

Introduction
Failure to deliver stents and balloons past tortuous, calcific lesions due to inadequate support has long plagued interventional cardiologists. The mother-daughter technique using a GuideLiner Catheter (Vascular Solutions, Inc. Minneapolis, Minnesota) is now commonly utilized to address these situations.(1, 2) Despite the improved support provided by the GuideLiner catheter, occasions arise in which a single GuideLiner is not adequate to facilitate the delivery of stents or balloons to target lesions. This is especially problematic when attempting percutaneous coronary intervention (PCI) on the retrograde limb of a bypassed coronary through a long saphenous vein graft (SVG). The double bend of the anastomosis into the retrograde coronary artery combined with the antegrade turn of the target branch is often uncrossable even with modern balloon and stent technology. We describe 2 cases of the “mother-daughter-granddaughter” double GuideLiner technique using a 6 Fr GuideLiner inside an 8 Fr GuideLiner to perform highly challenging PCI.
Case 1
72 year old man with a history of remote coronary artery bypass grafting (CABG) with left internal mammary artery to left anterior descending (LAD) and SVG to the first obtuse marginal (OM1) bypass, who later required left main (LM), LAD, and proximal left circumflex (LCX) complex bifurcation stenting presented to his cardiologist with severe refractory chest pain. Subsequent angiography demonstrated that the LM, proximal LCX, and LAD stents were totally occluded. The angiogram also showed a patent SVG to the OM1 with slow retrograde flow into a nearly occluded LCX and second obtuse marginal artery (OM2).
Description of the Procedure Case 1
Given the complexity of the turns required to gain access to the LCX, the mother-daughter-granddaughter double GuideLiner approach was utilized. The mother-daughter-granddaughter system was assembled outside of the body (Figure 1), and the entire unit including the microcatheter was advanced into the coronary. The SVG bypass to the OM1 was wired and the GuideLiner system was advanced so that the microcatheter was located in the OM2. The 6F GuideLiner was placed proximal to the anastomosis of the SVG to OM1 (Figure 2 Panel B). After ballooning the ostial OM1 stenosis, the GuideLiner unit was further advanced into the LCX allowing for the passage of equipment to the distal LCX (Figure 2 Panel C). The vessel was ballooned and stented with excellent angiographic result (Figure 2 Panel D).
Figure 1. Mother-Daughter-Granddaughter Double GuideLiner System.
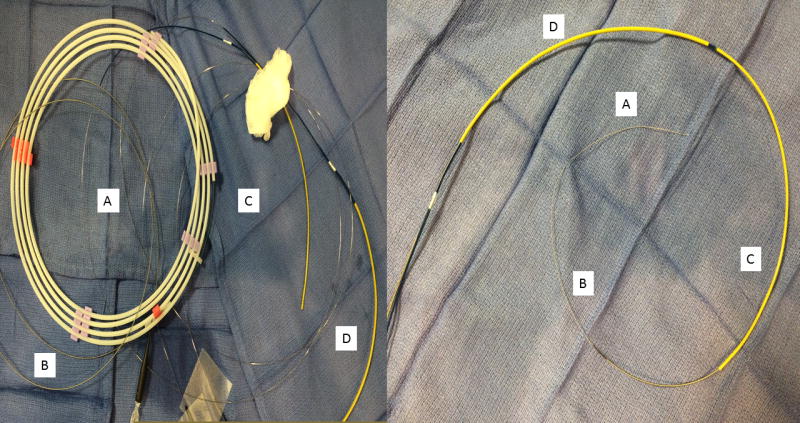
The mother-daughter-granddaughter double guideliner technique requires a 0.014” guidewire (A), a turnpike microcatheter (B), a 6F guideliner (C), and an 8F guideliner (D). The left panel shows the devices prior to assembly and right panel shows the devices assembled.
The dilator of the 8 Fr GuideLiner may be used to dilate into the proximal portion of the 6 Fr GuideLiner (C) to create an improved seal. The device is inserted into the body as a unit. A distal anchor may also be used to aid in deployment.
Figure 2. Angiography and Intervention Case 1.
