

Abstract
Introduction:
Workers represent half the world's population and are major contributors to economic and social development. Tobacco consumption in construction site workers has been considered a big challenge.
Objectives:
(1) To assess the prevalence of nicotine dependence among tobacco users. (2) To study the correlates of nicotine dependence among the construction site workers.
Methodology:
A cross sectional study was conducted using a predesigned and pretested structured proforma. The study was conducted among all construction site workers aged 18yrs and above in campus of Hamdard Institute of Medical Sciences and Research and associated HAH centenary hospital, New Delhi. Karl Fagerstrom Nicotine Dependence Questionnaire was used to assess dependence on nicotine.
Results:
The mean age of construction site workers was 32.04±11.6 years. Among the workers, majority (91%) were tobacco user. Among the users, 60% found it difficult to refrain from smoking/chewing in places where use of tobacco is not allowed (e.g. hospitals, government offices, cinemas, Libraries etc). 55% of the users smoked or chewed tobacco during the first hours after waking than during the rest of the day. On multivariate analysis, the factors which were found to be significantly associated with nicotine dependence were lower income group (OR 2.57, CI:1.66-3.99), smokeless tobacco use (OR 2.36, CI:1.30-4.27) and lower education (OR = 2.86 (95% CI 1.97-4.16) for illiterate).
Discussion:
The prevalence of tobacco use (91%) among construction workers is very high compared to that in the general population. Recognition of construction sites as work places and proper implementation of law is needed.
Keywords: Construction workers, nicotine dependence, tobacco use
INTRODUCTION
Nicotine dependence has been recognized as one of the major public health problems facing the human race, both in the developing and the developed countries. It kills one person prematurely every six smokers globally and one in two long-term smokers – largely in low- and middle-income countries.[1,2] India is equally affected by this single most preventable cause of death and disease, major risk factor for a noncommunicable disease that are slowly threatening the human life. It has been estimated by WHO that by 2020, tobacco use will be responsible for 13.3% of all deaths in India.[3] Smoking alone accounts for 7 lakh deaths annually and 8–9 lakh deaths annually due to all forms of tobacco use/exposure, many of the deaths occur below 70 years of age (>50%).[4] Every form of tobacco such as cigarette, cigar, pipe tobacco, snuff, and chewing tobacco contain 4000 chemicals along with nicotine which is highly addictive and is readily absorbed into the bloodstream.[5] It was found that physiological and behavioral processes that determine tobacco dependence are similar to those that determine heroin and cocaine addiction.[6]
Nicotine dependence is a sign of the compulsive use of nicotine-containing tobacco, physiologic tolerance (needing to use increase amounts of nicotine to achieve desired effects), nicotine withdrawal upon discontinuation (symptoms: craving, irritability, anger, anxiety, depression, increased appetite) and continued use despite a lot of problems due to its use.[7] The presence of nicotine sustains tobacco dependence, which in turn causes devastating health problems, mainly including heart diseases, lung disease, cancers and reproductive disorders, and increased susceptibility to a variety of infectious diseases. Tobacco harms almost every organ of the body.[8] The pharmacological reasons for nicotine use are an enhancement of mood, either directly or through relief of withdrawal symptoms and augmentation of mental or physical functions. The release of dopamine, glutamate, gamma-aminobutyric acid is particularly important in the development of nicotine dependence, and corticotropin releasing factor may play a key role in withdrawal.[8] It is now referred to as tobacco use disorder as it harbors enormous adverse consequences for health, and is recognized as a disease in the WHO's (International Classification of Diseases-10) and the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders-IV.[9]
Evidence shows that around 50% of those who start smoking in the adolescent years continue to smoke for 15–20 years.[10] Hence, early recognition and treatment of nicotine dependence are pertinent for quitting policy and to avert diseases and deaths due to tobacco use. It was also found that highly addicted smokers make serious attempts to quit but are able to stop only for a few hours.[11]
Workers represent half the world's population and are major contributors to economic and social development.[12] So, the effect of nicotine dependence on workers’ health causes significant economic costs due to increased absenteeism and reduced productivity.[13]
In India, nearly two-thirds of the contribution to the net domestic product is by the unorganized sector.[14] Notable differences in smoking rates are seen across occupational groups, and significantly higher tobacco consumption rates have been found among construction site workers.[15] As it is a crucial point of health promotion in the workplace tobacco consumption. In order to address these inequalities, new or alternative approaches should be considered as innovations beyond current practices.
