

Abstract
The most frequent cause of functional posterior crossbite is the reduction in width of the maxillary dental arch. This posterior crossbite is associated with anterior crowding which is presented as an infrapositioned canine or a palatally positioned lateral incisor on one side; this leads to an upper midline shift toward the crowded side. The present case report shows the management of posterior crossbite with functional shift and upper midline shift simultaneously without adverse side effects. In this case, rapid maxillary expansion along with fixed appliance is used to correct posterior crossbite with the upper dental midline shift using reciprocal action of elastic transseptal fibers.
Key words: Functional shift, midline shift, posterior crossbite
Introduction
Posterior crossbite is defined as any abnormal buccolingual relation between opposing molars, premolars or both in centric occlusion. The etiology of posterior crossbite can include any combination of dental, skeletal, and neuromuscular functional components.[1,2,3] The most frequent cause of functional posterior crossbite is the reduction in width of the maxillary dental arch. This results in anterior crowding, presented as an infrapositioned canine, which leads to an upper midline shift toward the crowded side.[4] Reduced maxillary width can be corrected with maxillary expansion treatment. The treatment mechanics for the correction of midline discrepancies must be also planned to achieve the desired results without adverse side effects. The following case shows how a upper midline shift with posterior crossbite can be corrected with rapid maxillary expansion (RME) followed guidance of the highly placed canine into occlusion.
Case Report
A 13-year-old male patient reported to the orthodontic clinic with the chief complaint of irregularly placed teeth in upper and lower jaw. His medical and dental history was noncontributory. On examination, he had an asymmetrical face with straight profile and competent lips. Chin was deviated toward the right side in occlusion due to the functional shift of mandible. There were no other associated signs or symptoms of temporomandibular disorder. Molar relation was Class I on both sides on Class III skeletal bases with average mandibular growth pattern. Posterior crossbite extended from canine to the first molar on the right side and on first molars on the left side. Maxillary and mandibular anterior crowding with deep bite was present with highly placed maxillary right canine and lingually placed lower left lateral incisor. There was upper midline shifted toward left side by 3 mm and lower midline shifted toward right side by 3 mm [Figure 1].
Figure 1.
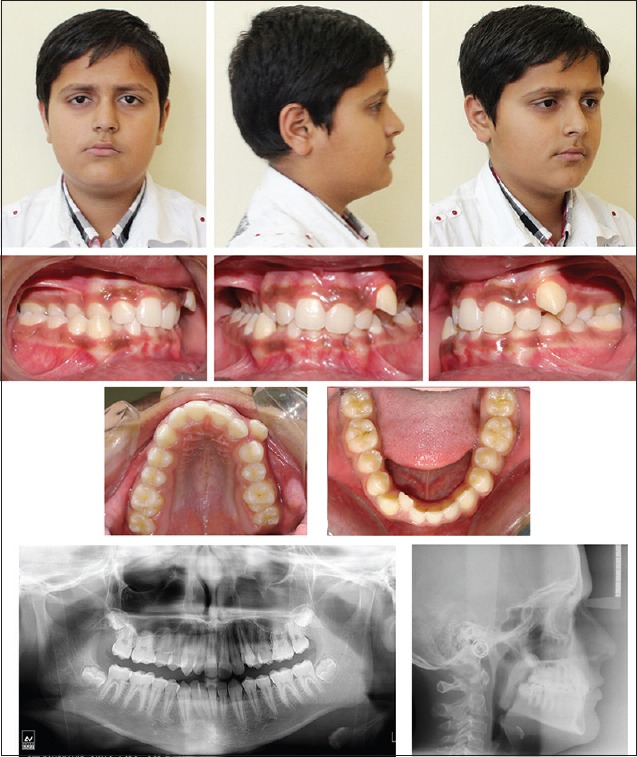
Pretreatment extraoral and intraoral photographs and radiographs showing crowding in upper, lower arch with highly placed upper left canine and posterior crossbite and deep bite
Cephalometric analysis revealed that he had cervical vertebrae maturation index stage 3, Class skeletal bases due to retrognathic maxilla with retruded maxillary and mandibular anteriors. Panoramic radiograph showed full complement of teeth in maxillary and mandibular arch except third molar in all quadrant, which was in almost crown completion stage [Figure 1].
