

Abstract
Introduction:
A case of malign hemorrhagic renal cyst in a 32 – year–old woman is reported. The patient was admitted to our hospital for further evaluation of right upper abdominal mass. CT scan and ultrasonic sonography showed a right giant renal cystic mass. The characteristic findings were thick and irregular wall and heterogeneous contents of the cystic mass.
Case report:
The presence of a malignant tumor in the cyst wall was suspected and nephrectomy was performed. The specimen measured 10 x 6 x 4 cm. The cyst contained bloody fluid and a hemorrhagic degenerating mass. Pathohistological examination showed evidence of malignant hemorrhagic renal cyst.
Keywords: kidney, malignant cyst, nephrectomy
1. INTRODUCTION
Renal cysts, in general, may be classified as “simple” or “complex”. “Simple” cysts are best defined using sonographic criteria. The difficulty arises when cysts do not meet the rigid characteristics of the “simple” definition. Therefore, clinicians need to rely on a rapid, safe and accurate system to identify benign versus malignant masses and ultimately have the guidance on nonsurgical or surgical treatment options. Malignant renal cyst is a very rare disease. In literature are prescribed as 0.5-1% of all renal cysts (1, 2). Their clinical symptoms are not specific and are mainly similar to the symptomatology of tumors and simple renal cysts (3, 8). Pre operative diagnostics procedure as intravenous urography–IVU, ultrasonic sonography, computed tomography - CT, magnetic resonance imaging - MRI, diagnostic punction of cysts and renal arteriography can rare determine the diagnosis (4, 5). The diagnosis based on Bosniak classification: Bosniak 1, Bosniak 2, Bosniak 2F, Bosniak 3 and Bosniak 4. Therefore the diagnosis is mostly determined by surgical intervention (6, 7). In this study, the authors have presented their case of hemorrhagic malignant renal cyst, which is treated by surgical intervention–nephrectomy.
2. MATERIALS AND METHODS
We are going to present the case of a female patient referred to our clinic with the initial ultrasound diagnosis of right giant renal cyst about 10 cm. Physical examination revealed no abnormalities. Given the result of the ultrasound (thick walls and small irregularities) and the possibility of a complicated cyst, we decided to investigate the matter further, and programmed the patient for an enhanced abdominal computer tomography with intravenous contrast.
The enhanced CT images revealed a right kidney cystic mass, with a 10 cm diameter, thick irregular walls with contrast enhancement, hyperdense content, and no pathological lymph nodes or distant metastases. The diagnosis was a Bosniak IV.
The Albanian Urological Association Guidelines Committee has reviewed the literature using a Medline search of the English language.
3. CASE PRESENTATION
Patient: Xh.B, female 32 years old. Symptoms: pain and feeling heaviness below right rib arch and right flank, for a long time intermittently and now more frequently. No hematuria noted elevated blood pressure Laboratory assessment: ESR: 10; Glucose: 4.32; urea: 6.30; creatinine: 63.2; Hgb: 127; RBC: 3.73; WBC: 7.6l; Hct: 0.36.
Figure 1.

A and 1B. Intravenous urography–IVU. There is a large well defined formation that occupies about upper two–thirds of the right kidney.
Figure 2.
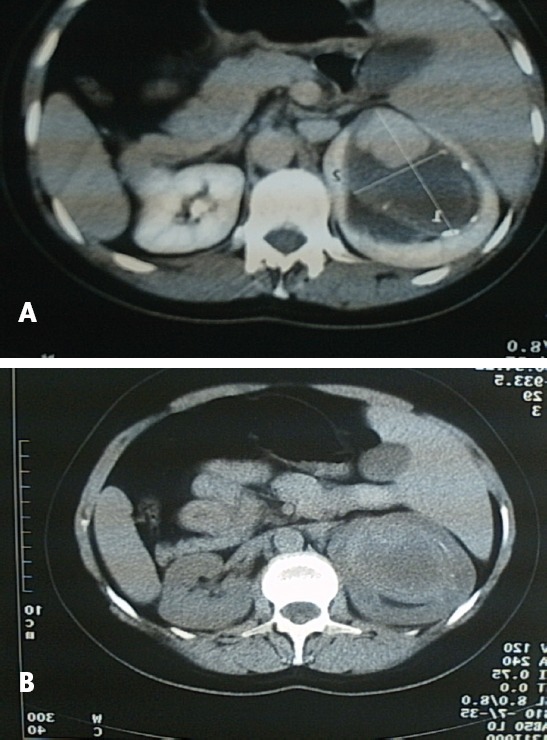
(A.B): CT of the right kidney; Radiologist`s comment: Very large renal mass lesion that occupies about upper two–thirds of right kidney.
Echotomografic findings: There is a large well defined formation that occupies about upper two -three of the right kidney sized 10 x 6 x 4 cm hypoechogenic with hyperechogenic walls.
4. DISCUSSION
Diagnosis is mainly based on histopathological features such as a well-developed capsule, fibrous stromata, multiple epithelial lining septa. According to Bosniak the renal cysts can be classified into 5 types. A simple renal cyst grows up of renal parenchyma. The cyst is filled with fluid and can cause local tissue destruction as it enlarged. Many cysts cause no symptoms and are discovered accidentally during other assessment or autopsy. Although the exact cause is unknown, cysts are considered structural defect that occurs prenatally. Diagnosis of a simple renal cyst involves intravenous urography, echosonogarphy, diagnostic puncture, CT, MRI. Echosonogarphy is the most commonly applied method because it reveals some features of cysts of suggesting malignancy: irregular walls, internal echoes inside the walls and the cysts, lack of characteristic potentiation of ultrasound beam (F).This indicate diagnostic punction and analysis cyst contents. If the aspirate is bloody there is (Tomas¹ 2010) a 28 - 50 % chance of malignancy.
Figure 3.