The current study was designed to identify correlates of nicotine dependence among construction site workers in India. They are highly susceptible to nicotine dependence for several reasons. Poor living conditions, migration along with the lack of basic amenities to maintain the standard of living, making them prone to dependence.[16] Employment-driven migration is mainly from the “relatively less developed” states to large metropolises and other large cities, wherein the migrants get absorbed in low-paid jobs in the unorganized sectors. We hypothesized that dependence would be associated with socio-demographic factors. Findings will stimulate and inform the creation, implementation, and evaluation of targeted dependence prevention and cessation strategies and programs. Although, several nationwide prevalence studies such as the National Family Health Survey and Global Adult Tobacco Survey report the proportion of the population using tobacco products in India nicotine dependence rates are not well documented.[17,18] Moreover, a study on correlates of nicotine dependence among construction site workers of Delhi were found scarce.
Objectives
To assess the prevalence of nicotine dependence among tobacco users
To study the correlates of nicotine dependence among the construction site workers.
METHODOLOGY
Study design and study population
A cross-sectional study was conducted among all construction site workers aged 18 years and above in campus of, Hamdard Institute of Medical Sciences and Research and associated HAH Centenary Hospital, New Delhi. The study included 250 workers for a period of 6 months (September 2014 to March 2015) but only 172 male workers agreed to participate in the study.
Inclusion criteria
All adult males and females (aged above 18 years) in a payroll of the construction site and willing to participate will be included.
Exclusion criteria
Workers who are mentally challenged if any would consent and unable to respond to the questions (due to hearing problem or any other reason) will be excluded.
Ethical clearance permission
Necessary permission to conduct the study was obtained from the concerned authority of the construction site. Written informed consent was obtained from the respondents after explaining the nature and objectives of the study in their local language. The study was approved by the Institutional Review Board and Institutional Ethical Committee.
Tool and methodology
Data was collected by face to face Interview method using WHO adopted pretested semi-structured questionnaire[19] having questions pertaining to sociodemographic details and tobacco use. Nicotine dependence was assessed using Fagerstrom test, a validated questionnaire for nicotine dependence.[20,21]
The semi-structured questionnaire included three sections as followings:
Demographic profile: It contained information on age, sex, education, occupation, income of the family
Socioeconomic status was determined using the modified Kuppuswamy scale[22]
Tobacco behavior: It contained information about knowledge, attitude, practice of workers regarding tobacco (number of cigarettes smoked per day, age at smoking initiation, duration of the smoking, smokeless tobacco products used (yes/no), ever tried to quit smoking (yes/no) and the number of times tried to quit in last 1 year, etc.). Fagerstrom test for nicotine dependence (FTND) is considered to be a self-reporting tool which conceptualizes dependence through physiological and behavioral symptoms.[21]
Nicotine dependence questionnaire
It contained following six standard questions of the FTND. (i) How soon after you wake up do you smoke your first cigarette? (Within 5 min [3 points], within 6–30 min [2 points], within 31–60 min [1 point]; after 60 min [0 point]); (ii) Do you find it difficult to refrain from smoking in places where it is forbidden? (Yes [1 point], no [0 point]); (iii) Which cigarette would you hate most to give up? (The first one in the morning [1 point], any other [0 point]); (iv) How many cigarettes per day do you smoke? (10 or less [0 point], 11–20 [1 point], 21–30 [2 points], and 31 or more [3 points]); (v) Do you smoke more during the first hours after waking than during the rest of the day? (Yes [1 point], no [0 point]); (vi) Do you smoke even when you are ill enough to be in bed most of the day? (Yes [1 point], no [0 point]). A total score for nicotine dependence (FTND) were obtained, 0–3 were categorized as minimal dependent, 3–7 were categorized as moderate dependent and 7–10 were severe dependent.
