

Abstract
The ability to manage financial affairs is a life skill of critical importance, and neuropsychologists are increasingly asked to assess financial capacity across a variety of settings. Sound clinical assessment of financial capacity requires knowledge and appreciation of applicable clinical conceptual models and principles. However, the literature has presented relatively little conceptual guidance for clinicians concerning financial capacity and its assessment. This article seeks to address this gap. The article presents six clinical models of financial capacity : (1) the early gerontological IADL model of Lawton, (2) the clinical skills model and (3) related cognitive psychological model developed by Marson and colleagues, (4) a financial decision-making model adapting earlier decisional capacity work of Appelbaum and Grisso, (5) a person-centered model of financial decision-making developed by Lichtenberg and colleagues, and (6) a recent model of financial capacity in the real world developed through the Institute of Medicine. Accompanying presentation of the models is discussion of conceptual and practical perspectives they represent for clinician assessment. Based on the models, the article concludes by presenting a series of conceptually oriented guidelines for clinical assessment of financial capacity. In summary, sound assessment of financial capacity requires knowledge and appreciation of clinical conceptual models and principles. Awareness of such models, principles and guidelines will strengthen and advance clinical assessment of financial capacity.
Keywords: Financial capacity, Financial competency, Conceptual models, Clinical assessment
The ability independently to manage one's financial affairs, known as financial capacity, is an everyday life skill of critical importance (Marson & Hebert, 2008; Marson, 2013; Marson, Triebel, & Knight, 2012; Widera, Steenpass, Marson, & Sudore, 2011). Financial capacity is tied closely to personal independence and successful function in the community, and has been equated in importance to “diet, exercise, and sleep” as a key indicator of overall health status in adults (Connolly, April 28, 2015). Clinicians including neuropsychologists are increasingly called upon to assess financial capacity (Widera et al., 2011). Yet despite its critical role as an everyday life skill, there is relatively little scientific literature and conceptual guidance available for clinicians and legal professionals concerning financial capacity as a topic, and in particular concerning its assessment in clinical and forensic settings.
Sound clinical and forensic assessment of financial and other capacities requires an understanding and appreciation of conceptual models of the capacity. Implicit in any financial capacity finding or judgment is an underlying conceptual approach to identifying, organizing and weighing specific capacity evidence deemed relevant to the assessment. Awareness of and adoption of a conceptual approach is often integral to a well-crafted assessment. Unfortunately, clinicians and forensic examiners have had few explicit clinical conceptual models of financial capacity available for guidance. As a result, in many cases the clinician or forensic examiner may not know how best to proceed conceptually and the approach may thus have flaws or limitations that reduce the assessment's efficacy.
As noted earlier, it is now well accepted that financial capacity is an important capacity both clinically and forensically. Yet since Lawton's seminal paper on IADLs published in 1969 (Lawton & Brody, 1969), it is notable how little conceptual work has been conducted relevant to financial capacity. As part of a detailed literature search, in the three decades between 1970 and 1999 we found no conceptual studies of financial capacity as a clinical or a legal construct.1 The first systematic theoretical efforts in this area only emerged in 2000 (Griffith et al., 2003; Marson et al., 2000) and have slowly accumulated since that time (Pinsker, Pachana, Wilson, Tilse, & Byrne, 2010). Although very recent work is now expanding the theoretical base (Lichtenberg, Stoltman, Ficker, Iris, & Mast, 2015; Medicine & National Academies of Sciences, 2016), financial capacity still largely remains a relatively poorly understood construct for clinicians, researchers, and forensic examiners.
The lack of conceptual models relates to multiple factors. These include the inherent complexity of financial capacity as a construct, its operation over multiple contexts and time frames in daily life, the diversity and breadth of financial skills and activities necessary in modern society, the degree to which financial experience varies across individuals, and the complicating effects of race and culture (Triebel, Okonkwo, Martin, Griffith, Crowther, & Marson, 2010). As a result, few clinical and forensic models of financial capacity exist, and there is not a model of financial capacity that currently unifies clinical and forensic perspectives.
Another important consequence of the lack of conceptual models is the relative scarcity and unavailability of dedicated assessment measures of financial capacity. There is a close relationship between conceptual modeling of a construct and the development of associated assessment measures. Although a number of general functional assessment measures incorporate financial subtests or items (Loeb, 1996; Loewenstein et al., 1989; Patterson, Goldman, McKibbon, Hughes, & Jeste, 2001), there are currently only a handful of measures specifically dedicated to the assessment of financial skills (Kershaw & Webber, 2008; Lichtenberg et al., 2015; Marson et al., 2000, 2009). The lack of dedicated assessment measures thus reflects the conceptual knowledge gap, and also contributes to clinician uncertainty as to how to best address these assessment questions.
This article is organized into two sections. In Section 1, we assemble and organize available conceptual work on financial capacity relevant to clinicians. Although forensic models of financial capacity also exist, they are not the focus of this article, which is rather targeted to neuropsychologists and other clinicians assessing financial capacity in clinical practice. The article presents six clinical models of financial capacity, and the different and evolving conceptual and practical perspectives they represent for clinical assessment of this capacity. In Section 2, we present conceptually oriented guidelines for clinical assessment of financial capacity that draw on these conceptual models and their underlying principles.
Clinical Conceptual Models of Financial Capacity
Early Gerontological Model: Financial Capacity as an IADL
An early model of financial capacity was presented by Powell Lawton and his colleague Elaine Brody as part of their seminal article on IADLs in older adults published in 1969 (Lawton & Brody, 1969). In this article Lawton and Brody described two key domains of function for older adults: (1) physical self-maintenance or self-care functions, and (2) more complex instrumental activities of daily life (IADLs) involving “instrumental self-maintenance” (Lawton & Brody, 1969, p. 179). The IADL domain included telephone use, shopping, food preparation, housekeeping, laundering, use of transportation, use of medicine, and importantly financial behavior described simply as the “ability to handle finances” (Lawton & Brody, 1969, p. 181). The authors viewed both men and women as exercising financial skills and thus both genders could be validly assessed using the financial IADL construct.
As part of their article, Lawton and Brody offered a rudimentary classification scheme for level of independent function across different IADLs. For financial behavior, they described three basic levels (Lawton & Brody, 1969, p. 181).2:
Manages financial matters independently (budgets, writes checks, pays rent, bills, goes to bank), collects and keeps track of income. [Level 1-Independent].
Manages day-to-day purchases, but needs help with banking, major purchases, etc. [Level 2-Partially Dependent].
Incapable of handling finances. [Level 3-Dependent].
Although simplistic to our modern eye, this framework represented one of the first efforts to recognize and schematize financial skills in community dwelling adults, and is still useful today. As noted, the model identified three levels of functioning, beginning with independent financial function (Level 1), which encompasses higher order activities of budgeting, tracking income, writing checks and engaging in bank transactions, and paying rent and other bills. Although not explicitly stated, Level 1 also implicitly encompasses lower order financial skills such as daily purchases. The second level involves circumstances of partial dependence on others in financial function (Level 2), where the individual can still carry out lower order skills such as daily purchases, but needs assistance with the higher order banking and transaction activities described for Level 1. The third level concerns complete dependence on others in financial function (Level 3) and is described simply as “incapable of handling finances” without additional description or elaboration.