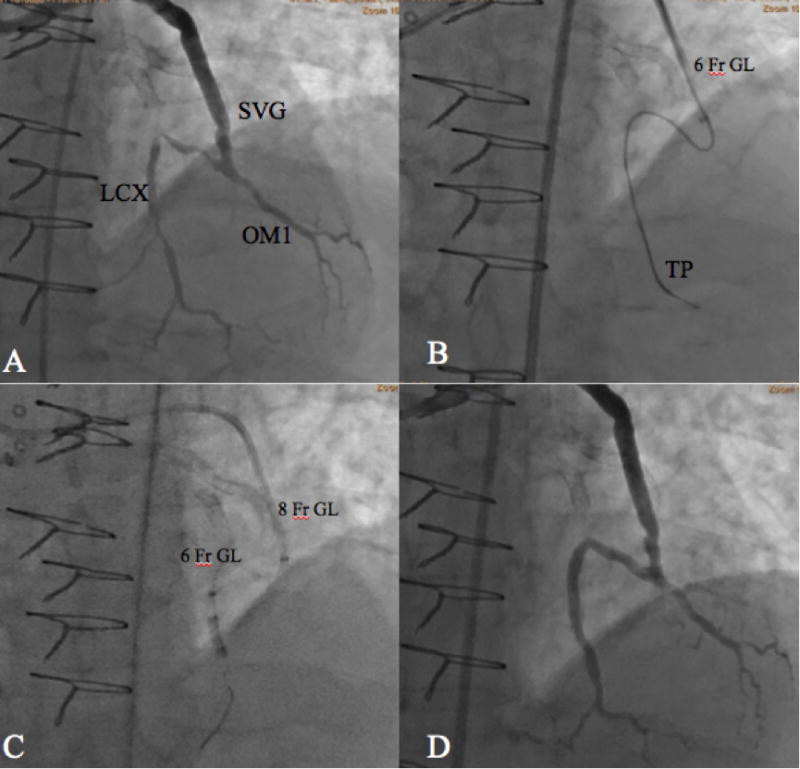
Abbreviations: LCX- Left Circumflex, SVG – Saphenous Vein Graft, OM – Obtuse Marginal, GL- GuideLiner, TP – Turnpike Catheter. Panel A. Diagnostic angiography demonstrating SVG to OM1 with retrograde filling of the LCX and the OM2. Panel B. The 6 Fr GuideLiner (inside the 8 Fr GuideLiner) is shown approaching the distal anastomosis of the SVG to OM1. The turnpike microcatheter and guidewire is positioned in the distal OM2. Panel C. The system has been advanced and a balloon is inflated in the distal LCX. The 6F GuideLiner is positioned beyond the OM1/LCX bifurcation, and the 8F GuideLiner is just proximal to the distal anastomosis of the SVG to OM1. Panel D. The final angiographic result after deploying stents to the distal LCX and proximal portion of the OM1 through the mother-daughter-granddaughter double GuideLiner system
Case 2
The patient is a 73 year old man with a history of mitral valve replacement with bioprosthetic valve and severe coronary artery disease status post remote CABG with known CTO of his LCX (Figure 3 Panel A). He presented with progressive shortness of breath and angina despite maximal antianginal medications. A previous antegrade attempt at CTO PCI of the LCX was unsuccessful.
Figure 3. Angiography and Intervention Case 2.
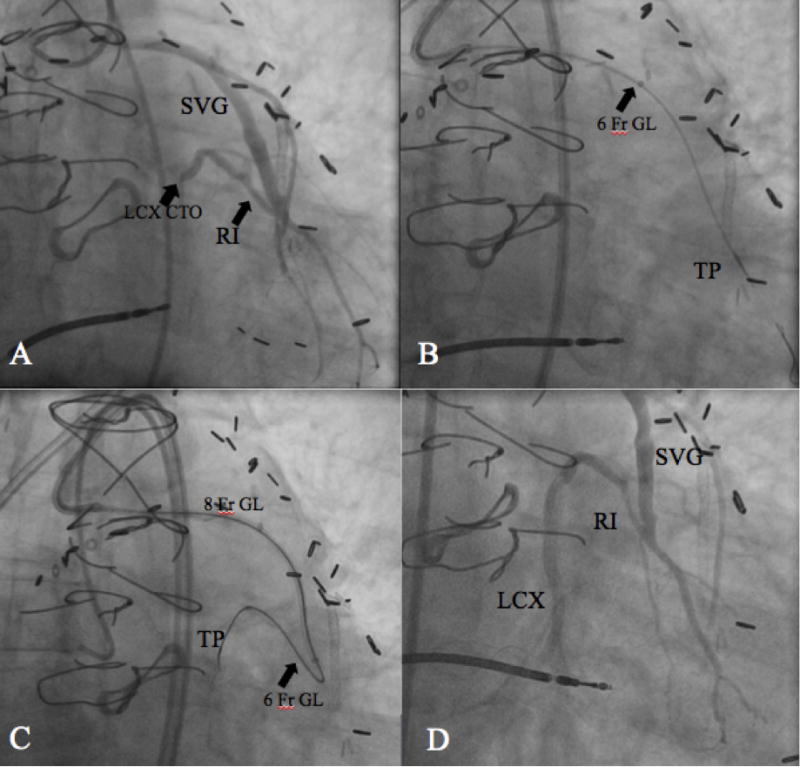
Abbreviations: LCX – Left Circumflex, SVG – Saphenous Vein Graft, RI – Ramus Intermedius, CTO – Chronic total occlusion, GL – GuideLiner, TP: Turnpike catheter. Panel A: Diagnostic angiography displaying SVG to RI with retrograde filling of the RI to the LCX which is chronically occluded distally. Panel B. A guidewire is positioned in the distal RI to allow for advancement of the mother-daughter-granddaughter double GuideLiner system. The 6 Fr GuideLiner is seen in mid portion of SVG and Turnpike in the distal RI. Panel C. The Mother-daughter-granddaughter system is positioned with the 8 Fr GuideLiner ending just prior to the SVG to RI anastomosis. The 6Fr GuideLiner is positioned at the ostium of the native LCX with the turnpike catheter in the LCX. The Turnpike was used to facilitate wire escalation to cross the LCX CTO via an antegrade approach. Panel D. Angiogram after stenting of the CTO LCX into the RI supplied by the SVG.
