

Abstract
Trichoepitheliomas are uncommon benign adnexal neoplasms that originate from the hair follicles. Multiple familial trichoepithelioma constitute an autosomal dominant disease characterized by the appearance of multiple flesh-colored, symmetrical papules, tumors and/or nodules in the central face and occasionally on the scalp. Although clinical diagnosis is usually straightforward in light of the family history and naked-eye examination, dermoscopy may aid in its confirmation. Dermoscopy of each papule revealed in-focus arborizing vessels, multiple milia-like cysts and rosettes amidst a whitish background.
In a patient with multiple facial papules revealing a dermoscopic appearance described above, the diagnosis of sporadic or familial multiple trichoepithelioma should be considered.
Keywords: trichoepithelioma, diagnosis, dermoscopy, dermatoscopy, CYLD
Introduction
Trichoepitheliomas are uncommon, benign, adnexal neoplasms that originate from the hair follicles. They usually present as solitary lesions but in the familial setting they appear as multiple lesions. Multiple familial trichoepithelioma constitute an autosomal dominant disease characterized by the appearance of multiple flesh-colored, symmetrical papules, tumors and/or nodules located in the central face and occasionally on the scalp [1].
Herein we present an interesting case of a female with multiple facial papules easily diagnosed as trichoepitheliomas with the use of dermoscopy.
Case report
A 29-year-old otherwise healthy female presented to our clinic for evaluation of multiple firm, flesh-colored, dome-shaped papules distributed primarily along the nasolabial folds and forehead. She first noticed their appearance during adolescence, after which they progressively increased in number (Figure 1). Scalp examination was unremarkable. Of note, she reported multiple relatives from her maternal lineage that developed similar lesions during youth.
Figure 1.


Multiple familial trichoepithelioma. Clinical presentation. (A) Overview image view. (B) Close-up. [Copyright: ©2016 Navarrete-Dechent et al.]
Dermoscopy of each papule revealed a similar appearance: in-focus arborizing vessels, multiple milia-like cysts and rosettes amidst a whitish background (Figure 2).
Figure 2.
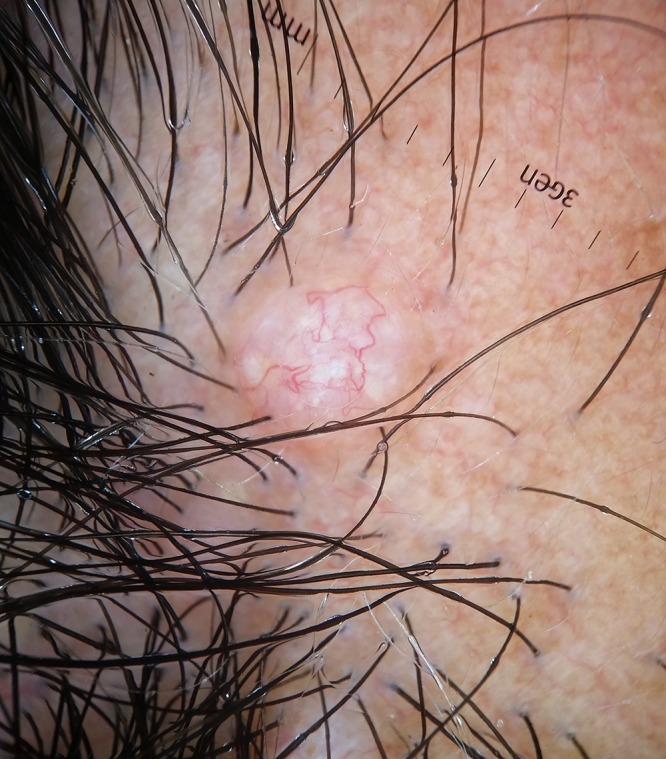
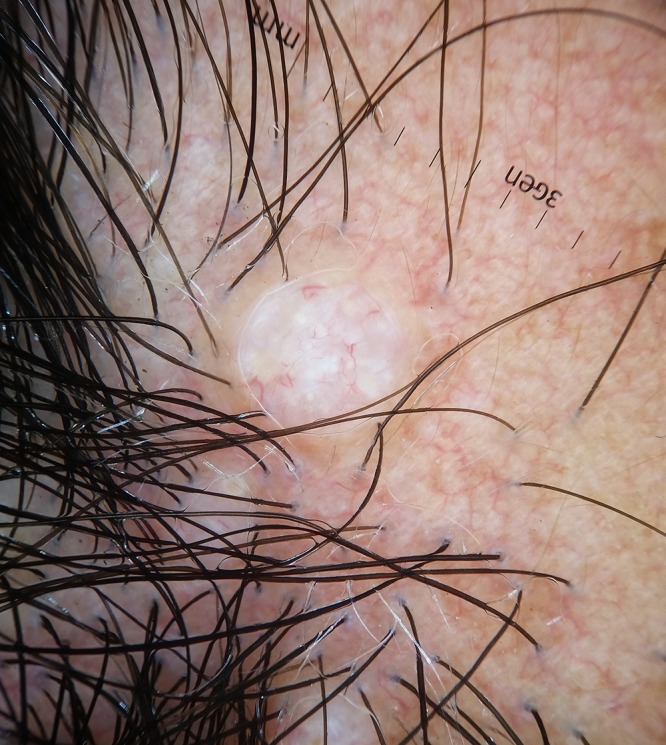
Dermoscopic features. (A) Image taken with contact polarized light. (B) Contact non-polarized light view. (Original magnification 10X). [Copyright: ©2016 Navarrete-Dechent et al.]