Despite its simplicity, the Lawton IADL model has stood the test of time. The model's core contribution has been to conceptualize financial capacity and other IADLs as sets of specific instrumental skills that help maintain an older adult's independent functioning in the community. In addition, the classification of dependence levels in function anticipated and has supported more detailed modern functional impairment classifications based on concepts of fully capable/independent (“can do without help”), partially capable/partially dependent (“can do with help”), and incapable/dependent (“cannot do even with help”) (Marson & Hebert, 2005). Although intended for assessment of the elderly, the IADL model and financial IADL construct also have utility for younger adult clinical populations such as patients with multiple sclerosis and traumatic brain injury.
At the same time, it should be recognized that the Lawton and Brody IADL model of financial capacity is limited in scope and detail. Obvious gaps in the model include failure to include financial decision-making tasks, financial judgment abilities (such as avoidance of scams and fraud), and higher order financial skills such as bank statement use, completing/filing tax returns, and making a will and estate plan. Lawton's model also did not address more basic but important financial skills such as identifying and counting coins/currency or understanding coin/currency relationships. As discussed below, many of these missing financial skills and activities are incorporated into more recent models of financial capacity.
The IADL model of financial capacity has utility for clinical assessment through its focus on the level of independent financial function of the individual. A general capacity question clinicians continually encounter is whether or not the individual is still able to live independently. The individual's relative independence in carrying out the financial IADL is many times a critical finding for such clinical judgments. Similarly, in forensic proceedings it is important for the court and parties to know whether the individual has sufficient financial skills to handle his/her financial affairs and estate and, if not, a conservator or guardian of the estate (the terminology varies by state) is appointed. If he or she is not able to live independently in the community a general guardianship is appointed that encompasses financial affairs and other activities. Impairment or loss of the financial IADL will significantly affect a court's decisions on both issues.
Clinical Model: Financial Capacity as Financial Skills Relevant to Independence
As an extension of the early IADL model, financial capacity can also be conceptualized as a broad set of clinically relevant financial skills and activities necessary for independent function in the community. These range from very basic skills of identifying and counting coins/currency and conducting cash transactions (Marson et al., 2012), to higher level abilities of managing a checkbook and reviewing a bank statement, to complex activities of making investment decisions. In this clinical model, financial capacity can be understood to have both performance and judgment dimensions (Marson et al., 2012). To possess financial capacity, a person must be able to perform a variety of tasks and skills to meet his or her needs within his/her life context—i.e., live independently. Such tasks and skills include understanding basic financial concepts, possessing basic monetary skills, carrying out cash transactions, and paying bills. In addition to such performance skills, in order to live independently an individual must also be able to exercise judgment and decision making to promote his or her own financial well-being. Thus, in addition to performance skills, the individual must be able to perform financial activities in ways that promote and protect his or her self or best interest (Marson et al., 2000; Marson, 2001; Marson, Hebert, & Solomon, 2011). There are many individuals who possess good financial performance skills but are unable to exercise them in ways that support their best interest. An example is the patient with schizophrenia who despite adequate financial knowledge and performance skills has poor judgment and dissipates her monthly entitlement check on illicit drugs, thereby losing her home or placement and becoming homeless.
In response to the absence of available comprehensive conceptual models, in the late 1990s our research group at University of Alabama Birmingham developed a clinical model of financial capacity based on skills and activities deemed relevant to the independent functioning of community dwelling older adults (Marson et al., 2000). Our group was interested in studying financial skill decline occurring in Alzheimer's disease and recognized the need at the onset to establish a model of everyday financial skills relevant to community dwelling older adults. We initially identified everyday tasks/activities with the following characteristics:
Clinical relevance to independent function
Represented both simple and complex abilities
Represented declarative, procedural, and judgmental knowledge sources
In constructing the clinical model, we conceptualized financial capacity as a series of domains of activity that each had specific clinical relevance to independent function (Griffith et al., 2003; Marson et al., 2000; Marson, 2001). Examples of such domains included basic monetary skills, conducting cash transactions, managing a checkbook and a bank statement, and exercising financial judgment. This domain-based approach was clinically oriented and consistent with the presumed multidimensionality of financial capacity and its variability across individuals. It is also consistent with the legal principle of limited financial competency adopted within most state legal jurisdictions that recognizes that an individual may be competent to carry out some financial activities but not others (Grisso, 1986; Marson et al., 2000; Marson et al., 2011; Marson, 2001).
In addition to domains of activity, our clinical model identified specific financial abilities or tasks (Marson et al., 2000, 2001). Tasks reflect more basic financial skills that taken together comprise domain level capacities. For example, the domain of “financial conceptual knowledge” draws upon specific declarative abilities, such as understanding simple concepts (e.g., a loan or savings) and also procedural and judgmental abilities involved in applying concepts in everyday life (e.g., selecting interest rates or identifying a medical deductible). The domain of “checkbook management” was conceptualized to include declarative abilities such as naming and defining the parts of a checkbook/register, and also procedural abilities of using a checkbook/register in everyday transactions. The domain of “financial judgment” drew upon explicit judgmental tasks related to detection/awareness of possible financial fraud. Therefore, tasks represented abilities that, taken together, constitute broader, clinically relevant domains of financial activity. We defined tasks as being simple or complex depending on the level of cognitive difficulty they appear to require (Marson et al., 2000; Marson et al., 2011; Marson, 2001).
The UAB clinical model has undergone revision and now also considers financial capacity at the global level (Griffith et al., 2003; Marson, 2001). Clinical capacity, as well as legal capacity or competency, are ultimately overall categorical judgments or classifications made by a clinician or legal professional. Thus, the UAB clinical model of financial capacity now has three levels (Griffith et al., 2003):
specific financial abilities or tasks, each of which is relevant to a particular domain of financial activity;
general domains of financial activity, which each have clinical relevance to independent function in the community; and
overall financial capacity, which reflects a global estimate of capacity based on the totality of domain- and task-level performance.
This clinical model of financial capacity, presented in Table 1, comprises 9 domains, 18 tasks, and two global levels (Griffith et al., 2003; Marson et al., 2000, 2008; Marson, 2001; Marson et al., 2011).
Table1.