Model analysis showed that patient had overjet of 1 mm and overbite of 6 mm with arch length deficiency of 7 mm in maxillary arch and 5 mm in mandibular arch. Asymmetric maxillary arch with a constriction of 4 mm in the molar and 2.5 mm in the premolar region on the right side was found on occlusogram. The initial contact point of upper and lower tooth of patient during closing of jaw [Figure 2].
Figure 2.

Pretreatment photograph showing initial contact point of upper and lower tooth
Treatment plan
Treatment objective was to correct the posterior crossbite to prevent the functional shift of the mandible toward the right side, to coincide upper and lower midlines and to relieve the maxillary and mandibular anterior crowding and achieve normal overjet and overbite with good intercuspation. The patient was planned to be treated with RME device to expand the maxillary arch and simultaneously correct the upper midline shift with fixed mechanotherapy.
Treatment progress
RME was done using a banded type Hyrax appliance which was palatally soldered bilaterally to the bands of first molar and first premolar on either side with a 19-Gauge stainless steel wire. The molar bands were welded with molar tubes on either side. The removable lower posterior bite plane was given from mesial of the first premolar to the second molar bilaterally on lower arch to jump the bite and Hyrax appliance framework was cemented to the maxillary arch. The screw was turned twice each day, once in the morning and once in the evening, for a total of 0.5 mm activation per day. The activation was carried out until desired 5 mm expansion was achieved in 10 days.
Immediately after the expansion, 0.022 slot McLaughlin, Bennett, Trevisi preadjusted brackets were bonded on the maxillary arch to correct the maxillary anterior crowding [Figure 3]. The central incisor started moving towards the midline diastema reciprocally by the residual forces of the elastic transseptal fibers and also using power chain. Tight figure of eight was given from maxillary right central incisor to right upper canine to prevent reciprocal movement of the right central incisor. The expansion appliance was left for 4 months aid to in retention. After the removal of the Hyrax appliance, the removable maxillary anterior bite plane was used for bite opening as well as retention. The mandibular arch was bonded, and 0.014″ NiTi is placed for alignment. Once the alignment was completed, coordinated 0.017″ × 0.025″ SS wire was placed in upper and lower arch. Pre- and post-model symmetry were compared with ortho grid. Posttreatment records show proclination of upper and lower anteriors for compensation of arch length-tooth size discrepancy [Figure 4]. Lateral cephalometric superimposition shows a significant amount of growth changes in maxilla, mandible, and soft tissue of face [Figure 5].
Figure 3.

Midtreatment intraoral photographs showing Banded Hyrax with 0.016 SS wire in upper arch and lower posterior bite plate
Figure 4.
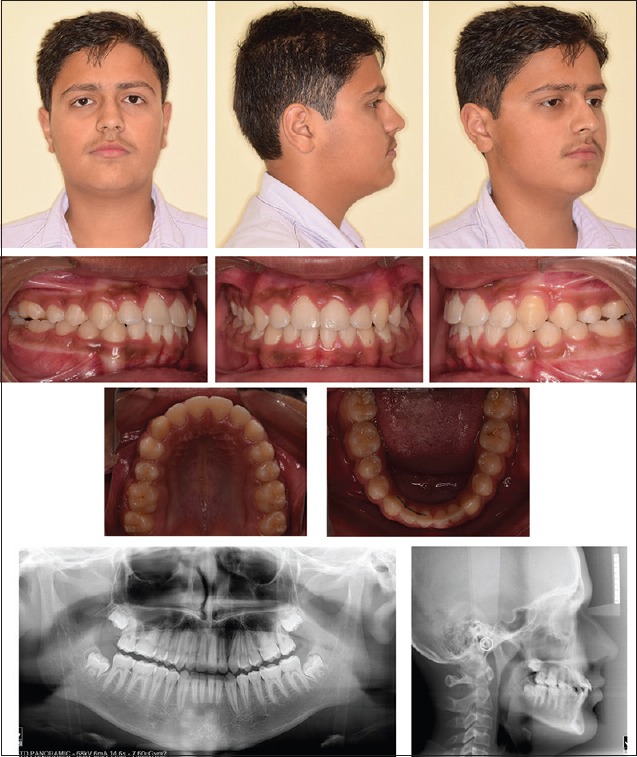
Posttreatment extraoral and intraoral photographs and radiographs showing highly placed upper left canine in occlusion with normal overjet, overbite, and proclination of upper and lower incisor for compensation of arch length-tooth size discrepancy
Figure 5.