Histologic examination revealed a small, well-circumscribed, dermal tumor with branched nests of basaloid cells, small keratin cysts, and a rather dense collagenous stroma with visible fibrocytes, consistent with trichoepithelioma (Figure 3).
Figure 3.
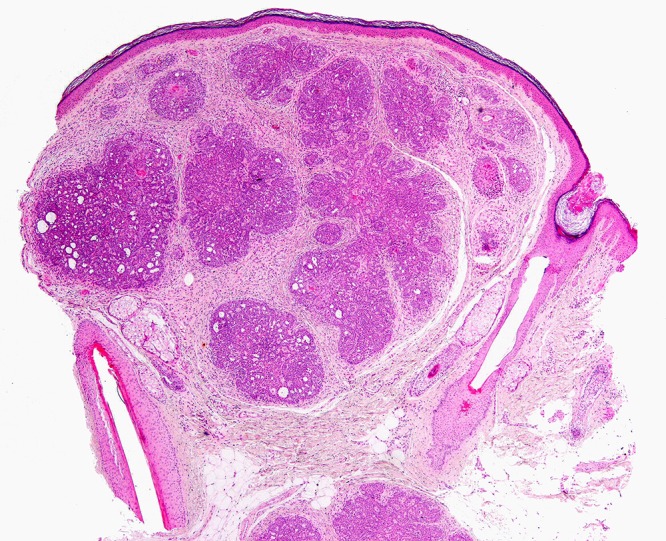
Photomicrograph showing a small, well-circumscribed, dermal tumor, with branched nests of basaloid cells, keratin cysts, and a dense collagenous stroma (H&E, 40×). [Copyright: ©2016 Navarrete-Dechent et al.
Discussion
Trichoepitheliomas are rare benign hamartomatous tumors originating from the pilosebaceous follicle. They most commonly present as solitary papules, but in the familial setting they appear in clusters characteristically involving the central face and/or the scalp [2]. They present with variable size from small papules that are of minor cosmetic relevance to multiple tumors that can lead to functional impairment such as visual obstruction. The incidence of multiple familial trichoepithelioma (OMIM #601606) in the US has been reported to be between 2.14—2.7 cases per year, with a female predilection [2,3]. They frequently first appear during childhood or adolescence.
Initially this disease was believed to be linked to loss in the heterozygosity of the 9p21 gene [4], however, recent studies have reported a mutation in the cylindromatosis tumor suppressor gene (CYLD) located in the chromosome 16q12-q13 in roughly 40% of cases [5]. This gene is a tumor suppressor gene altered in both multiple familial trichoepithelioma, familial cylindromatosis and in the Brooke-Spiegler syndrome [5]. In fact, those three conditions appear to be a spectrum of genodermatoses with a common molecular origin—CYLD mutation spectrum [6]—but with differing clinical manifestations [5,7–9]. Missense mutations of the CYLD gene appears to be more frequent in familial trichoepitheliomas than in Brooke-Spiegler syndrome or familial cylindromatosis and this may, in part, explain the phenotypic differences in these conditions [6].
While the PTCH gene was also thought to be linked to the etiopathogenesis of multiple familial trichoepithelioma, recent evidence suggests that it is rarely, if ever, mutated in this disease [7].
Dermoscopy allows for the noninvasive visualization of structures not visible to the naked eye, and when correctly interpreted improves the clinicians’ diagnostic accuracy. Although a facial papule displaying arborizing vessels and shiny white structures under dermoscopy is highly suggestive of basal cell carcinoma, the patient’s clinical history and the presence of numerous identical lesions raised the clinician’s suspicion for multiple familial trichoepithelioma. Importantly, each lesion had a similar dermoscopic morphology that was consistent with features that have previously been described for desmoplastic trichoepithelioma and solitary trichoepitheliomas, namely, arborizing vessels and milia-like cysts [10,11]. The presence of milia-like cysts in dermoscopy was correlated with the presence of keratin cysts in the histopathology (Figure 3).