UAB clinical conceptual model of financial capacity: 18 tasks, 9 domains, 2 global scores
| Domain/Task | Description | Difficulty |
|---|---|---|
| Domain 1 | Basic Monetary Skills | |
| Task 1a Naming Coins/Currency | Identify specific coins and Currency | Simple |
| Task 1b Coin/currency relationships | Indicate relative monetary values of coins/currency | Simple |
| Task 1c Counting coins/currency | Accurately count groups of coins and currency | Simple |
| Domain 2 | Financial Conceptual Knowledge | |
| Task 2a Define financial concepts | Define a variety of financial concepts | Complex |
| Task 2bApply financial concepts | Practical application/computation using concepts | Complex |
| Domain 3 | Cash Transactions | |
| Task 3a1 item grocery purchase | Enter into simulated 1 item transaction; verify change | Simple |
| Task 3b3 item grocery purchase | Enter into simulated 3 item transaction; verify change | Complex |
| Task 3cChange/vending machine | Obtain change for vending machine use; verify change | Complex |
| Task 3dTipping | Understand tipping convention; calculate/identify tips | Complex |
| Domain 4 | Checkbook Management | |
| Task 4a Understand checkbook | Identify and explain parts of check and check register | Simple |
| Task 4b Use checkbook/register | Enter into simulated transaction; pay by check | Complex |
| Domain 5 | Bank Statement Management | |
| Task 5a Understand bank statement | Identify and explain parts of a bank statement | Complex |
| Task 5b Use bank statement | Identify specific transactions on bank statement | Complex |
| Domain 6 | Financial Judgment | |
| Task 6a Detect mail fraud risk | Detect and explain risks in mail fraud solicitation | Simple |
| Task 6c Detect telephone fraud risk | Detect and explain risks in telephone fraud solicitation | Simple |
| Domain 7 | Bill Payment | |
| Task 7a Understand bills | Explain meaning and purpose of bills | Simple |
| Task 7b Prioritize bills | Identify bills that need immediate attention | Simple |
| Task 7c Prepare bills for mailing | Prepare simulated bills, checks, envelopes for mailing | Complex |
| Domain 8 | Knowledge of Assets/Estate | |
| Indicate/verify asset ownership, estate arrangements | Simple | |
| Domain 9 | Investment Decision-Making | |
| Understand investment options/returns; make decisions | Complex | |
| Global 1Domains 1–7 | Overall performance across domains 1–7 and tasks | |
| Global 2 Domains 1–9 | Overall performance across domains 1–9 and tasks |
Adapted from and reprinted with permission from (Griffith et al., 2003), the American Academy of Neurology.
As noted, in many ways the UAB clinical skills model can be viewed as an extension and elaboration of the earlier Lawton IADL model. Although the clinical model encompasses a much broader range of financial tasks and activities than the Lawton IADL model, conceptually it is organized around the same premise of independent function in the community. The clinical skill model has been the basis for instrument development by the UAB group, including the Financial Capacity Instrument (FCI) (Griffith et al., 2003; Marson et al., 2000), the FCI-Short Form (FCI-SF) (Gerstenecker et al., 2015; Marson et al., 2014), the Semi-Structured Clinical Interview for Financial Capacity (SCIFC) (Marson et al., 2009), and the Current Financial Capacity Form (CFCF) (Wadley, Harrell, & Marson, 2003). The model and different assessment instruments associated with it have also supported multiple empirical studies of financial capacity in MCI and Alzheimer's dementia, Parkinson's disease, and TBI (Dreer, Devivo, Novack, & Marson, 2012; Griffith et al., 2003; Marson et al., 2000, 2009; Marson et al., 2011; Marson et al., 2012; Marson, 2001; Martin et al., 2013).
The clinical skills model of financial capacity is intuitively attractive for clinical practice because it encompasses many everyday financial skills associated with independent living. The conceptual framework of tasks, domains, and global financial capacity also has utility for hierarchically organizing financial skills and activities, and for thinking clinically about a particular individual's financial skill set. At the same time, the model has some limitations. First, the multiple financial tasks and domains may not always map on or relate to every individual and their financial environment. As noted, the model was initially developed to promote investigation of financial skill decline in older persons with Alzheimer's disease. Thus it inherently assumes a particular developmental and financial skill context—older adults who generally have enjoyed a lifetime of both normal cognitive function and normal financial skill acquisition and financial functioning—who now are declining across a range of financial tasks and activities. It is not as well suited, for example, to adults with neurodevelopmental and young adults with psychiatric disorders like schizophrenia. These individuals developmentally do not experience normal cognition and financial skill acquisition, and as a result do not typically exercise many higher order financial skills contemplated by the clinical model, such as checkbook management, bank statement management, bill payment, estate planning, and investment decision-making. Instead, these individuals may rely on very basic coin/currency and simple transaction skills, and pay for services with cash or money orders. Thus the UAB clinical skill model as presented is linked to a particular psychosocial background and SES level. This limitation notwithstanding, the core domains and skills of the model (domains 1–7) apply to a very large segment of the adult U.S. population and thus the model is relevant across many age groups and disorders.
In a similar vein, the clinical model as presented does not currently extend to digital and online banking, and is rooted more in 20th century than 21st century financial modalities (although 20th century financial modalities remain highly relevant to the older adult cohort). However, the UAB clinical model is flexible and currently is being elaborated to incorporate electronic banking and other modern digital financial activities.
Cognitive Psychological Model: Financial Capacity as Types of Financial Knowledge
Cognitive psychology provides another conceptual vantage point for understanding financial capacity. In this model, financial capacity comprises a broad range of declarative, procedural, and judgment based financial abilities and skills important for independent function (Marson et al., 2000; Moye & Marson, 2007; Pinsker et al., 2010). Declarative knowledge concerns knowledge of personal (autobiographical) and general facts and information acquired over the course of a lifetime. It is often divided into personal episodic knowledge of the world (e.g., first day of school, trip to England) and into semantic knowledge which is memory for facts, knowledge of the world, and meaning of words and concepts (Anderson, 1976). Declarative knowledge for finances thus involves the ability to describe personal and general facts and concepts and events related to financial activities. For example, financial declarative knowledge includes knowledge of personal financial data and investment decisions, as well as knowledge of the value of coins and currency, rules for doing arithmetic problems, and the meanings of financial terms such as interest rate, loan, and bond.
In contrast, procedural knowledge is knowledge exercised in conducting or accomplishing a task such as playing a piano or driving a car. Unlike declarative knowledge, procedural knowledge may not be readily described or articulated, as it may acquired without explicit awareness and may be exercised in daily life in a nonconscious or tacit manner (Stadler, 1989; Stillings, Weisler, Chase, Feinstein, Garfield, & Rissland, 1995). Procedural financial knowledge includes the ability to carry out over-learned, motor based financial skills and routines such as making change, writing checks, using an ATM machine, and conducting simple on-line banking transactions (Moye & Marson, 2007). The emphasis is not on the declarative knowledge informing the task but on the skills in “how” to carry out the financial task.
Judgment, which we reference as judgmental knowledge, involves the ability to use declarative and procedural financial knowledge/skills to make personal decisions consistent with self- or best interest, in daily as well as novel or ambiguous situations (Marson et al., 2000; Moye & Marson, 2007). Judgment is thus a crucial aspect of financial capacity. For example, a person with mental illness can have a range of intact financial performance skills (declarative and procedural financial knowledge) but lack financial capacity due to failures of judgment in making decisions inconsistent with self- or best interest. Put differently, financial judgment is a critical form of emotional and self-awareness and knowledge that is linked to self-attention, executive function, and goal orientation, and that permits a person correctly to “interpret” a financial situation and make decisions that promote best interest. Exercising good judgment is an aspect of what Lichtenberg has called a person's “financial situational awareness” (Lichtenberg et al., 2015).
Many financial tasks involve a combination of declarative, procedural, and judgmental knowledge. One example involves making a new will. In making a will, a person needs to have declarative knowledge as to what a will is, who are his/her natural and other heirs (“objects of bounty” such as family members, as well as friends and charities, and the nature and extent of assets passing under the will (e.g., real estate holdings, bank and brokerage accounts, personal property). Procedural aspects of a will execution for the testator involve reading the will and then executing it by signing. Judgmental aspects of a will signing include deciding on how best to divide up one's estate among potential heirs, what financial amounts or shares to assign respective heirs, the timing of such distributions under the will and testamentary trust, and who to serve as executor or personal representative of the estate.