Operational definition
Subjects were interviewed about their tobacco status. They were classified as current tobacco user: Use tobacco regularly for within 1 month prior to examination; Nontobacco users: Never use tobacco or occasionally use tobacco; ex-tobacco user: Stopped more than 1 month prior to the examination. To determine the correlates of nicotine dependence, the sample was categorized based on their treatment into only two groups: Those with minimal or nondependent (FTND ≤3), and those with moderate to severe dependence (FTND >3). The questionnaire was anonymous, and anonymity had been maintained. First, we contacted contactor at construction units for permission to conduct the survey on their premises. Upon receipt of this permission, we then contacted recognized worker who mobilized and encouraged their co-workers to participate in the study. The study purpose was explained to all eligible participants, and verbal consent was obtained from all who elected to participate. Questionnaires were checked by investigators for completeness. Following completion, all participants were given a token of appreciation (free medicines if required) and appropriate treatment (counseling/pharmacotherapy) based on the scoring interpretation for nicotine dependence from Fagerstrom questionnaire and study finding in the tobacco cessation clinic of the hospital. They were referred to appropriate department if any health problem was identified.
Statistical analysis
The data were analyzed using IBM SPSS 22.0. Armonk, NY: IBM Corp. Chi-square test was used to evaluate the associations among nicotine dependence and the sociodemographic variables. The variables which were found to have a significant association in univariate analysis were further assessed by logistic regression analyses to identify the predictors of nicotine use and dependence. For analysis the dependents were grouped into two groups, the participants with moderate to severe dependence as per the score were considered at highly dependents and those falling into the mild category with scores 0–3 were considered as mild dependents.
RESULTS
All the construction site workers were males. The mean age of construction site workers was 32.04 ± 11.6 years. Among the workers, majority (91%) were tobacco users and out of these 49% were using smokeless tobacco, 29% were smokers bidi/cigarette and 22% were smokers as well as tobacco chewers [Table 1].
Table 1.
Pattern of tobacco use amongst construction site workers
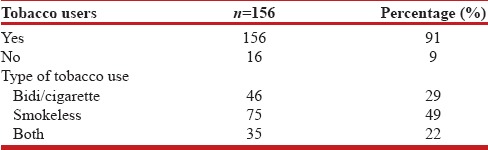
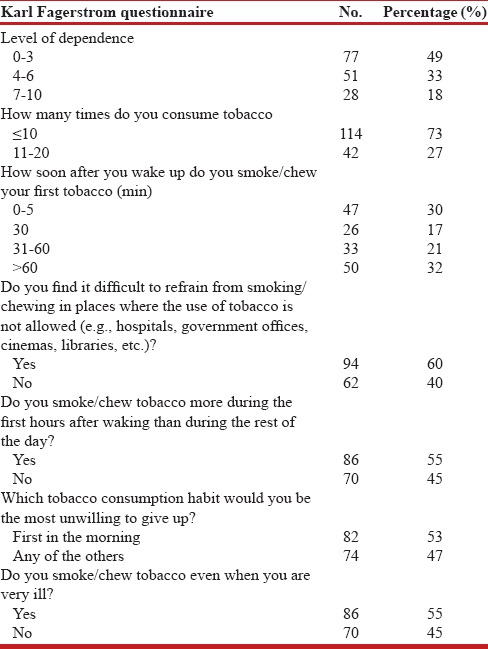
Table 2 shows Karl Fagerstrom Nicotine Tolerance and dependence among workers. It was found that 51% of tobacco users were moderate to severe nicotine dependent. Among the users, 60% found it difficult to refrain from smoking/chewing in places where the use of tobacco is not allowed (e.g., hospitals, government offices, cinemas, libraries, etc.). Slightly more than half (55%) of the users smoked or chewed tobacco more during the first hours after waking than during the rest of the day.
Table 2.