Description of the Procedure for Case 2
Given the complex nature of the turns needed to approach the LCX CTO, the mother-daughter-granddaughter double GuideLiner was again utilized. The GuideLiner system allowed for navigation of the SVG followed by a sharp turn to wire back to the proximal ramus intermedius (RI). The 6 Fr GuideLiner was positioned near the ostium of the LCX CTO and a Turnpike catheter (Vascular Solutions, Inc. Minneapolis, Minnesota) was used facilitate wire escalation to cross the CTO from an antegrade approach (Figure 3 Panel C). The length of the lesion was then ballooned and stented with two drug eluting stents extending into the obtuse marginal branch (Figure 3 Panel D).
Discussion
GuideLiner-facilitated PCI is becoming increasingly common in clinical practice. A recent retrospective study by Waterbury et al. described over 300 cases of GuideLiner-facilitated PCI and showed an 80% procedural success rate.(3) Additionally, the mother-daughter approach using the GuideLiner has been demonstrated to aid in CTO and SVG PCI.(4)
The presented cases are the first examples of utilization of a GuideLiner within a GuideLiner or the “mother-daughter-granddaughter” double GuideLiner technique. This technique allows navigation of tortuous saphenous grafts to enable wiring of the retrograde limb of the native circulation. This novel technique offers two advantages: 1. delivery of stents through the GuideLiner with “unsheathing”, rather than risky “pushing” of equipment through severe tortuosities 2. improved guide length to approach very distant targets i.e. via saphenous vein grafts.
In the presented cases no complications occurred. Several steps by the operator can be utilized to prevent complications and achieve successful intervention with the double GuideLiner technique. First, injections through the system should generally be avoided to prevent hydraulic vessel dissection. Second, the operator must perform meticulous back-bleeding of the catheters to prevent air entrainment or thrombus embolization. Third, as the double GuideLiner system may occlude blood flow, the patient must be carefully monitored for the development of ischemia and/or hemodynamic instability. Patients with borderline pre-procedural hemodynamics may not tolerate this technique. Finally, the operator should avoid advancing the system only over a coronary wire, but rather should use a microcatheter or a balloon for additional support to reduce the probability of iatrogenic dissection.(3) In conclusion, we report the first two described cases using the mother-daughter-granddaughter double GuideLiner technique to successfully perform highly complex PCI in situations that may have previously been considered technically unapproachable.
Supplementary Material
Acknowledgments
Dr. Karmpaliotis is speaker honoraria from Abbot Vascular, Boston Scientific, Ashai, and Medtronic. Dr. Green is supported by a Career Development Grant Award (K23 HL12114) from the National Heart, Lung, and Blood Institute. Dr. Kandzari receives research/grant support from Biotronik, Boston Scientific, Medinol, Medtronic, and St. Jude/Thoratec; minor consulting honoraria from Boston Scientific and Medtronic. Dr. Nicholson has served as a consultant, proctor, and on the advisory board of Boston Scientific and Abbott Vascular; and has served as a proctor for Asahi Intecc. Dr. Lembo has served on the advisory board of Abbott Vascular. Dr. Thompson is an employee of Boston Scientific.
Footnotes
Disclosures
All other authors have nothing to disclose.
References
- 1.Kumar S, Gorog DA, Secco GG, Di Mario C, Kukreja N. The GuideLiner “child” catheter for percutaneous coronary intervention – early clinical experience. J Invasive Cardiol. 2010;22:495–8. [PubMed] [Google Scholar]
- 2.Repanas TI, Christopoulos G, Brilakis ES. “Candy Cane” Guide Catheter Extension for Stent Delivery. J Invasive Cardiol. 2015;27:E169–70. [PubMed] [Google Scholar]
- 3.Waterbury TM, Sorajja P, Bell MR, Lennon RJ, Mathew V, Singh M, Sandhu GS, Gulati R. Experience and complications associated with use of guide extension catheters in percutaneous coronary intervention. Catheter Cardiovasc Interv. 2015 doi: 10.1002/ccd.26329. [DOI] [PubMed] [Google Scholar]
- 4.Mozid AM, Davies JR, Spratt JC. The utility of a guideliner catheter in retrograde percutaneous coronary intervention of a chronic total occlusion with reverse cart-the “capture” technique. Catheter Cardiovasc Interv. 2014;83:929–32. doi: 10.1002/ccd.25205. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.