A different example is a bond purchase. In purchasing a bond, an individual needs to have declarative knowledge that a bond is a type of debt security, knowledge of the meaning of associated financial terms such as coupon (interest rate), maturity date (date that the bond's principal becomes payable to bond holder), and yield to maturity (expected return over time). From a procedural knowledge standpoint, the individual needs to contact his/her broker or dealer, discuss the basic terms of purchase, and place a bond purchase order. With respect to judgmental knowledge, the individual purchasing the bonds needs to determine whether or not the bond issue is of investment grade or lower (junk), confirm that the company issuing the debt has acceptable credit worthiness, establish that the bond purchase fits within the individual's overall investment strategy, and that the yield to maturity is acceptable given the risk of issuer default being assumed.
Like the IADL model, the cognitive psychological model has potential utility for assessment of financial capacity. It may be useful in some cases for clinicians to analyze a patient or client's financial strengths and deficits through the lens of declarative, procedural and judgmental knowledge. Such an inquiry may also lead the clinician to better understand the neurocognitive and behavioral abilities that may underlie an individual's financial capacity strengths and deficits. Such knowledge may have potential value in both clinical and forensic assessments of financial capacity, allowing both families and courts additional insight into the type of skills and deficits present and their implications for financial activity.
The cognitive psychological model above also has limitations. As noted by Pinsker and colleagues (2010), the model focuses heavily on cognitively mediated knowledge and functional skills, thereby underestimating the contribution of social, emotional, and other contextual factors to financial function: “Although this view does well to conceptualize the cognitive and functional aspects of financial capacity, it falls short of fully specifying the social and cultural influences on financial capacity” (Pinsker et al., 2010, p. 333). However, these social, affective, and contextual factors, although important to recognize and consider, may also be understood ultimately to influence and shape an individual's expression of the three core forms of financial knowledge. Viewed in this way, the three core forms of financial knowledge remain highly relevant to financial capacity irrespective of the individual's personal circumstances and milieu.
Decision-Making Model: Financial Capacity as Core Decision-Making Abilities
Another conceptual vantage point for thinking clinically about financial capacity is as a decisional capacity. It is important to recognize that the financial capacity construct is notably broader than financial decision-making per se, as it encompasses basic everyday knowledge and performance skills that are not inherently “decisional” in nature (e.g., counting coins/currency, purchasing groceries, completing a check register, using an ATM machine). Nonetheless, financial decision-making is a critical dimension of financial capacity, as it is linked to high value transactions such as investment and estate planning decisions and informs other key financial activities such as preparing a budget or an annual income tax return, or deciding to accept or reject a scam attempt). For this reason, conceptual models of financial decision-making are highly relevant to clinical and forensic assessment and warrant theoretical attention.
A well established and applied clinical model of decisional abilities has been set forth by Paul Appelbaum, Thomas Grisso, and colleagues (Grisso & Appelbaum, 1998). The model comprises four core decisional abilities that were adduced from case law and the psychiatric literature on competence (Appelbaum & Grisso, 1988; Roth, Meisel, & Lidz, 1977). These core decisional abilities are:
evidencing a choice (yes or no) regarding a decision (Choice);
understanding the decisional situation and choices (Understanding);
appreciating consequences to one personally of a particular choice (Appreciation); and
reasoning about choices in the decisional situation (Reasoning).
Taken together, these four abilities represent different components of specific decision-making capacity (Marson, Schmitt, Ingram, & Harrell, 1994). The decisional model was initially developed in connection to assessment of treatment consent capacity (also known as medical decision-making capacity) and later was adapted for assessment of research consent capacity (Grisso & Appelbaum, 1998). However, the model is adaptable to many other decision-making contexts including financial capacity. Applied to the financial sphere, the four decisional abilities can be framed as follows:
Choice: ability to make a choice about a financial transaction or situation;
Understanding: ability to “understand” information relevant to a financial transaction/situation and associated choices about the transaction/situation;
Appreciation: ability to “appreciate” consequences to one personally of different choices relevant to the financial transaction/situation; and
Reasoning: ability to “reason” and think logically about different choices presented by a financial transaction/situation.
The decisional model is attractive because it provides a readily usable conceptual framework for analyzing a person's capacity to make specific financial decisions, which as noted is a core aspect of financial capacity. The model has served as the conceptual basis of two recent measures of financial capacity (Lai, Gill, Cooney, Bradley, Hawkins, & Karlawish, 2008; Lichtenberg et al., 2015). Karlawish & Lai (2008) have developed a measure (Assessment of Capacity for Everyday Decision-Making, or ACED) which uses the decisional model to assess an older adult's capacity to accept or refuse an intervention for problems managing IADLs such as finances, meal preparation, and managing medication (Karlawish & Lai, 2008; Lai et al., 2008; Lichtenberg et al., 2015; Yu, Lui, Lam, Chiu, Karlawish, & Appelbaum, 2009). Lichtenberg and colleagues have drawn upon the same decisional model to develop a new measure (the Lichtenberg Financial Decision Rating Scale, or LFDRS) (discussed below) that assesses an individual older adult's capacity to make “sentinel” financial decisions free from the effects of undue influence and financial exploitation (Lichtenberg et al., 2015).
Given its established track record in other areas of clinical decision-making, the decisional model has considerable potential in situations/transactions where the core clinical issue is capacity to make a financial decision such as an investment or estate planning. At the same time, the model's focus on decision-making is also its inherent limitation, as the model does not apply readily to non-decisional aspects of the financial capacity construct. For example, the decisional model arguably cannot fully address the question of whether a young adult with severe mental illness can manage his/her overall financial affairs, because the model only focuses on key decision-making questions and not on the individual's day-to-day financial activities and performance which in many cases of severe mental illness may ultimately be more critical to independence. Another limitation may relate to forensic applications. The decisional model as of yet has not been applied consistently in forensic settings, where legal standards for capacity to conduct financial transactions are based on common law precedent and statutory language distinct from the decisional abilities model. However, new instruments like the ACED and LFDRS, which incorporate these decisional abilities, may increasingly be used by clinicians called upon to testify in forensic matters. Time will tell as to whether the decisional model establishes itself as a commonly used conceptual approach to answering questions of financial capacity.
Person-Centered Model of Financial Capacity
Recent gerontological research has focused on the value of a person-centered approach to working with older adults with neurocognitive disorders (Fazio, 2013). This approach advocates viewing an individual as a unique whole with specific strengths as well as weaknesses, and with unique subjective experiences (Mast, 2011). Lichtenberg has adopted this person-centered orientation in developing a conceptual model of financial capacity that seeks to integrate research on financial decisional abilities and financial exploitation/abuse (Lichtenberg et al., 2015).
