

Abstract
Background:
Bronchial artery aneurysm (BAA) is an uncommon but potentially life-threatening disease, and multiple BAAs are even rarer. Clinically, the tortuous and short neck of a BAA may present significant challenges for invasive intervention.
Methods:
This report describes the detailed process of diagnosis and treatment and includes a literature review of the etiology, clinical presentation, and therapeutic management of BAA.
Results:
A rare case of multiple BAAs, with one having an inflow artery arising from the brachiocephalic trunk, was referred to our hospital. The patient was successfully treated with coil embolization and brachiocephalic artery stent placement. In addition, we conducted a literature review involving 63 cases of BAA. BAA was most commonly associated with bronchiectasis and was located predominantly in the mediastinum. There was no significant difference between the diameters of the ruptured aneurysms and those of the nonruptured aneurysms (P = 0.115). Transcatheter arterial embolization was the most commonly adopted technique to treat BAA, while thoracic aortic endovascular repair was selected if the neck between the aneurysm and the aorta was short. Subgroup analysis suggested that patients with > 1 BAA were significantly more likely to be female than male (χ2 test, P = 0.034).
Conclusion:
Transcatheter coil embolization combined with stent placement could be a reasonable treatment option for BAAs with a tortuous and short neck. According to our literature review, patients with multiple BAAs display distinctive clinical characteristics compared with patients with a single BAA.
Keywords: brachiocephalic artery stent, brachiocephalic trunk, bronchial artery aneurysm, coil embolization
1. Introduction
Bronchial artery aneurysm (BAA) is a rare but potentially deadly disease, reportedly accounting for <1% of all aneurysms, revealed by selective bronchial arteriography.[1] Patients with multiple BAAs are even more rarely seen. Here, we report a case of multiple BAAs arising from an ectopic bronchial artery. The patient was successfully treated with coil embolization combined with stent placement. The etiology, clinical manifestations, and therapeutic treatment of BAA are herein discussed, with reference to 63 cases reported previously.
2. Consent
This study adhered to the tenets of the Declaration of Helsinki. Informed consent was signed by the patient for publication of this report and its related images.
3. Case presentation
A 50-year-old female with chronic chest pain radiating to her back was referred to our hospital for further examination. She had been treated for hypertension for 7 years with felodipine (Plendil; 5 mg daily). The patient was normal on physical examination. Her laboratory results were generally nonsignificant, except mildly elevated high-sensitivity C-reactive protein 9.36 mg/L, gamma-glutamyl transferase 83 U/L, aspartate aminotransferase 38 U/L, and erythrocyte sedimentation rate 25 mm/h.
A contrast-enhanced computed tomography (CT) scan revealed multiple aneurysms with the largest lesion adjacent to the brachiocephalic artery. By carefully studying a 3-dimensional reconstruction of a CT scan, we found 3 aneurysms, 2 of which were bronchial artery aneurysms, and one was in the phrenic artery. The largest one, 2.5 × 2.2 cm, was located in the mediastinum and was fed by an abnormal bronchial artery branching from the brachiocephalic trunk (Fig. 1); the other 2 were inside the right lung, with 1 (1.0 × 0.9 cm) fed by right bronchial artery and 1 (1.1 × 1.1 cm) fed by phrenic artery. Enlargement of the right bronchial and phrenic artery were also observed (Fig. 2).
Figure 1.