When evaluating a solitary papule with the aforementioned dermoscopic findings, a biopsy may be necessary for definitive diagnosis. If a biopsy is contemplated, then it is important to underscore that small partial biopsies may lead the pathologist to misinterpreted the specimen as basal cell carcinomas [12]. Histopathology findings suggesting the diagnosis of trichoepithelioma over basal cell carcinoma include the fibrocytic loss of the stroma, aggregations of cells with smooth borders, the presence of granulomatous inflammation, monomorphic nuclei and papillary mesenchymal bodies [1].
Finally, treatment options for multiple trichoepithelioma include destructive/ablative techniques such as cryotherapy, dermabrasion, electrodissection and radiation therapy, all with variable to poor outcomes [2]. Interestingly, our patient chose not to undergo any treatment, which is also a valid option.
Conclusion
A patient evaluated with multiple facial papules that on dermoscopy reveal in-focus arborizing vessels, multiple milia-like cysts and rosettes amidst a whitish background should lead the clinician to consider the diagnosis of sporadic or familial multiple trichoepithelioma.
Footnotes
Funding: None.
Competing interests: The authors have no conflicts of interest to disclose.
All authors have contributed significantly to this publication.
References
- 1.Mapar MA, Ranjbari N, Afshar N, Karimzadeh I, Karimzadeh A. Severely disfiguring multiple familial trichoepitheliomas with basal cell carcinoma. Indian J Dermatol Venereol Leprol. 2014;80(4):349–52. doi: 10.4103/0378-6323.136924. [DOI] [PubMed] [Google Scholar]
- 2.Kataria U, Agarwal D, Chhillar D. Familial Facial disfigurement in multiple familial trichoepithelioma. J Clin Diagn Res. 2013;7(12):3008–9. doi: 10.7860/JCDR/2013/6218.3830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yiltok SJ, Echejoh GO, Mohammad AM, et al. Multiple familial trichoepithelioma: a case report and review of literature. Niger J Clin Pract. 2010;13(2):230–2. [PubMed] [Google Scholar]
- 4.Harada H, Hashimoto K, Ko MS. The gene for multiple familial trichoepithelioma maps to chromosome 9p21. J Invest Dermatol. 1996;107(1):41–3. doi: 10.1111/1523-1747.ep12297860. [DOI] [PubMed] [Google Scholar]
- 5.Young AL, Kellermayer R, Szigeti R, et al. CYLD mutations underlie Brooke-Spiegler, familial cylindromatosis, and multiple familial trichoepithelioma syndromes. Clin Genet. 2006;70(3):246–9. doi: 10.1111/j.1399-0004.2006.00667.x. [DOI] [PubMed] [Google Scholar]
- 6.Nagy N, Farkas K, Kemény L, Széll M. Phenotype-genotype correlations for clinical variants caused by CYLD mutations. Eur J Med Genet. 2015;58(5):271–8. doi: 10.1016/j.ejmg.2015.02.010. [DOI] [PubMed] [Google Scholar]
- 7.Kazakov DV, Vanecek T, Zelger B, et al. Multiple (familial) trichoepitheliomas: a clinicopathological and molecular biological study, including CYLD and PTCH gene analysis, of a series of 16 patients. Am J Dermatopathol. 2011;33(3):251–65. doi: 10.1097/DAD.0b013e3181f7d373. [DOI] [PubMed] [Google Scholar]
- 8.Zheng G, Hu L, Huang W, et al. CYLD mutation causes multiple familial trichoepithelioma in three Chinese families. Hum Mutat. 2004;23(4):400. doi: 10.1002/humu.9231. [DOI] [PubMed] [Google Scholar]
- 9.Farkas K, Deák BK, Sánchez LC, et al. The CYLD p.R758X worldwide recurrent nonsense mutation detected in patients with multiple familial trichoepithelioma type 1, Brooke-Spiegler syndrome and familial cylindromatosis represents a mutational hotspot in the gene. BMC Genet. 2016;17(1):36. doi: 10.1186/s12863-016-0346-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ardigo M, Zieff J, Scope A, et al. Dermoscopic and reflectance confocal microscope findings of trichoepithelioma. Dermatology. 2007;215(4):354–8. doi: 10.1159/000107631. [DOI] [PubMed] [Google Scholar]
- 11.Lazaridou E, Fotiadou C, Patsatsi A, et al. Solitary trichoepithelioma in an 8-year-old child: clinical, dermoscopic and histopathologic findings. Dermatol Pract Concept. 2014;4(2):55–58. doi: 10.5826/dpc.0402a11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Poniecka AW, Alexis JB. An immunohistochemical study of basal cell carcinoma and trichoepithelioma. Am J Dermatopathol. 1999;21(4):332–6. doi: 10.1097/00000372-199908000-00004. [DOI] [PubMed] [Google Scholar]