A key premise and catalyst for Lichtenberg is that existing models and measures of financial capacity address assessment issues generically with neutral or hypothetical stimuli (“How many dimes in $1.50?” or “What is a loan?”), rather than focusing on the specific individual and his/her actual financial situation and decision-making abilities and judgment (Lichtenberg et al., 2015). As noted earlier, Lichtenberg and his group are particularly interested in an individual's ability to make important or “sentinel” financial decisions that are free from financial exploitation and undue influence and that are consistent with prior financial values. In effect, a three prong model of financial decisional capacity is proposed. Using a person-centered approach, the model seeks to integrate the four core abilities of the decision-making model (described by Lichtenberg as “intellectual factors”) with simultaneous consideration of various risks of financial exploitation (described as “contextual factors”) and the individual's lifelong financial values (“values”). Put differently, the model seeks to evaluate “integrity of financial decisional ability” through a person-centered approach that considers, in the setting of a specific financial decision or transaction: (1) an individual's vulnerability to exploitation and undue influence (contextual factors), (2) his/her core decisional abilities (intellectual factors), and (3) his/her adherence to personal financial values. As noted, the model has given rise to an associated assessment measure, called the Lichtenberg Financial Decision Making Rating Scale (LFDRS) (Lichtenberg et al., 2015).
The person-centered model, although new and largely untested, represents an innovative and potentially valuable contribution to the growing clinical conceptual literature on financial capacity. Because it explicitly focuses on the individual, it has particular relevance to forensic settings where an individual's decisional capacity regarding a specific transaction is frequently at issue. The model may have less relevance to clinical settings where the clinician's focus is often less on a specific transaction and more on the individual's capacity to manage his/her overall financial affairs successfully over time. A second criticism is that all financial capacity evaluations ultimately focus on an individual and his or her financial abilities, so in a sense all conceptual models of financial capacity are person-centered in application.
Institute of Medicine Model: Financial Capacity as Financial Function in the Real World
The Institute of Medicine (IOM) and National Academy of Science (NAS), through an hoc committee entitled the Committee to Evaluate the Social Security Administration's Capability Determination Process for Adult Beneficiaries recently made an important theoretical contribution to the conceptualization of financial capacity (Medicine & National Academies of Sciences, 2016). The committee was constituted and charged by the IOM in 2015 to conduct a study to evaluate the Social Security Administration's (SSA's) capability determination process for adults receiving SSA disability benefits (SSA beneficiaries), and to provide recommendations to improve the accuracy and efficiency of SSA's policy and procedures for these capability determinations (Medicine & National Academies of Sciences, 2016). As reflected in its report entitled Informing Social Security's Process for Financial Capability Determination, the IOM committee reviewed a broad range of sources, including capability determination processes used by other similar benefit programs, abilities required to manage and direct the management of benefits, and the financial capacity literature and assessment measures, and developed a conceptual model of “financial capability” that informed and guided the committee's thinking and recommendations to SSA. As discussed below, the committee's conceptual model is robust, thoughtful and nuanced, and overall represents an important theoretical advance. The model is also somewhat complex and requires some elucidation to make its premises and definitions clear (see Fig. 1 for a graphical depiction of the IOM model).
Fig. 1.
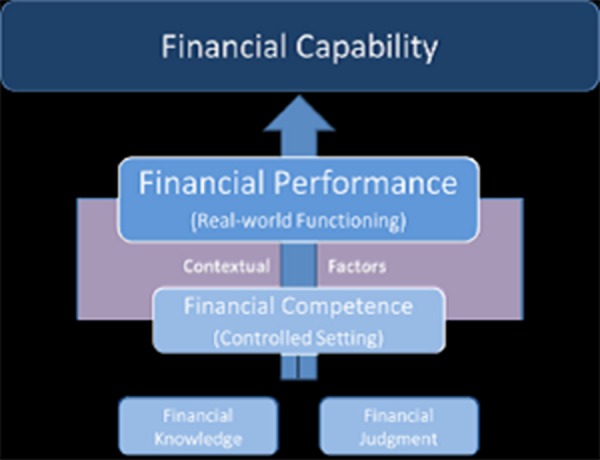
Institute of medicine model of financial capability.
Reprinted with permission from Informing Social Security's process for financial capability determination, 2016 by the National Academies of Sciences, courtesy of the National Academies Press, Washington, D.C.
The guiding premise of the SSA model is that the best measure of a person's financial capacity (“financial capability” in SSA terms) is the person's actual real world financial performance in meeting their basic needs (Medicine & National Academies of Sciences, 2016). Financial performance is thus defined as “an individual's degree of success in handling financial demands in the context of the stresses, supports, contextual cues, and resources in his or her actual environment.” (Medicine & National Academies of Sciences, 2016, p. 5). The concept of the individual's financial context or environment is critical here, as it is the reference point against which the individual person's current financial functioning is measured, as opposed to more generic clinical skills and heuristics. This concept of the individual's specific environment was introduced and emphasized by Grisso in his seminal book on competency assessment, in which he conceptualized competency in terms of the interaction between an individual's environmental demands and his or her specific functional capacity (Grisso, 2003). If evidence of a patient's real world financial performance in meeting basic needs is the best indicator of their financial capacity, how then does a clinician obtain evidence of their real world financial performance? It is at this point that the IOM model becomes conceptually and definitionally complex. The committee expressed the view that financial performance can “best be captured by those professionals and others who have first-hand knowledge of and experience with how an individual functions in his or her environment and who have sufficient opportunities to observe the individual in that environment over an extended period of time.” (Medicine & National Academies of Sciences, 2016, p. 7) However, the committee also realistically noted that informed third party observations of real world financial performance may be difficult to obtain, due to lack of professional training in the assessment of financial capacity, as well as to lack of personal knowledge and also biases that family members and other lay observers may possess. Thus the committee's recommendation concerning relying on informed observers may be more exhortatory at the present time then practical. A key committee recommendation is for SSA to provide detailed guidance to professional and lay informants regarding information needed to make capability determinations and to develop information that would enable SSA to judge the validity of evidence provided by informants.
Another conceptually important aspect of the IOM model was the cautious but pragmatic approach that the committee took with respect to traditional clinical assessments of financial capacity. In distinction to financial performance, the committee defined the term financial competence as “the financial skills one possesses, as demonstrated through financial knowledge and financial judgment, typically assessed in a controlled (e.g., office or other clinical) setting.” (Medicine & National Academies of Sciences, 2016, p. 5). In defining financial competence, the committee acknowledged and incorporated the financial knowledge types of declarative knowledge, procedural knowledge3, and judgment4 proposed by Marson (see Cognitive Psychology model above), and also noted the potential value of existing financial capacity measures for supplying evidence of financial knowledge and judgment. Importantly, the committee was cautious regarding the probative value of such lab and office based clinical data for determinations of financial capability, noting the important interplay of contextual factors:
“An individual may be financially competent in an office or clinical setting but may not exercise his or her financial knowledge and judgment in a real-life setting sufficiently to meet his or her basic needs. Conversely, an individual may fail to demonstrate financial knowledge or judgment in a controlled setting but may perform effectively with assistance of support systems in his or her environment. Because contextual factors can enhance or diminish individuals’ (real-world) financial performance relative to what would be expected based on the financial competence they exhibit in controlled settings, it is important to consider more than financial competence when thinking about financial capability.” (Medicine & National Academies of Sciences, 2016, p. 5).
This statement represents an important conceptual point and caveat concerning traditional clinical assessments of financial capacity. If the clinician obtains the assessment data in a controlled setting (office or clinic)—which is very frequently the case—the evidence of financial knowledge and judgment may not always be fully representative of the patient's actual performance in the real world, and thus must be qualified in terms of its evidentiary value for determining overall “financial capability.”At the same time, the committee recognized that in many cases evidence of financial competence from controlled settings may be the best or even only evidence of financial capability available. Although a real world performance standard is ideal, the problem again is that pragmatically it is and likely will continue to be difficult to obtain accurate reports of real world financial functioning from knowledgeable and unbiased observers. Thus in this writer's judgment, reliance on clinical assessment data from controlled settings will continue to be a vital part of the financial capacity assessment landscape for the foreseeable future.