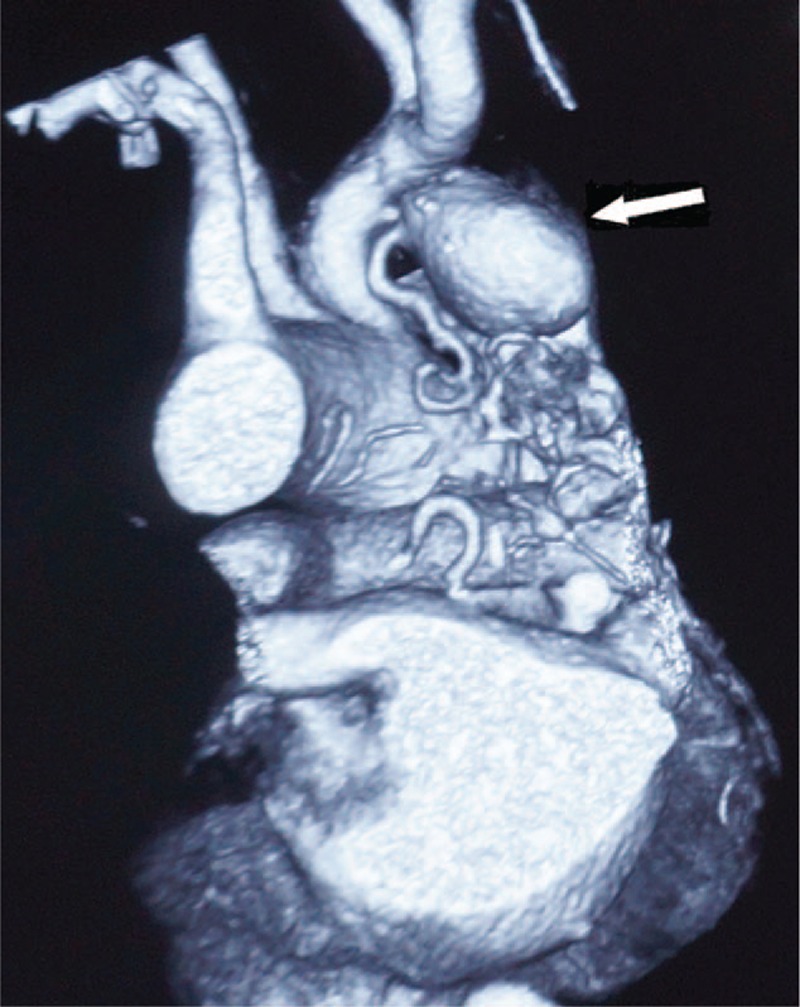
Three-dimensional reconstruction of contrast-enhanced computed tomography scan. The white arrow indicates the bronchial artery aneurysm adjacent to the brachiocephalic trunk. Note the ectopic bronchial artery branching from the brachiocephalic trunk and the extremely short neck of the aneurysm.
Figure 2.
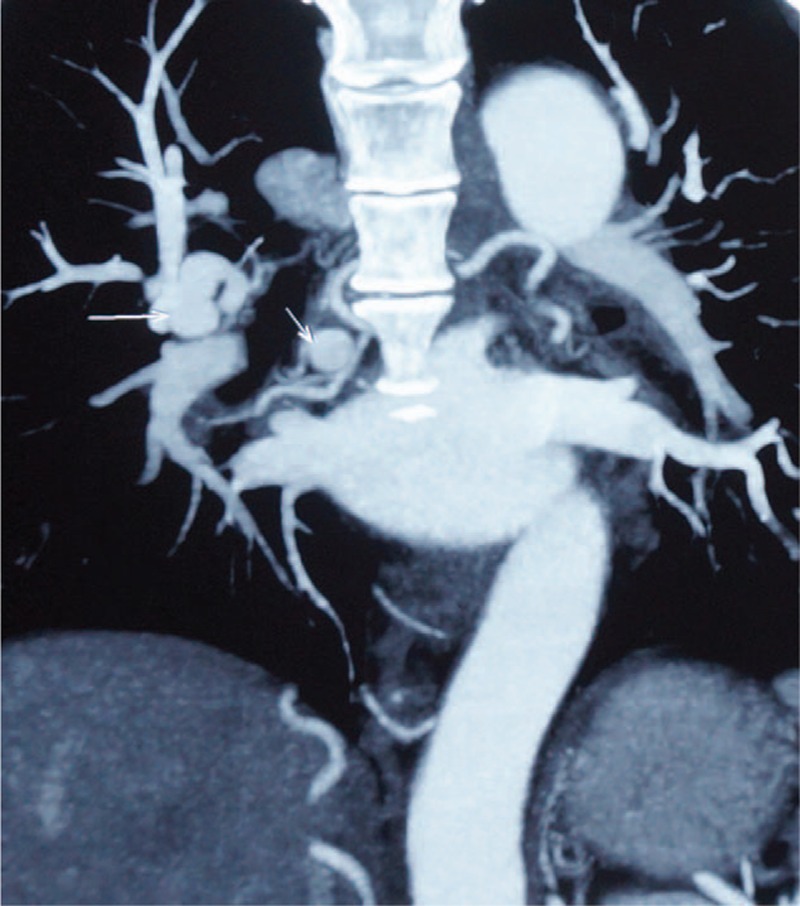
Coronary reconstruction of contrast-enhanced computed tomography scan. The 2 small white arrows from left to right show the other bronchial aneurysm and phrenic artery aneurysm, respectively.