A, 3B and 3C. Surgical intervention: Right nephrectomy. Surgical finding: there is an a large cystic formation that incorporate upper pole and middle area of the right kidney with thick and calcified capsule filled with hemorrhagic fluid and masse of loose costs.
Bosniak 1. Simple cyst: Imperceptible wall, rounded. Work-up: nil. Percentage malignant: ~0%.
Bosniak 2. Minimally complex: A few thin <1 mm septa or thin calcifications (thickness not measurable); non-enhancing high-attenuation (due to proteinaceous or hemorrhagic contents) renal lesions of less than 3 cm are also included in this category; these lesions are generally well marginated. Work-up: nil. Percentage malignant: ~ 0%.
Bosniak 2F. Minimally complex: Increased number of septal, minimally thickened with nodular or thick calcifications. But no measurable contrast enhancement enhancing. Hyperdense cyst > 3 cm diameter, mostly intrarenal (less than 25% of wall visible); no enhancement. Requiring follow-up: needs ultrasound. CT of follow up - no strict rules on the time frame but reasonable at 6 months. Percentage malignant: ~ 5%.
Bosniak 3. Indeterminate: Thick, nodular multiple septa or wall with measurable enhancement, hyperdense on CT (see 2F). Treatment/work-up: partial nephrectomy or radio-frequency ablation in elderly or poor surgical candidates. Percentage malignant: ~ 55%.
Bosniak 4. Clearly malignant: Solid mass with a large cystic or a necrotic component. Treatment: partial or total nephrectomy. Percentage malignant: ~ 100%.
Our case was classified in stage Bosniak IV. Identifications of malignant cells established the definite diagnosis, while hemorrhagic contents, high lipid contention and lactate dehydrogenase - LDH are suggestive of malignancy. After pathological confirmation for malignant kidney cyst and adequate treatment, on these patients is likely to achieve long-term survival. The therapy of malignant cysts is always surgical and usually nephrectomy.
5. CONCLUSION
The characteristic findings were thick and irregular wall and heterogeneous contents of the cystic mass. The cyst contained bloody fluid and a hemorrhagic degenerating mass. Pathohistological examination showed evidence of malignant hemorrhagic renal cyst. Which is treated by surgical intervention and usually nephrotomy.
Footnotes
• Competing interests: None declared.
• Author’s contributions: NSH performed the examination of the patient, has treated and performed the follow up. HA collected the data, analyzed them and writing the text. RXH performed urological examination and assist in writing the text. ASH has analyzed the images and assist in writing the text. MXH performed urological examination and recommendation publication. All authors read and approved the final manuscript.
REFERENCES
- 1.Thomas FW. Guidelines on the management of renal cyst disease. Can Urol Assoc J. 2010 Apr;4(2):98–99. doi: 10.5489/cuaj.10023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Harisinghani MG, et al. Incidence of malignancy in complex cystic renal masses (Bosniak category III):should imaging-guided biopsy precede surgery? AJR - Am J Roentgenol. 2003 Mar;180(3):755–8. doi: 10.2214/ajr.180.3.1800755. [DOI] [PubMed] [Google Scholar]
- 3.Ascenti G, Mazziotti S, Zimbaro G, et al. Complex cystic renal masses:characterization with contrast-enhanced US. Radiology. 2007;243:158–65. doi: 10.1148/radiol.2431051924. [DOI] [PubMed] [Google Scholar]
- 4.Lane BR, Campbell SC, Remer EM, et al. Adult cystic nephroma and mixed epithelial and stromal tumor of the kidney:clinical, radiographic, and pathologic characteristics. Urology. 2008;71:1142–8. doi: 10.1016/j.urology.2007.11.106. [DOI] [PubMed] [Google Scholar]
- 5.Moch H. Cystic renal tumors:new entities and novel concepts. Adv Anat Pathol. 2010;17:209–214. doi: 10.1097/PAP.0b013e3181d98c9d. [DOI] [PubMed] [Google Scholar]
- 6.Webster WS, et al. Surgical resection provides excellent outcomes for patients with cystic clear cell renal cell carcinoma. Urology. 2007;70:900–10. doi: 10.1016/j.urology.2007.05.029. [DOI] [PubMed] [Google Scholar]
- 7.You D, et al. Multilocular cystic renal cell carcinoma:clinicopathological features and preoperative prediction using multiphase computed tomography. BJU Int. 2011;108:1444–9. doi: 10.1111/j.1464-410X.2011.10247.x. [DOI] [PubMed] [Google Scholar]
- 8.Kuroda N, Ohe C, Mikami S, Inoue K, Nagashima Y, Cohen RJ, Pan CC, Michal M, Hes O. Multilocular cystic renal cell carcinoma with focus on clinical and pathobiological aspects. Histopathol. 2012;27:969–74. doi: 10.14670/HH-27.969. [DOI] [PubMed] [Google Scholar]