This criticism notwithstanding, the IOM committee model of financial capability is of substantial conceptual value to the practicing clinician. The model highlights the importance of understanding the patient's real world financial performance, and thus underscores the value of the clinician obtaining (where possible) reports of the patient's actual financial functioning from knowledgeable and unbiased sources. The model also properly emphasizes the importance of understanding the patient's actual financial environment, including the specific “stresses, supports, contextual cues, and resources” that inform and shape the patient's financial actions and behaviors, and his or her everyday financial successes and/or failures. As noted, the model also offers support for use of existing “traditional” financial capacity measures and techniques used in controlled settings, recognizing their value in eliciting objective evidence of the patient's financial knowledge and judgment, while qualifying to some degree their overall probative value as evidence of real world financial function.
General Recommendations for Clinical Assessment of Financial Capacity
The following section of the paper discusses general recommendations for clinical assessment of financial capacity. As will be seen, many of these recommendations are conceptual in nature. In addition, as appropriate the recommendations also seek to reference the conceptual models and principles discussed in the preceding sections of the article.
Identify and clarify the specific referral question(s) relevant to financial capacity
At the outset of a financial capacity evaluation, a clinician should take time to identify and clarify the different capacity issues involved (Marson et al., 2012). In many cases, multiple “financial” capacity issues may be intertwined, and sorting them out ahead of time is essential to conducting an effective evaluation. For example, the clinician should seek to identify how general or narrow the issue may be. For example, is this a matter related to the individual's overall financial capacity and need for a conservatorship, or a more narrow issue of contractual capacity for a specific transaction, or both? In addition, what is the time frame of the issue? Is the referral seeking a prospective evaluation of an individual's current financial capacity, or a retrospective judgment of his or her financial capacity at some earlier point of time? Is there a specific related forensic claim? For example, is the financial capacity issue linked to a related legal claim of undue influence?
At the outset of the evaluation, identify the patient's premorbid level of financial function
It is important for the clinician early on to form a clear picture of the patient's premorbid level of financial functioning (Marson et al., 2012). Prior knowledge of a patient's premorbid financial skills and baseline will inform the kinds of questions and testing that should be pursued in answering the referral questions. For example, if a patient has never managed a checkbook during his or her life, it may not make sense to test the patient's ability to complete a checkbook register, and the clinician cannot persuasively attribute deficits on such a checkbook task to the effects of a neurocognitive disorder. Thus knowledge of a patient's premorbid financial functioning—skills, knowledge, and values—is essential for the clinician to draw meaningful conclusions regarding the patient's current financial capacity and possible deficits or declines in financial skills from a prior baseline.
Despite its methodological importance, the issue of premorbid financial capacity has not received much clinical or research attention, and unfortunately is usually ignored entirely. Traditionally the sources of information regarding premorbid financial function are patient and family report as elicited through clinical interview. There are a few extant structured interview and rating forms that can help organize the receipt of this information (Wadley et al., 2003). In establishing a patient's premorbid financial capacity, the clinician has an opportunity to draw upon and apply one or more of the conceptual models discussed previously. From the standpoint of the clinical model (discussed earlier), the clinician considers the different premorbid financial skills and knowledge types acquired by the patient and the scope of financial activities engaged in. From the standpoint of the decision-making model, the clinician appraises the types of financial decisions and judgment that the patient premorbidly exercised. Finally, assessment of a patient's premorbid financial capacity inherently involves a person-oriented approach where the clinician seeks to identify and understand the patient's premorbid financial skills, knowledge, and values within his/her premorbid financial context.
The clinician should seek to understand the patient's current financial environment and its demands and requirements
As part of conducting a financial capacity evaluation, it is important for the clinician to understand the patient's current financial environment and its demands and requirements. Forming a clear picture of the patient's current financial environment will help the clinician understand what financial skills are critical to the patient maintaining independence in his/her context and community, and what skills may be of secondary or tertiary importance. Like premorbid financial capacity, knowledge of the current financial environment informs the kind of questions and capacity testing that the clinician will pursue in answering the referral questions. And as discussed below, knowledge of the patient's real world financial environment allows the clinician to determine the “goodness of fit” between the patient's current financial skills, knowledge and values, and the demands of that environment, to arrive at a sound financial capacity judgment.
Similar to premorbid financial capacity, in determining a patient's current financial capacity the clinician again has an opportunity to draw upon and apply one or more of the conceptual models discussed previously. From the standpoint of the clinical model, the clinician considers the different financial skills and knowledge types currently possessed by the patient and the scope of financial activities he/she is reportedly currently engaged in. From the standpoint of the decision-making model, the clinician appraises the types of financial decisions and judgment that the patient is currently able to exercise. Finally, assessment of an individual patient's current financial capacity again inherently involves a person-oriented approach where the clinician seeks to identify and understand the patient's current financial skills, knowledge and values within his/her current real world financial environment or context.
In assessing a patient's current financial capacity, the clinician should focus on functional evidence of actual financial skills, knowledge, and values obtained from the patient, family members and other collateral sources, and capacity-specific measures
In assessing a patient's current financial capacity, a clinician should focus on core functional evidence of the patient's actual financial skills, abilities and values, viewed in relation to the current demands of the patient's financial environment (Grisso, 2003). Such core functional evidence is derived from patient, family members and other collateral source report, and from financial capacity specific measures. Accordingly, it is crucial in clinical interview to ask specific questions relevant to the patient's current financial skills, knowledge, and values, and to administer financial capacity measures that also can provide such capacity-specific evidence. As discussed below, general clinical observations, diagnostic assignment, and neuropsychological test findings also have an important role but are secondary forms of evidence for purposes of assessing a patient's financial capacity.
The clinician should analyze the functional evidence of the patient's actual financial skills and knowledge in relation to the demands and requirements of the patient's financial environment. A judgment of financial capacity or incapacity should be based on the relative congruence or incongruence between the patient's actual financial skills, knowledge and values, and the demands and requirements of the patient's financial environment
A clinical judgment of financial capacity involves an analysis and comparison of the patient's actual financial skills and knowledge in relation to the demands and requirements of the patient's financial environment. As suggested by the IOM model, what is the “goodness of fit” between these two bodies of evidence? Does the patient have the financial skills, knowledge, judgment and values to successfully manage his or her financial affairs within their particular financial environment? Or has the patient undergone cognitive decline or behavioral changes that have compromised her financial skills and judgment, and/or her longstanding financial values, such that she can no longer consistently carry out key financial tasks or make decisions in her best interest necessary to live independently in her community? In making a clinical judgment of financial capacity or incapacity, the clinician thus must consider and weigh all the evidence and decide whether the patient's current financial skills, knowledge and values are sufficiently congruent with, or incongruent with, the demands of her real world financial environment.