We decided to treat only the ectopic bronchial artery aneurysm localized in the mediastinum via an endovascular approach. Considering the short neck of the aneurysm, we combined transcatheter arterial embolization with stent placement. Following aortic arch aortography via a femoral approach (Fig. 3A), a selective brachiocephalic arteriography demonstrated the ectopic BAA arising from 1 abnormal branch of brachiocephalic trunk (Fig. 3B). We managed to advance into the outflow artery and released several interlocking coils (Cook Medical, Bloomington, IN) into the outflow artery, the aneurysm sac, and then the inflow artery. A bare-metal stent (Cordis, 12–40 mm) was then successfully deployed across the origin of the abnormal bronchial artery at the brachiocephalic trunk. Owing to the length of the brachiocephalic trunk, the origin of the right subclavian artery was covered.
Figure 3.

Images of aneurysm. (A) Aortic arch aortography in a frontal view. This angiogram shows an aneurysm adjacent to the brachiocephalic trunk. (B) Selective brachiocephalic arteriogrphy before embolization. The aneurysm was fed by an abnormal bronchial artery branching from the brachiocephalic trunk. (C) Postprocedure angiogram in a frontal view. The ectopic bronchial aneurysm had been successfully embolized by interlocking coils. The right common carotid artery and subclavian artery were patent.
A postprocedural angiogram confirmed embolization of the aneurysm and patent right common carotid and subclavian arteries (Fig. 3C). The postoperation CT angiogram was satisfactory, with thrombosis formed in the aneurysm sac (Fig. 4).
Figure 4.
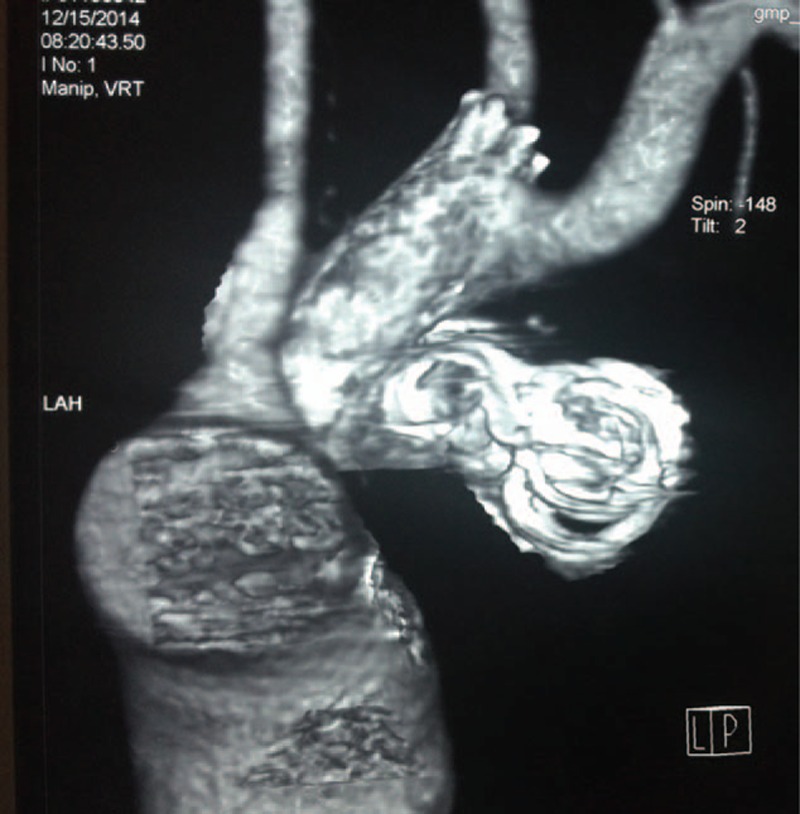
Three-dimensional reconstruction of contrast-enhanced computed tomography scan 1 week after operation. The aneurysm was successfully embolized by interlocking coils. The brachiocephalic trunk was patent and protected by a bare metal stent.
The patient returned 4 months after the procedure. The CT angiogram showed a patent right subclavian artery, and the completely thrombosed aneurysm (Fig. 5).
Figure 5.

Coronary reconstruction of contrast-enhanced computed tomography scan 4 months after operation. The brachiocephalic trunk and right subclavian artery were patent and the aneurysm remained thrombosed.