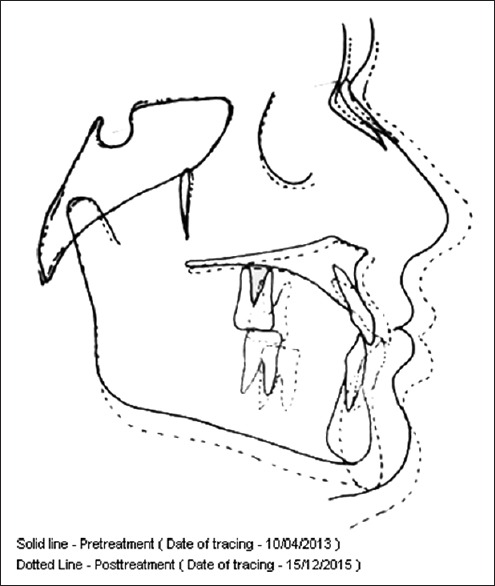
Pretreatment (solid line) and posttreatment (dashed line) lateral cephalogram superimposition
Discussion
Functional posterior crossbite treatment success depends on the expansion of the maxillary arch, removal of occlusal interferences, and elimination of the functional shift. RME is recommended in the patients in early permanent dentition stage of development, as it gives greater degree of skeletal expansion and produce less dental tipping than slow maxillary expansion protocols. In a patient of posterior crossbite, with the use of RME, the midpalatal suture opens, the alveolar processes bend, and move laterally with the maxilla; and the central incisors are separated, creating a midline diastema. During the retention period of expansion, the central incisors start moving toward the midline diastema reciprocally by the residual forces of the elastic transseptal fibers, but it would not correct the midline shift because the central incisors move reciprocally toward each other.[5,6,7] In this case, we used RME along with fixed appliance to correct the upper dental midline shift, without active forces using tight figure of eight from right molar to right central incisor. Due to this after expansion and right central incisor does not move reciprocally and left central incisor move mesially, so upper midline correction occurs. These treatment protocols correct the constriction of the maxilla and provide enough space to correct the anterior crowding with midline shift.
Conclusion
This case report shows that simultaneous approach to correct the midline shift and anterior crowding with posterior crossbite caused by the constriction of the maxilla were treated successfully with RME along with fixed appliance.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Moyers R. Handbook of Orthodontics. 2nd ed. Chicago: Year Book Medical Publishers, Inc.; 1966. pp. 332–41. [Google Scholar]
- 2.Allen D, Rebellato J, Sheats R, Ceron AM. Skeletal and dental contributions to posterior crossbites. Angle Orthod. 2003;73:515–24. doi: 10.1043/0003-3219(2003)073<0515:SADCTP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Kennedy DB, Osepchook M. Unilateral posterior crossbite with mandibular shift: A review. J Can Dent Assoc. 2005;71:569–73. [PubMed] [Google Scholar]
- 4.Alcan T, Ceylanoglu C. Upper midline correction in conjunction with rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2006;130:671–5. doi: 10.1016/j.ajodo.2005.02.020. [DOI] [PubMed] [Google Scholar]
- 5.Haas AJ. Palatal expansion: Just the beginning of dentofacial orthopedics. Am J Orthod. 1970;57:219–55. doi: 10.1016/0002-9416(70)90241-1. [DOI] [PubMed] [Google Scholar]
- 6.Binder RE. Correction of posterior crossbites: Diagnosis and treatment. Pediatr Dent. 2004;26:266–72. [PubMed] [Google Scholar]
- 7.Starnbach H, Cleall J. The effects of splitting the mid palatal suture on the surrounding structures. Am J Orthod. 1964;50:923–4. [Google Scholar]