Cognitive function, diagnosis, and other clinical observations represent a secondary level of clinical evidence in a financial capacity evaluation
Clinicians, in particular neuropsychologists, must be wary of relying on capacity-remote cognitive measures, such as the much vaunted Trails B, as an acceptable proxy for financial capacity-specific information (Marson et al., 2012). Trails B is a measure of executive function that does not convey any capacity-specific information regarding an individual's financial abilities and functioning. It is not an acceptable or sufficient replacement for patient and collateral report and/or direct performance evidence of financial function. Similarly, diagnosis by itself, such as Alzheimer's type dementia, TBI or schizophrenia, cannot itself be dispositive of a question of financial capacity. The specific functional abilities constituent to financial capacity in the individual's personal financial context must be evaluated (Grisso, 2003), and this requires capacity-level information. Put differently, diagnosis and neuropsychological test findings are highly relevant but secondary levels of evidence for purposes of assessing a patient's current financial capacity.
Neuropsychological evidence has substantial value in financial capacity evaluations by providing the clinician with explanatory links between the neurocognitive disorder (or other diagnostic condition) and identified impairments in financial skills and knowledge
Although neuropsychological test results by themselves do not represent capacity findings, they play a very valuable role in capacity evaluations and should be incorporated into such assessments wherever possible (Marson et al., 2012). As noted by Grisso, these clinical test results and observations provide the explanatory links that meaningfully tie a condition such as acute traumatic brain injury to specific impairments in financial skills5 (Grisso, 1986). Thus, an acutely injured patient with moderate or severe TBI, involving intraparenchymal hemorrhage and frontal contusions, may demonstrate a neurocognitive profile reflecting characteristic impairments in attention, short-term memory, and executive function. These cognitive deficits can then be meaningfully related to corresponding deficits in the TBI patient's financial knowledge, performance, and judgment skills, as elicited through financial capacity questions and measures. In conjunction with other evidence, specific neurocognitive deficits also raise persuasive inferences that certain financial skills, such as awareness of fraud risk or complex financial decision making, were likely impaired at critical points in a disease process.
Summary
The ability to manage one's financial affairs is an everyday life skill of critical importance, and neuropsychologists are increasingly called upon to assess financial capacity across a variety of settings. Sound clinical and forensic assessment of financial capacity requires an understanding and appreciation of applicable clinical conceptual models of the capacity. Yet despite its importance, there is relatively little conceptual guidance available for clinicians concerning financial capacity and its assessment in clinical and forensic settings. This article has sought to assemble and present available conceptual work on financial capacity relevant to clinicians assessing financial capacity in everyday practice. The article presented six clinical models of financial capacity, beginning with (1) the early gerontological IADL model of Lawton and Brodie, and followed by (2) the UAB clinical skills model developed by Marson and colleagues, (3) a related cognitive psychological model also offered by Marson and colleagues, (4) a financial decision-making model adapting the earlier decisional capacity work of Appelbaum and Grisso, (5) a recent person-centered model of financial decision-making developed by Lichtenberg and colleagues, and (6) a recent and theoretically rigorous and thought provoking model developed through a committee constituted by the IOM and National Academy of Sciences Presentation of these models has included specific discussion of the different and evolving conceptual and practical perspectives they represent for clinician assessment in both older adult and younger adult populations.
Finally, building upon this conceptual discussion, we have also presented a series of conceptually oriented guidelines for clinical assessment of financial capacity that draw upon the different conceptual models and their underlying principles. It is the author's hope that the presentation and discussion of these conceptual models, principles and guidelines will strengthen and advance clinical assessment of financial capacity.
Funding
This work was supported by the National Institute on Aging (5R01 AG021927) (Dr. Marson, PI).
Conflict of Interest
None declared.
Footnotes
Searches included PubMed and Google and two law databases, LegalTrac and Academic Search Premier, accessed via Mervyn Sterne Library at University of Alabama at Birmingham. Keywords used in the search were financial capacity, money management, elderly, aged, older adult, elder and geriatric within the time period January 1, 1970 to December 31, 1999.
The bracketed level numbers and functional descriptors have been added by the author.
The committee defined financial knowledge as “the possession of the declarative knowledge (i.e., information that a person knows) and procedural knowledge (i.e., knowing how to perform a task) required to manage one's finances (e.g., the concept of money, values of currency, making change, check writing, use of automatic teller machines, and online banking procedures).” (Medicine & National Academies of Sciences, 2016, p. 5).
The committee defined financial judgment as “the possession of the abilities (understanding, reasoning, and appreciation) needed to make financial decisions and choices that serve the individual's best interests.” (Medicine & National Academies of Sciences, 2016, p. 5).
As noted by Grisso in the forensic context, decision makers must go further and “present the logic that links these clinical observations [i.e., test results] to the capacities with which the law is concerned”(Grisso, 1986, p. 8). See also Marson, Martin, Triebel, & Nabors, 2010 and Marson, Hebert, & Solomon, 2011).
References
- Anderson J. R. (1976). Language, memory, and thought. Hillsdale, New Jersey: Lawrence Erlbaum Associates. [Google Scholar]
- Appelbaum P., & Grisso T. (1988). Assessing patients’ capacities to consent to treatment. New England Journal of Medicine, 319, 1635–1638. [DOI] [PubMed] [Google Scholar]
- Connolly M. T. (Producer). (April 28, 2015). Elder justice and dementia panel. Advisory Council on Alzheimer's Research, Care, and Services Meetings.
- Dreer L. E., Devivo M. J., Novack T., & Marson D. C. (2012). Financial capacity following traumatic brain injury (TBI): A six-month longitudinal study. Rehabiliation Psychology, 57 (1), 5–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazio S. (2013). The individual is the core-and the key-to person centered care. Generations, 37 (3), 16–22. [Google Scholar]
- Gerstenecker A., Eakin A., Triebel K., Martin R., Swenson-Dravis D., & Petersen R. C., et al. (2015). Age and education corrected older adult normative data for a short form version of the financial capacity instrument. Psychological Assessment, 28, 737–749. doi:10.1037/pas0000159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffith H. R., Belue K., Sicola A., Krzywanski S., Zamrini E., & Harrell L., et al. (2003). Impaired financial abilities in mild cognitive impairment: A direct assessment approach. Neurology, 60 (3), 449–457. [DOI] [PubMed] [Google Scholar]
- Grisso T. (1986). Evaluating competencies: Forensic assessments and instruments. New York: Plenum Press. [Google Scholar]
- Grisso T. (2003). Evaluating competencies: Forensic assessments and instruments (2nd ed.). New York: Kluwer Academic. [Google Scholar]
- Grisso T., & Appelbaum P. (1998). Assessing competence to consent to treatment: A guide for physicians and other health professionals. New York: Oxford University. [Google Scholar]
- Karlawish J., & Lai J. (2008). Manual for the Assessment of Capacity for Everyday Decision-Making (ACED).