4. Discussion
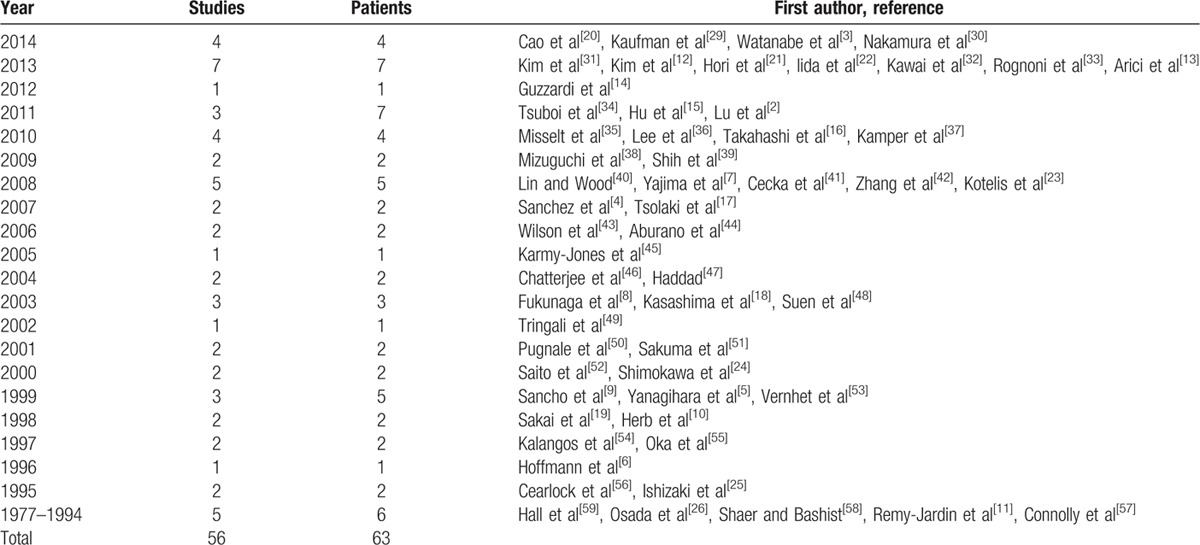
BAA occurs rarely. We searched the PubMed database with the search term “bronchial artery aneurysm” and found 56 articles with relevant data for 63 cases (Table 1). We reviewed these cases to enhance our understanding of the etiology, clinical presentations, and therapeutic management of BAA.
Table 1.
Review of 56 articles involving 63 cases of bronchial artery aneurysms.
The etiology of BAA is poorly understood. It has been suggested that both increased bronchial arterial flow and focal weakening of the vessel wall contribute to the pathogenesis of BAA.[2] Our analysis of the relevant literature revealed that BAA was most commonly associated with bronchiectasis (Fig. 6), with other factors being hypertension, chronic obstructive pulmonary disease vasculitis, chronic bronchopulmonary infection, tuberculosis, and trauma. However, many patients with BAA had a clean medical history.
Figure 6.
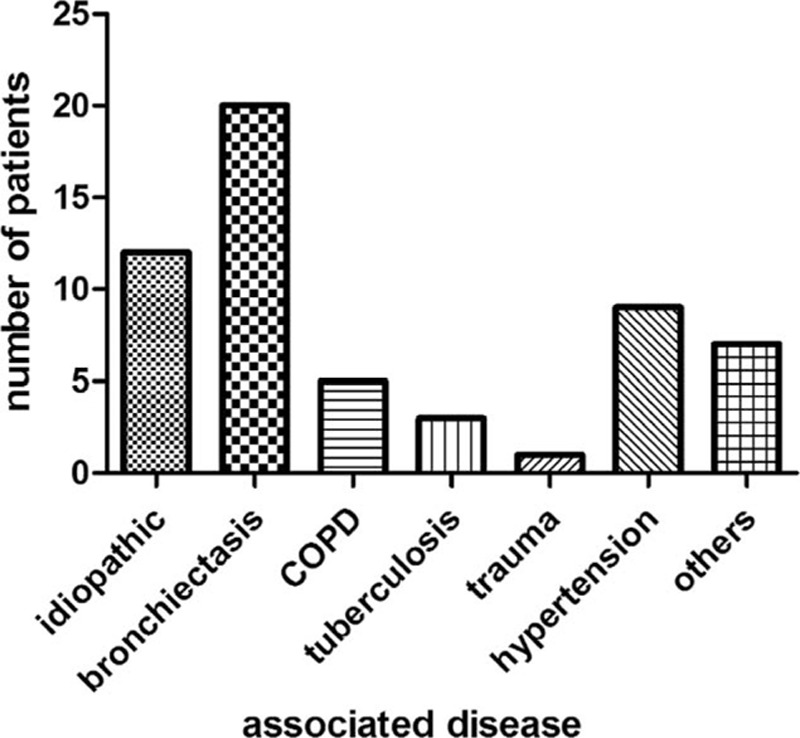
Common associated diseases of bronchial artery aneurysm. COPD = chronic obstructive pulmonary disease, No = no associated disease identified.