Distribution of workers as per the Karl Fagerstrom Nicotine Tolerance and dependence
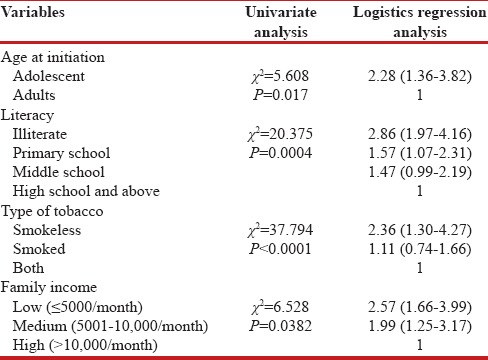
On univariate analysis, high dependence on use of tobacco was found to be significantly associated with age at initiation, lower education status, lower income group, type of tobacco use, electrocardiogram changes, knowledge regarding harmfulness of tobacco use and high blood pressure. The variables which were found to be significantly associated in univariate analysis were further analyzed by applying regression model. On regression analysis, the factors which were found to be significantly associated with high nicotine dependence were age at initiation (odds ratio [OR] 2.28, confidence interval [CI]: 1.36–3.82), lower income group (OR 2.57, CI: 1.66–3.99), smokeless tobacco use (OR 2.36, CI: 1.30–4.27) and lower education (OR = 2.86 [95% CI 1.97–4.16] for illiterate). Nagelkerkes R-value was found to be 0.488 [Table 3].
Table 3.
Binary logistic regression analysis to evaluate factors associated with dependence on nicotine
When we asked tobacco users as to why they started smoking, they came forward with multiple reasons. Among the users, 78.21% of them said because of peer pressure, 69.23% smoked in groups for time pass, 21.79% were influenced by family practice while 8.97% said they wanted to try something new, and 15% attributed their behavior to other reasons.
Among the users (79) those who had high nicotine dependent scores (>3), 10% had visited the health center for any ill health in the past month, while only 6% of those having low (≤3) nicotine dependent score (77) visited the health center in the past month for any ill health.
DISCUSSION
Majority of the participants were tobacco users (91%), and prevalence of smoking and tobacco chewing were 29% and 49%, respectively while 22% were using both. As per Laad et al. the prevalence of tobacco users were found to be 63.8%.[23] A study done by Akram et al. in Mangalore among industrial workers found the prevalence of tobacco use as 53.7% and prevalence of smoking, tobacco chewing was found to be 11.9% and 41.8%, respectively.[24] Ansari et al. found the prevalence of tobacco use among power loom workers in Mau Aima town, Allahabad district to be 85.9% and the prevalence of smoking and tobacco chewing among them were 62.28% and 66.07%, respectively.[25] Tobacco consumption was found to highly prevalent among the workers in the present study. Various reasons underlying could be poor literacy, lack of knowledge, and ignorance. The workers who were dependent on nicotine were highly motivated and counseled on harmful effects of tobacco and how to refrain from it.
Among the tobacco users, 18% of workers have a high level of nicotine dependence and 33% have a moderate level of nicotine dependence. Akram et al. found that 9.7% of industrial workers have a high level of nicotine dependence and 2.23% have a moderate level of nicotine dependence.[24] Our study highlights the relatively high prevalence of nicotine dependence in this population. The difference could be due to different methodology and study settings. Among the tobacco users, majority were illiterates. Manimunda et al. in their study conducted in Andaman also found lower educational status to be significantly associated with high nicotine dependence.[26] Another study on smoking prevalence among residents of resettlement colony in Delhi (India) in 2012 showed that the highest rate is found among the illiterate population.[27]
The average age at initiation of tobacco use was 16.5 years. As per Laad et al. the age of initiation was found to be 20.87 years.[23] High nicotine dependence was found to be significantly associated with the age of initiation.
Consumption of smokeless tobacco was significantly associated with nicotine dependence. The reasons could be due to the easy availability of smokeless tobacco and the fact that its consumption is not banned at public places. Ignorance regarding the harmful effect of smokeless tobacco use could be another factor associated with it.
While trying to address the social and economic impact of tobacco use and nicotine dependence, it was found that peer pressure, entertainment source, and family values greatly influence initiation of tobacco use. Saglam et al. in their study among health care workers found reasons such as wanting attention, stress, sadness, and curiosity for initiation of tobacco use.[28] These findings call for mass awareness and behavior change communication amongst the community to curb the myths and address the issue of nicotine dependence. More number of workers with moderate to high level of dependence visited health centers for ill health; this can be a leading factor for absenteeism and economic burden for the workers. Moreover, workers with lower income were more dependent on nicotine, thus making dependence a cause of vicious cycle of the economic burden.
