi: 10.1016/j.addbeh.2015.07.028. doi:10.1016/j.addbeh.2015.07.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grucza RA, Norberg KE, Bierut LJ. Binge drinking among youths and young adults in the United States: 1979-2006. Journal of the American Academy of Child & Adolescent Psychiatry. 2009;48:692–702. doi: 10.1097/CHI.0b013e3181a2b32f. http://dx.doi.org/10.1097/CHI.0b013e3181a2b32f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler A. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6:1–55. [Google Scholar]
- Humphrey JA, White JW. Women's vulnerability to sexual assault from adolescence to young adulthood. Journal of Adolescent Health. 2000;27:419–424. doi: 10.1016/s1054-139x(00)00168-3. http://dx.doi.org/10.1016/S1054-139X(00)00168-3. [DOI] [PubMed] [Google Scholar]
- Koss MP, Abbey A, Campbell R, Cook S, Norris J, Testa M, White J. Revising the SES: a collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly. 2007;31:357–370. http://dx.doi.org/10.1111/j.1471-6402.2007.00385.x. [Google Scholar]
- Krebs CP, Lindquist CH, Warner TD, Fisher BS, Martin SL. The campus sexual assault (CSA) study. Department of Justice (DOJ 221153); 2007. https://www.ncjrs.gov/pdffiles1/nij/grants/221153.pdf. [Google Scholar]
- Lewis MA, Litt DM, Blayney JA, Lostutter TW, Granato H, Kilmer JR, Lee CM. They drink how much and where? Normative perceptions by drinking contexts and their association to college students’ alcohol consumption. Journal of Studies on Alcohol and Drugs. 2011;72 doi: 10.15288/jsad.2011.72.844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindgren KP, Neighbors C, Blayney JA, Mullins PM, Kaysen D. Do drinking motives mediate the association between sexual assault and problem drinking? Addictive Behaviors. 2012;37:323–326. doi: 10.1016/j.addbeh.2011.10.009. doi: 10.1016/j.addbeh.2011.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller MB, Leffingwell T, Claborn K, Meier E, Walters S, Neighbors C. Personalized feedback interventions for college alcohol misuse: An update of Walters & Neighbors (2005). Psychology of Addictive Behaviors. 2013;27:909–920. doi: 10.1037/a0031174. doi:10.1037/a0031174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user's guide (sixth edition) Muthén & Muthén; Los Angeles, CA: 1998-2011. [Google Scholar]
- NIAAA (National Institute of Alcohol Abuse and Alcoholism) NIAAA council approves definition of binge drinking. Vol. 3. NIAAA Newsletter 2004; 2004. p. 3. [Google Scholar]
- Norris J, George WH, Stoner SA, Masters N, Zawacki T, Davis K. Women's responses to sexual aggression: the effects of childhood trauma, alcohol, and prior relationship. Experimental and Clinical Psychopharmacology. 2006;14:402–411. doi: 10.1037/1064-1297.14.3.402. http://dx.doi.org/10.1037/1064-1297.14.3.402. [DOI] [PubMed] [Google Scholar]
- Parks KA, Hsieh YP, Bradizza CM, Romosz AM. Factors influencing the temporal relationship between alcohol consumption and experiences with aggression among college women. Psychology of Addictive Behaviors. 2008;22:210–218. doi: 10.1037/0893-164X.22.2.210. http://dx.doi.org/10.1037/0893-164X.22.22.210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rollnick S, Heather N, Gold R, Hall W. Development of a short 'readiness to change' questionnaire for use in brief, opportunistic interventions among excessive drinkers. British Journal Of Addiction. 1992;87:743–754. doi: 10.1111/j.1360-0443.1992.tb02720.x. Doi: 10.1111/j.1360-0443.1992.tb02720.x. [DOI] [PubMed] [Google Scholar]
- Scott-Sheldon LA, Carey KB, Elliott JC, Garey L, Carey MP. Efficacy of alcohol interventions for first-year college students: a meta-analytic review of randomized controlled trials. Journal of Consulting and Clinical Psychology. 2014;82:177–188. doi: 10.1037/a0035192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith KZ, Smith PH, Grekin ER. Childhood sexual abuse, distress, and alcohol-related problems: Moderation by drinking to cope. Psychology of Addictive Behaviors. 2014;28:532–537. doi: 10.1037/a0035381. doi:10.1037/a0035381. [DOI] [PubMed] [Google Scholar]
- Stoner SA, Norris J, George WH, Davis K, Masters N, Hessler DM. Effects of alcohol intoxication and victimization history on women's sexual assault resistance intentions: the role of secondary cognitive appraisals. Psychology of Women Quarterly. 2007;31:344–356. http://dx.doi.org/10.1111/j.1471-6402.2007.00384.x. [Google Scholar]
- Testa M, Hoffman JH, Livingston JA, Turrisi R. Preventing college women's sexual victimization through parent based intervention: a randomized controlled trial. Prevention Science. 2010;11:308–318. doi: 10.1007/s11121-010-0168-3. http://dx.doi.org/10.1007/s11121-010-0168-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Livingston JA. Alcohol consumption and women's vulnerability to sexual victimization: can reducing women's drinking prevent rape? Substance Use & Misuse. 2009;44:1349–1376. doi: 10.1080/10826080902961468. http://dx.doi.org/10.1080/10826080902961468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Testa M, Livingston JA, Collins R. The role of women's alcohol consumption in evaluation of vulnerability to sexual aggression. Experimental and Clinical Psychopharmacology. 2000;8:185–191. doi: 10.1037//1064-1297.8.2.185. [DOI] [PubMed] [Google Scholar]
- Ullman SE, Najdowski CJ. Revictimization as a moderator of psychosocial risk factors for problem drinking in female sexual assault survivors. Journal of Studies on Alcohol and Drugs. 2009;70:41–49. doi: 10.15288/jsad.2009.70.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White A, Castle IP, Chen CM, Shirley M, Roach D, Hingson R. Converging patterns of alcohol use and related outcomes among females and males in the United States, 2002 to 2012. Alcoholism: Clinical and Experimental Research. 2015;39:1712–1726. doi: 10.1111/acer.12815. doi: 10.1111/acer.12815. [DOI] [PubMed] [Google Scholar]