The clinical manifestations of BAA vary and depend on where the aneurysm is located and whether the aneurysm has ruptured. For patients who had a ruptured aneurysm, the most common symptom was chest pain, and then hemoptysis, back pain, epigastric pain, and symptoms related to shock. For patients with intact aneurysms, the BAA was usually identified incidentally upon thoracic scanning.
Other BAA-related symptoms included hemoptysis, dysphagia, chest pain, cough, hoarseness, dyspnea, pneumonia, and fever. There was no significant difference between the diameters of the ruptured aneurysms (mean 2.93 cm) and those of the nonruptured aneurysms (mean 2.18 cm; P = 0.115). Therefore, there may be no correlation between size of the aneurysm and the likelihood of rupture.
Our review of the literature also showed that most aneurysms (83.3%, 45/54) were located in the mediastinum, with either the left (20/50) or right (26/50) bronchial artery as the feeding artery. In addition, aneurysms arising from both bronchial arteries were observed (8.0%, 4/50), but intrapulmonary aneurysm of the left side was rarely encountered (3.7%, 2/54).
Because rupture can threaten life, BAA should be treated immediately after the diagnosis is established. With the improvement of endovascular technique, less invasive approaches are more commonly applied as initial treatments. These include transcatheter arterial embolization (TAE) of the bronchial artery, and occasionally thoracic aortic endovascular repair.
According to the literature, TAE was performed on 46 patients diagnosed with BAA. Among these cases, 5 procedures were unsuccessful and were succeeded immediately with surgical intervention or a second TAE.[3–6] After temporal success in another 5 patients, refilling of the aneurysm on follow-up imaging and recurrence of symptoms was documented.[7–11] The reasons for failure of a TAE were complicated, but may be related to the greatly enlarged bronchial artery and revascularization by collateral arteries.
One of the challenging problems in treating some BAAs was the short neck between the aneurysm and aorta—in our case, between the aneurysm and the brachiocephalic trunk. Thoracic aortic endovascular repair was selected to solve the short neck issue, as reported in 9 articles.[4,12–19] In our case, we chose to implant a stent across the ectopic bronchial artery to avoid movement of the interlocking coils. To our best knowledge, this is the first time that combined TAE and stent was used in treating BAA. Long-term follow-up data are still needed, as thoracic aortic endovascular repair was reported to fail eventually.[17]
In addition, we conducted a subgroup investigation of patients with multiple BAAs, for which only 12 cases were available in the literature.[3,10,17,20–28] These patients were slightly younger (mean age, 50.7 years) than cases of single BAA reported in the literature (mean age, 59.3 years). We also observed that patients with >1 BAA were significantly more likely to be female (80%) than male (χ2 test, P = 0.034). Also, aneurysms arising from the right bronchial artery were seen in 6 of 8 patients. There was no significant difference between multiple BBAs and single BBA (χ2 test, P = 0.246). In terms of etiology, 4 patients were associated with bronchiectasis, Hughes-Stovin syndrome, tuberculosis, and silicosis, respectively, whereas others were idiopathic. These findings suggest that the mechanism(s) underlying the development of multiple BAAs may be distinct from that of a single BAA.
5. Conclusion
BAA is a potentially life-threatening lesion that requires prompt treatment, regardless of its diameter or patient symptoms. With the improvement of endovascular technology, TAE has become the major treatment for BAA. However, the tortuous and short neck of the BAA may still present significant challenges for clinical intervention. Long-term follow-up studies are needed. In addition, patients with multiple BAAs display distinctive patterns and need further clinical investigations.
Footnotes
Abbreviations: BAA = bronchial artery aneurysm, CT = computed tomography, TAE = transcatheter arterial embolization.
XD and D-HJ contributed equally to this work.
The authors report no conflicts of interest.
