

Abstract
Introduction:
Glaucoma is the most common optic neuropathy which is characterized by progressive loss of retinal ganglion cells, the excavation of the optic nerve head, associated with defects in the visual field. It is not a disease, but the final result of united and yet completely unidentified cellular and subcellular processes and effects of many factors responsible for changes in retinal ganglion cells leading to their accelerated apoptosis.
Methods:
This is a prospective-retrospective, comparative, randomized clinical trial that included 150 patients, 97 were female and 53 male. The age of patients ranged from 18 to 80 years.
Results:
The highest degree of myopia in category of tilted optic discs had patients with large disc (4.05 + -0.65). Values of the degree of myopia have linearly declined in relation to the size of the oblique disc. The analysis of the results revealed that the subjects who had a higher degree of myopia associated with glaucoma had frequent parapapillar atrophy of alpha and beta zones. The highest percentage of subjects with parapapillar changes were in the group of patients who had other than glaucoma and myopia (62%), then in the group of patients with glaucoma only (56%).
Conclusion:
Previous studies on the relationship between myopia and open-angle glaucoma are based on the results of observational studies. However, according to recent findings, based on the available studies, the systematic approach to estimate the association between myopia and glaucoma does not exist. Disc Damage Likelihood Scale (DDLS) is a new system for assessing glaucomatous damage of the optic disc which strongly correlates with the degree of visual field loss.
Keywords: optic neuropathy, glaucoma, early detection
1. INTRODUCTION
Glaucoma is the most common optic neuropathy which is characterized by progressive loss of retinal ganglion cells, the excavation of the optic nerve head, associated with defects in the visual field (1). It is believed that the pathophysiology of glaucoma is multifactorial. Multiple factors are equally active in cell bodies and their axons leading to the death of retinal ganglion cells.
It is not a disease, but the final result of united and yet completely unidentified cellular and subcellular processes and effects of many factors responsible for changes in retinal ganglion cells leading to their accelerated apoptosis. Since glaucoma is a sindrome of eye disease in which there is damage to the optic nerve, and if left untreated can result in total loss of sight. Defects in the nerve fiber layer of the retina prior to visible changes at the head of the optic nerve and defects in the visual field are detected when it is already 40% of axons irretrievably lost (2). Glaucoma is the second cause of blindness worldwide, after cataracts, and unlike cataract, glaucoma causes irreversible blindness.
According to the World Health Organization (WHO) and the World Association of Glaucomatologist (WGO), in the year 2010, 66.8 million people worldwide suffer from glaucoma, and 6.7 million are blind from this disease (3).
2. OBJECTIVE
Primary glaucoma is a disease that occurs insidiously, without notice. It manifests itself in damage to the optic nerve, loss of vision and eventually decline in central visual acuity (4). In order to understand and assess the presence of glaucomatous changes in the optic nerve, it is necessary to know and understand the optic nerve head characteristics of healthy people. As in other biological characteristics, changes on the optic nerve head differ among healthy population, impeding recognition of pathological changes (5).
The relationship between the optic disc size, neuroretinal rim and cup/disc ratio, are crucial in identifying glaukomatous changes in the optic nerve head (6). Scleral channel is the gateway to the retinal nerve fibers that leave the eye. Typically it is the oval cross-section of 1,75mm. Size depends on the size of the optical disc, and the size of the bulbus. Eyes with small scleral canal have small optical discs, and those with large channels have large discs (7). Different ways of entering the optic nerve in the sclera provides irregular and unusual look like optical discs such as tilted disc. According to recent research, the link between myopia and glaucoma remains unexplained in most cases, mainly due to the fact that it is difficult to sort out the structural and functional abnormalities we meet in myopia from the ‘real’ glaucoma changes (8).
There is strong epidemiological evidence linking myopia and glaucoma. Miopic optic disc can be a major challenge in terms of correct diagnosis of glaucoma. By using optical coherence tomography, it was found that myopia is associated with changes in retinal nerve fiber layer, in the form of temporal displacement and the thinning of the upper and lower segments of retinal layers of nerve fibers. As is the case with all the progressive condition, it is often not possible to distinguish glaucomatous from nonglaucomatous changes of the optical disc based on a single examination, but the follow up by the OCT analysis of the optic nerve head and associated changes in the visual field may result in the usefull data (9).
Although myopia is a known risk factor for glaucoma, it can also lead to structural and functional defects that can not be distinguished from those caused by glaucoma (10).
3. MATERIALS AND METHODS
This is a prospective-retrospective, comparative, randomized clinical trial that included 150 patients, 97 were female and 53 male. The age of patients ranged from 18 to 80 years. In order to make scientifically valuable statistical comparison, a total of 300 eyes was examined, ie. 100 eyes in 3 groups of patients of both sexes: Group I - patients with glaucoma, Group II - patients with myopia and glaucoma, Group III - patients only with myopia. Criteria for inclusion in the study: patients with myopia, the patients of both sexes Caucasian, patients older than 18 and younger than 80 years, patients who are diagnosed with glaucoma, patients who, in addition to ophthalmologic tests carried out and test with SOCT 3D and computerized perimetry test, we took into account only those results in which the reliability factor (RF) was in the permissible overdrafts, under 15%. Criteria for exclusion from the study:patients with a previous ophthalmic surgery or laser treatment to the eye that is the subject of tests, patients with other diseases of the eye (macular disease, hemophtalmos, cataracts, uveitis, keratitis), patients with head injuries and eye patients neuroophthalmological diseases and diseases of the retina that may affect the visual field disturbance (neuritis, eye contusion, retinopathy), patients with neuropsychiatric disorders, patients with claustrophobia and inability to withstand the tests of the visual field to the end, patients in which the reliability factor in excess of 15%, patients being treated with chemotherapeutic agents, anti-metabolites, patients with severe systemic diseases. All patients after anamnesis underwent following ophthalmological examination: natural visual acuity and best corrected visual acuity, applanation tonometry Goldman, biomicroscope examination autorefractometry, gonioscopy, fundus examination - direct ophthalmoscopy (stereobiomicroscopy Volk lens + 90D), three-dimensional spectral optical coherence tomography (SOCT 3D), static computerized perimetry (KOWA).
4. RESULTS
The The study included 300 eyes of patients who were divided into three equal groups, according to the criteria for inclusion in the study. The first group includes subjects diagnosed with glaucoma and analyzed 100 eyes with glaucoma, the second group includes subjects who have been diagnosed with glaucoma and myopia (n = 100), and the third group includes participants only with myopia (n = 100).
Table 1 shows the average age of the respondents in relation to the experimental group. The average age of patients with glaucoma was 65.83 ± 14.15 years (18-86), while the average age of patients with glaucoma and myopia was 64.26 ± 12.68 years (27-82). The average age of patients with myopia amounted to 50.09 ± 17 years (23-81), and the participants of this group were significantly younger than did those in the first two groups, F = 34,668; p <0.05 (Table 2).
Table 1.
The average age of the respondents in relation to the study group