- Kershaw M. M., & Webber L. S. (2008). Assessment of financial competence. Psychiatry, Psychology and Law, 15 (1), 40–55. [Google Scholar]
- Lai J. M., Gill T. M., Cooney L. M., Bradley E. H., Hawkins K. A., & Karlawish J. H. (2008). Everyday decision-making ability in older persons with cognitive impairment. American Journal of Geriatric Psychiatry, 16 (8), 693–696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawton M., & Brody E. (1969). Assessment of older people: Self-maintaining and instrumental activities of daily living. The Gerontologist, 9, 179–185. [PubMed] [Google Scholar]
- Lichtenberg P. A., Stoltman J., Ficker L. J., Iris M., & Mast B. (2015). A person-centered approach to financial capacity assessment: Preliminary development of a new rating scale. Clinical Gerontologist, 38 (1), 49–67. doi:10.1080/07317115.2014.970318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loeb P. (1996). Independent living scales manual. San Antonio: The Psychological Corporation. [Google Scholar]
- Loewenstein D. A., Amigo E., Duara R., Guterman A., Hurwitz D., & Berkowitz N., et al. (1989). A new scale for the assessment of functional status in Alzheimer's disease and related disorders. Journal of Gerontology, 44 (4), P114–121. [DOI] [PubMed] [Google Scholar]
- Marson D. C. (2001). Loss of financial capacity in dementia: Conceptual and empirical approaches. Aging, Neuropsychology and Cognition, 8, 164–181. [Google Scholar]
- Marson D. C. (2013). Clinical and ethical aspects of financial capacity in dementia: a commentary. American Journal of Geriatric Psychiatry, 21 (4), 382–390. doi:10.1016/j.jagp.2013.01.033. [DOI] [PubMed] [Google Scholar]
- Marson D. C., & Hebert K. (2008). Financial capacity. In Cutler B. L. (Ed.) Encyclopedia of psychology and the law (Vol. 1, pp. 313–316). California: Sage. [Google Scholar]
- Marson D. C., Hebert K., & Solomon A. (2011). Assessing civil competencies in older adults with dementia: Consent capacity, financial capacity, and testamentary capacity In G. J. Larrabee. (Ed.), Forensic neuropsychology: A scientific approach (2nd ed., pp. 401–437). New York: Oxford University. [Google Scholar]
- Marson D. C., & Hebert K. R. (2005). Functional assessment in geriatric neuropsychology In D. Attix & K. A. Welsh-Bohmer (Eds.), Geriatric neuropsychology assessment and Intervention, (pp. 158–197). New York: Guilford. [Google Scholar]
- Marson D. C., Martin R. C., Triebel K. L., & Nabors L. B. (2010). Capacity to consent to research participation in adults with malignant glioma. Journal of Clinical Oncology, 28 (24), 3844–3850. doi:10.1200/JCO.2009.27.9091. [DOI] [PubMed] [Google Scholar]
- Marson D. C., Martin R. C., Wadley V., Griffith H. R., Snyder S., & Goode P. S., et al. (2009). Clinical interview assessment of financial capacity in older adults with mild cognitive impairment and Alzheimer's disease. Journal of the American Geriatrics Society, 57 (5), 806–814. doi:10.1111/j.1532-5415.2009.02202.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marson D. C., Sawrie S. M., Snyder S., McInturff B., Stalvey T., & Boothe A., et al. (2000). Assessing financial capacity in patients with Alzheimer disease: A conceptual model and prototype instrument. Archives of Neurology, 57, 877–884. [DOI] [PubMed] [Google Scholar]
- Marson D. C., Schmitt F. A., Ingram K. K., & Harrell L. E. (1994). Determining the competency of Alzheimer patients to consent to treatment and research. Alzheimer Disease & Associated Disorders, 8 (Suppl. 4), 5–18. [PubMed] [Google Scholar]
- Marson D. C., Triebel K., Gerstenecker A., Martin R., Edwards K., Pankratz V. S., et al. (2014). Detecting declining financial skills in preclinical Alzheimer's disease. The Financial Capacity Instrument-Short Form. – Poster presentation 10th annual conference of the international society for CNS clinical trials and methodology. Boston, Massachusetts.
- Marson D. C., Triebel K. L., Knight A. J. (2012). Assessment of financial capacity: A neuropsychological perspective In G. J. Demakis. (Ed.), Civil capacities in clinical neuropsychology, (pp. 39–68). New York: Oxford University. [Google Scholar]
- Martin R., Griffith H. R., Belue K., Harrell L., Zamrini E., & Anderson B., et al. (2008). Declining financial capacity in patients with mild Alzheimer disease: A one-year longitudinal study. American Journal of Geriatric Psychiatry, 16 (3), 209–219. [DOI] [PubMed] [Google Scholar]
- Martin R. C., Triebel K. L., Kennedy R. E., Nicholas A. P., Watts R. L., & Stover N. P., et al. (2013). Impaired financial abilities in Parkinson's disease patients with mild cognitive impairment and dementia. Parkinsonism & Related Disorders, 19 (11), 986–990. doi:10.1016/j.parkreldis.2013.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mast B. (2011). Whole person dementia assessment. Baltimore MD: Health Professions Press. [Google Scholar]
- Medicine & National Academies of Sciences, E (2016). In Appelbaum P. S., Spicer C. M., & Valliere F. R. (Eds.), Informing Social security's process for financial capability determination. Washington, D.C.: The National Academies Press. [PubMed] [Google Scholar]
- Moye J., & Marson D. C. (2007). Assessment of decision-making capacity in older adults: An emerging area of practice and research. Journal of Gerontology B Psychological Sciences & Social Sciences, 62 (1), P3–P11. [DOI] [PubMed] [Google Scholar]
- Patterson T., Goldman S., McKibbon C., Hughes T., & Jeste D. (2001). UCSD performance-based skills assessment: Development of a new measure of everyday functioning for severely mentally ill adults. Schizophrenia Bulletin, 27 (2), 235–245. [DOI] [PubMed] [Google Scholar]
- Pinsker D. M., Pachana N. A., Wilson J., Tilse C., & Byrne G. J. (2010). Financial capacity in older adults: A review of clinical assessment approaches and considerations. Clinical Gerontologist, 33, 332–346. [Google Scholar]
- Roth L., Meisel A., & Lidz C. (1977). Tests of competency to consent to treatment. American Journal of Psychiatry, 134 (3), 279–284. [DOI] [PubMed] [Google Scholar]
- Stadler M. A. (1989). On learning complex procedural knowledge. Journal of Experimental Psychology: Learning, Memory, and Cognition, 15 (6), 1061–1069. [DOI] [PubMed] [Google Scholar]
- Stillings N. A., Weisler S. E., Chase C. H., Feinstein M. H., Garfield J. L., & Rissland E. L. (1995). Cognitive science: An introduction (2nd ed.). Cambridge, Massachuetts: The MIT Press. [Google Scholar]
- Triebel K. L., Okonkwo O. C., Martin R., Griffith H. R., Crowther M., & Marson D. C. (2010). Financial capacity of older African Americans with amnestic mild cognitive impairment. Alzheimer Disease & Associated Disorders, 24 (4), 365–371. doi:10.1097/WAD.0b013e3181e7cb05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wadley V. G., Harrell L. E., & Marson D. C. (2003). Self- and informant report of financial abilities in patients with Alzheimer's disease: Reliable and valid?. Journal of the American Geriatric Society, 51 (11), 1621–1626. [DOI] [PubMed] [Google Scholar]
- Widera E., Steenpass V., Marson D., & Sudore R. (2011). Finances in the older patient with cognitive impairment. Journal of the American Medical Associaton, 305 (7), 698–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu F. O. T., Lui V. W. C., Lam L. C. W., Chiu H. F. K., Karlawish J. H. T., & Appelbaum P. S. (2009). Assessment of capacity to make financial decision in Chinese psychogeratric Patients: A pilot study. Hong Kong Journal of Psychiatry, 19 (2), 82. [Google Scholar]