References
- 1.Fujita J, Akashi K, Kunikane H, et al. A case of bronchial artery aneurysm demonstrating a mass shadow on chest X-ray film. Nihon Kyobu Shikkan Gakkai Zasshi 1991; 29:1591–1595. [PubMed] [Google Scholar]
- 2.Lu PH, Wang LF, Su YS, et al. Endovascular therapy of bronchial artery aneurysm: five cases with six aneurysms. Cardiovasc Intervent Radiol 2011; 34:508–512. [DOI] [PubMed] [Google Scholar]
- 3.Watanabe H, Numata T, Yanai H, et al. Bronchial artery aneurysm diagnosed on 3D-CT. Intern Med 2014; 53:1451–1452. [DOI] [PubMed] [Google Scholar]
- 4.Sanchez E, Alados P, Zurera L, et al. Bronchial artery aneurysm treated with aortic stent graft and fibrin sealant. Ann Thorac Surg 2007; 83:693–695. [DOI] [PubMed] [Google Scholar]
- 5.Yanagihara K, Ueno Y, Kobayashi T, et al. Bronchial artery aneurysm. Ann Thorac Surg 1999; 67:854–855. [DOI] [PubMed] [Google Scholar]
- 6.Hoffmann V, Ysebaert D, De Schepper A, et al. Acute superior vena cava obstruction after rupture of a bronchial artery aneurysm. Chest 1996; 110:1356–1358. [DOI] [PubMed] [Google Scholar]
- 7.Yajima N, Tsutsui H, Yoshioka T, et al. Gigantic bronchial artery aneurysm treated with transcatheter arterial embolization: a case report. Angiology 2008; 59:757–760. [DOI] [PubMed] [Google Scholar]
- 8.Fukunaga A, Okushiba S, Ohno K, et al. Mediastinal bronchial artery aneurysm with hematemesis. Dis Esophagus 2003; 16:328–331. [DOI] [PubMed] [Google Scholar]
- 9.Sancho C, Dominguez J, Escalante E, et al. Embolization of an anomalous bronchial artery aneurysm in a patient with agenesis of the left pulmonary artery. J Vasc Interv Radiol 1999; 10:1122–1126. [DOI] [PubMed] [Google Scholar]
- 10.Herb S, Hetzel M, Hetzel J, et al. An unusual case of Hughes-Stovin syndrome. Eur Respir J 1998; 11:1191–1193. [DOI] [PubMed] [Google Scholar]
- 11.Remy-Jardin M, Remy J, Ramon P, et al. Mediastinal bronchial artery aneurysm: dynamic computed tomography appearance. Cardiovasc Intervent Radiol 1991; 14:118–120. [DOI] [PubMed] [Google Scholar]
- 12.Kim YK, Sung YM, Kim JH, et al. Aortic stent-graft for a giant bronchial artery aneurysm with ultrashort neck. Ann Thorac Cardiovasc Surg 2014; 20 (Suppl):781–785. [DOI] [PubMed] [Google Scholar]
- 13.Arici V, Bozzani A, Odero A. Successful endovascular treatment of a bronchial artery aneurysm refractory to transcatheter embolization. Ann Vasc Surg 2013; 27:802.e813–805.e813. [DOI] [PubMed] [Google Scholar]
- 14.Guzzardi G, Cerini P, Fossaceca R, et al. Endovascular treatment of bronchial artery aneurysm with aortic stent-graft placement and coil embolization. Ann Vasc Surg 2012; 26:1013.e1015–1018.e1015. [DOI] [PubMed] [Google Scholar]
- 15.Hu CX, Huang S, Xu ZW, et al. Combination of aortic stent-graft and arterial embolization for ruptured bronchial artery aneurysm. Ann Thorac Surg 2011; 92:e19–e21. [DOI] [PubMed] [Google Scholar]
- 16.Takahashi Y, Tsutsumi Y, Monta O, et al. Stent grafting for giant bronchial artery aneurysm disguised as an aneurysm with multiple feeding arteries. Ann Thorac Surg 2010; 89:1652–1654. [DOI] [PubMed] [Google Scholar]
- 17.Tsolaki E, Salviato E, Coen M, et al. Double right bronchial artery aneurysm treated with combined procedures. Eur J Vasc Endovasc Surg 2007; 34:537–539. [DOI] [PubMed] [Google Scholar]
- 18.Kasashima F, Endo M, Kosugi I, et al. Mediastinal bronchial artery aneurysm treated with a stent-graft. J Endovasc Ther 2003; 10:381–385. [DOI] [PubMed] [Google Scholar]
- 19.Sakai T, Razavi MK, Semba CP, et al. Percutaneous treatment of bronchial artery aneurysm with use of transcatheter coil embolization and thoracic aortic stent-graft placement. J Vasc Interv Radiol 1998; 9:1025–1028. [DOI] [PubMed] [Google Scholar]