Limitations of the study
Though the study provides useful information, it may have some limitations. The survey was done in the one construction site of Delhi, and hence the results can only be generalized to the sampled population. The cross-sectional nature of our study and self-reported rates of tobacco use are the major limitations of our study. Thus, the results demonstrate associations but do not provide evidence for causality. Moreover, due to the existing social taboo about tobacco use, all of them might not have participated in the survey. In spite of these limitations, we believe that our findings have not been significantly affected.
CONCLUSION AND RECOMMENDATIONS
The prevalence of tobacco use and dependence on nicotine was very high among construction workers compared to that in the general population. Factors found to be significantly associated include age at initiation, lower income group, smokeless tobacco use, lower education. Sensitization of workers and especially youth through schools and community-based awareness program about the problem, social support for deaddiction is needed. Income generation is strongly recommended as part of cessation strategy for this particular group. Recognition of construction sites as workplaces and proper implementation of the law for both form of tobacco is needed. Immediate other intervention programs are warranted to reduce the future burden of tobacco among these workers. Nicotine dependence prevalence estimates provide important baseline information that influences policy decisions on development and implementation of tobacco cessation strategies, particularly among this group. Proper behavior change communication package with motivation is required to abstain from or abandon the use of tobacco in this particular group.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jha P, Chaloupka FJ, Moore J, Gajalakshmi V, Gupta PC, Peck R, et al. Tobacco Addiction. Disease Control Priorities in Developing Countries. 2nd ed. Ch. 46. New York: Oxford University Press, World Bank; 2006. pp. 869–86. [Google Scholar]
- 2.WHO Report on the Global Tobacco Epidemic: Implementing Smoke-free Environments. Geneva: World Health Organization; 2009. [Last accessed on 2015 Nov 2]. Available from: http://www.who.int/tobacco/mpower/2009/en/ [Google Scholar]
- 3.Geneva: WHO; 2008. World Health Organization: WHO Report on Global Tobacco Epidemic 2008: MPOWER Package; pp. 7–9. [Google Scholar]
- 4.Peto R, Lopez AD, Boreham J, Thun M, Heath C, Doll R. Mortality from smoking worldwide. British Medical Bulletin. 1996;52:12–21. doi: 10.1093/oxfordjournals.bmb.a011519. [DOI] [PubMed] [Google Scholar]
- 5.National Cancer Institute. Smokeless Tobacco or Health: An International Perspective. Smoking and Tobacco Control Monograph 2. Bethesda, MD: National Cancer Institute; 1992. [Google Scholar]
- 6.US Department of Health and Human Services. The Health Consequences of Smoking: Nicotine Addiction: A Report of the Surgeon General. Washington, DC: US Government Printing Office; 1988. [Google Scholar]
- 7.WHO. WHO Report on the Global Tobacco Epidemic. World Health Organization. [Last assessed on 2015 Nov 22]. Available from: http://www.who.int/tobacco/global_report/2009/en/index.html .
- 8.U.S. Department of Health and Human Services. The health consequences of smoking. A report of the Surgeon General. Atlanta, Georgia: Centre for Disease Control, National Centre for Disease Prevention and Health Promotion, Office of Smoking and Health; 2004. [Google Scholar]
- 9.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013. pp. 571–4. [Google Scholar]
- 10.Smoking Statistics Fact Sheet. Manila, World Health Organization Regional Office for the Western Pacific. 2002. [Last accessed on 2015 Nov 15]. Available from http://www.wpro.who.int/media_centre/fact_sheets/fs_20020528.html .