- 20.Cao X, He H, Li X, et al. Extracorporeal membrane oxygenation as a platform for the management of massive hemoptysis caused by bronchial artery aneurysm. Chin Med J (Engl) 2014; 127:3032. [PubMed] [Google Scholar]
- 21.Hori D, Noguchi K, Nomura Y, et al. Successful endovascular treatment of ruptured bronchial artery aneurysm. Asian Cardiovasc Thorac Ann 2013; 21:615–617. [DOI] [PubMed] [Google Scholar]
- 22.Iida Y, Saguchi T, Ikeda N, et al. Bronchial artery aneurysm. J Vasc Surg 2013; 58:217. [DOI] [PubMed] [Google Scholar]
- 23.Kotelis D, Allenberg JR, Richter G, et al. Images in vascular medicine. Multiple arterial aneurysms in the mediastinum. Vasc Med 2008; 13:173–174. [DOI] [PubMed] [Google Scholar]
- 24.Shimokawa S, Ishizaki N, Watanabe S. Ruptured bronchial artery aneurysm. Ann Thorac Surg 2000; 69:1641–1642. [DOI] [PubMed] [Google Scholar]
- 25.Ishizaki N, Shimokawa S, Tanaka K, et al. Ruptured bronchial artery aneurysm associated with pleural telangiectasis and tortuous portal obstruction: report of a case. Surg Today 1995; 25:852–854. [DOI] [PubMed] [Google Scholar]
- 26.Osada H, Kawada T, Ashida H, et al. Bronchial artery aneurysm. Ann Thorac Surg 1986; 41:440–442. [DOI] [PubMed] [Google Scholar]
- 27.Siegler CM, Mason AC, Clouston JC. Bronchial artery aneurysms in association with Mycobacterium avium intracellulare complex. J Thorac Imaging 1996; 11:155–157. [DOI] [PubMed] [Google Scholar]
- 28.Giron J, Assoun J, Cholot M, et al. Multiple bronchial artery aneurysms in a patient with silicosis. Rev Mal Respir 1995; 12:311–313. [PubMed] [Google Scholar]
- 29.Kaufman C, Kabutey NK, Sgroi M, et al. Bronchial artery pseudoaneurysm with symptomatic mediastinal hematoma. Clin Imaging 2014; 38:536–539. [DOI] [PubMed] [Google Scholar]
- 30.Nakamura R, Inage Y, Tsuchiya A, et al. Bronchial artery aneurysm treated with video-assisted thoracoscopic surgery. Ann Vasc Surg 2014; 28:1321.e1321–1323.e1321. [DOI] [PubMed] [Google Scholar]
- 31.Kim HJ, Son HS, Cho SB, et al. Development of a life-threatening mediastinal hematoma from a ruptured bronchial artery aneurysm. J Thorac Cardiovasc Surg 2013; 146:e47–e49. [DOI] [PubMed] [Google Scholar]
- 32.Kawai N, Sato M, Minamiguchi H. Bronchial artery aneurysm and pulmonary arteriovenous malformation. J Vasc Interv Radiol 2013; 24:47. [DOI] [PubMed] [Google Scholar]
- 33.Rognoni A, Lupi A, Rosso R, et al. Giant bronchial artery aneurysm treated by coil embolization and Amplatzer placement. J Cardiovasc Med (Hagerstown) 2015; 16 suppl 1:S66–S67. [DOI] [PubMed] [Google Scholar]
- 34.Tsuboi R, Oki M, Saka H. Mediastinal bronchial artery aneurysm mimicking a subcarinal tumor. Respiration 2011; 82:207–208. [DOI] [PubMed] [Google Scholar]
- 35.Misselt AJ, Krowka MJ, Misra S. Successful coil embolization of mediastinal bronchial artery aneurysm. J Vasc Interv Radiol 2010; 21:295–296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lee YJ, Park SS, Kim SY, et al. A case of systemic polyarteritis nodosa involving bronchial artery. Sarcoidosis Vasc Diffuse Lung Dis 2010; 27:164–168. [PubMed] [Google Scholar]
- 37.Kamper L, Smettan J, Abanador-Kamper N, et al. Multimodal visualization of a retrocardial bronchial artery aneurysm with rare origin from the distal descending aorta. Clin Res Cardiol 2010; 99:51–52. [DOI] [PubMed] [Google Scholar]
- 38.Mizuguchi S, Inoue K, Kida A, et al. Ruptured bronchial artery aneurysm associated with bronchiectasis: a case report. Ann Thorac Cardiovasc Surg 2009; 15:115–118. [PubMed] [Google Scholar]
- 39.Shih SY, Hu SY, Tsan YT, et al. Spontaneous hemomediastinum and hemothorax caused by ruptured bronchial artery aneurysm. Eur J Cardiothorac Surg 2009; 35:1076. [DOI] [PubMed] [Google Scholar]
- 40.Lin J, Wood DE. Bronchial artery aneurysm refractory to transcatheter embolization. Ann Thorac Surg 2008; 86:306–308. [DOI] [PubMed] [Google Scholar]
- 41.Cecka F, Raupach J, Hoffmann P, et al. Ruptured bronchial artery aneurysm: case report. Acta Medica (Hradec Kralove) 2008; 51:241–243. [PubMed] [Google Scholar]
- 42.Zhang LJ, Yang GF, Lu GM. Noninvasive diagnosis of bronchial artery aneurysm using dual-source computed tomography angiography. Acta Radiol 2008; 49:291–294. [DOI] [PubMed] [Google Scholar]
- 43.Wilson SR, Winger DI, Katz DS. CT visualization of mediastinal bronchial artery aneurysm. AJR Am J Roentgenol 2006; 187:W544–W545. [DOI] [PubMed] [Google Scholar]
- 44.Aburano H, Kawamori Y, Horiti Y, et al. Bronchial artery aneurysm embolization with NBCA. Cardiovasc Intervent Radiol 2006; 29:1141–1143. [DOI] [PubMed] [Google Scholar]
- 45.Karmy-Jones R, Hastreiter D, Burdick T. Hemothorax complicating bronchial artery aneurysm. Can Respir J 2005; 12:279–281. [DOI] [PubMed] [Google Scholar]
- 46.Chatterjee A, Ghosh S, Salhiyyah K, et al. A rare presentation of a ruptured bronchial artery aneurysm. Thorax 2004; 59:912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Haddad R. Bronchial artery aneurysm. Eur J Cardiothorac Surg 2004; 26:213. [DOI] [PubMed] [Google Scholar]
- 48.Suen HC, Dumontier CC, Boeren J, et al. Ruptured bronchial artery aneurysm associated with sarcoidosis. J Thorac Cardiovasc Surg 2003; 125:1153–1154. [DOI] [PubMed] [Google Scholar]
- 49.Tringali S, Tiffet O, Berger JL, et al. Bronchial artery aneurysm disguised as a leiomyoma of the esophagus. Ann Thorac Surg 2002; 73:632–633. [DOI] [PubMed] [Google Scholar]
- 50.Pugnale M, Portier F, Lamarre A, et al. Hemomediastinum caused by rupture of a bronchial artery aneurysm: successful treatment by embolization with N-butyl-2-cyanoacrylate. J Vasc Interv Radiol 2001; 12:1351–1352. [DOI] [PubMed] [Google Scholar]
- 51.Sakuma K, Takase K, Saito H, et al. Bronchial artery aneurysm treated with percutaneous transluminal coil embolization. Jpn J Thorac Cardiovasc Surg 2001; 49:330–332. [DOI] [PubMed] [Google Scholar]
- 52.Saito Y, Ueda Y, Imamura H, et al. Operative aneurysmectomy and middle lobectomy for asymptomatic bronchial artery aneurysm in young patient. Eur J Cardiothorac Surg 2000; 18:366–369. [DOI] [PubMed] [Google Scholar]
- 53.Vernhet H, Bousquet C, Jean B, et al. Bronchial aneurysms mimicking aortic aneurysms: endovascular treatment in two patients. Cardiovasc Intervent Radiol 1999; 22:254–257. [DOI] [PubMed] [Google Scholar]
- 54.Kalangos A, Khatchatourian G, Panos A, et al. Ruptured mediastinal bronchial artery aneurysm: a dilemma of diagnosis and therapeutic approach. J Thorac Cardiovasc Surg 1997; 114:853–856. [DOI] [PubMed] [Google Scholar]
- 55.Oka M, Fukuda M, Terashi K, et al. Bronchial artery aneurysm as a cause of atelectasis. Intern Med 1997; 36:917–919. [DOI] [PubMed] [Google Scholar]
- 56.Cearlock JR, Fontaine AB, Urbaneja A, et al. Endovascular treatment of a posttraumatic bronchial artery pseudoaneurysm. J Vasc Interv Radiol 1995; 6:495–496. [DOI] [PubMed] [Google Scholar]
- 57.Connolly B, Manson D, Khattak S, et al. Bronchial artery aneurysm in hyperimmunoglobulinemia E syndrome. Pediatr Radiol 1994; 24:592–593. [DOI] [PubMed] [Google Scholar]
- 58.Shaer AH, Bashist B. Computed tomography of bronchial artery aneurysm with erosion into the esophagus. J Comput Assist Tomogr 1989; 13:1069–1071. [DOI] [PubMed] [Google Scholar]
- 59.Hall RJ, Miller GA, Kerr IH. Ruptured bronchial artery aneurysm mimicking aortic dissection. Br Heart J 1977; 39:909–910. [DOI] [PMC free article] [PubMed] [Google Scholar]