- 11.Shiffman S, Scharf DM, Shadel WG, Gwaltney CJ, Dang Q, Paton SM, et al. Analyzing milestones in smoking cessation: Illustration in a nicotine patch trial in adult smokers. J Consult Clin Psychol. 2006;74:276–85. doi: 10.1037/0022-006X.74.2.276. [DOI] [PubMed] [Google Scholar]
- 12.WHO Worker's Health: Global Plan of Action. [Last accessed on 2015 Nov 15]. Available from: http://www.who.int/occupational_health/publications/global_plan/en/
- 13.Gaafar MA, Basiony LA. Pattern of smoking habit and quit attempts among industrial workers in Kuwait. Occup Med Health Aff. 2013;1:115. [Google Scholar]
- 14.Labour.nic.in. Informal Sector in India: Approaches for Social Security. [Last accessed on 2015 Nov 16]. Available from: http://www.labour.nic.in/ss/INFORMALSECTORININDIA-ApproachesforSocialSecurity.pdf .
- 15.Shah C, Sonaliya KN, Mehta HK. A study of socio demographic profile and addiction pattern among construction workers in Ahmedabad city, Gujarat. Indian J Prev Soc Med. 2012;43:188–91. [Google Scholar]
- 16.Mukherji S. Low quality migration in India: The phenomena of distressed migration and acute urban decay working for unorganised labour – The case of Mumbai. [Last accessed on 2015 Nov 05]. Available from: http://www Iariworg/papers/2009pdf .
- 17.Reddy KS, Gupta PC. Tobacco use in India: Practices, patterns and prevalence. Report on Tobacco Control in India. New Delhi, India: Ministry of Health and Family Welfare, Government of India; 2004. [Google Scholar]
- 18.World Health Organization: Global Adult Tobacco Survey (GATS)India Report 2009-2010. [Last accessed on 2015 Nov 19]. Available from: http://www.whoindia.org/EN/Section20/Section25_1861.html .
- 19.Global Adult Tobacco Survey Collaborative Group. Tobacco Questions for Surveys. A Set of Key Questions from the Global Adult Tobacco Survey. (GATS) 2nd ed. Atlanta, GA: Centre for Disease Control and Prevention; 2011. [Google Scholar]
- 20.Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for Nicotine dependence: A revision of the Fagerström tolerance questionnaire. Br J Addict. 1991;86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 21.Pomerleau CS, Carton SM, Lutzke ML, Flessland KA, Pomerleau OF. Reliability of the Fagerstrom tolerance questionnaire and the Fagerstrom test for nicotine dependence. Addict Behav. 1994;19:33–9. doi: 10.1016/0306-4603(94)90049-3. [DOI] [PubMed] [Google Scholar]
- 22.Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy's socioeconomic status scale-updating for 2007. Indian J Pediatr. 2007;74:1131–2. [PubMed] [Google Scholar]
- 23.Laad P, Adsul B, Chaturvedi R, Shaikh M. Prevalence of substance abuse among construction workers. Paripex Indian J Res. 2013;2:280–3. [Google Scholar]
- 24.Akram S, Gururaj NA, Nirgude AS, Shetty S. A study on tobacco use and nicotine dependence among plywood industry workers in Mangalore City. J Evol Med Dent Sci. 2015;4:5729–35. [Google Scholar]
- 25.Ansari ZA, Bano SN, Zulkifle M. Prevalence of tobacco use among power loom workers – A cross-sectional study. Indian J Community Med. 2010;35:34–9. doi: 10.4103/0970-0218.62551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Manimunda SP, Benegal V, Sugunan AP, Jeemon P, Balakrishna N, Thennarusu K, et al. Tobacco use and nicotine dependency in a cross-sectional representative sample of 18,018 individuals in Andaman and Nicobar Islands, India. BMC Public Health. 2012;12:515. doi: 10.1186/1471-2458-12-515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Garg A, Singh MM, Gupta VK, Garg S, Daga MK, Saha R. Prevalence and correlates of tobacco smoking, awareness of hazards, and quitting behavior among persons aged 30 years or above in a resettlement colony of Delhi, India. Lung India. 2012;29:336–40. doi: 10.4103/0970-2113.102812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Saglam L, Bayraktar R, Kadioglu EE, Acemoglu H. Smoking prevalance and the degree of nicotine dependence among healthcare workers at the ataturk university medical facility. Eurasian J Med. 2010;42:74–7. doi: 10.5152/eajm.2010.21. [DOI] [PMC free article] [PubMed] [Google Scholar]