Table 2.
Gender structure of respondents

Of the total number of subjects included in this study (n300), males were 35.3% and female 64.7%. In all three groups dominated the respondents were female and not a statistically significant difference compared to the test group, χ2 = 0.381; p = 0.827. An analysis of the average value of the height of the diopter in patients with myopia in subjects which in addition to glaucoma and myopia have established a statistically significant difference (Table 3). The average height of the diopter in patients with glaucoma and myopia amounted to -3.77 ± 1.55, while in patients with myopia it was only -2.49 ± 1.25, F = 40,940; p <0.05 (Table 4). Statistically significant difference was found in DDLS values in relation to RNFL findings in patients with glaucoma in all three of optical disc sizes using Hi-square test (Table 5). In the group of patients that have had a large optic disc, the average cup disc diameter size was significantly higher in patients with myopia than in the other two test groups (p <0.05). However, in patients who have a medium optic disc size, the cup disc diameter was significantly higher in patients who have had myopia and glaucoma, as compared to subjects who had only glaucoma or just myopia (p <0.05). In patients with small disc was no significant difference in the average cup disc diameter (p = 0.139) (Table 6).
Table 3.
Myopia degree in relation to the study group
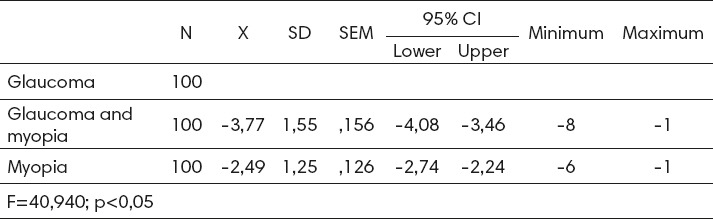
Table 4.
DDLS impact on RNFL findings in relation to the study group and the size of the optic disc

Table 5.
Average cup disc diameters in relation to the optic disc size

Table 6.
Average DDLS values in relation to the optic disc size

Through the analysis of the average DDLS values in relation to the optic disc size of the respondents in the study groups we established a statistically significant difference only for large discs considering the DDLS values in other participants study groups (p = 0.033), in patients who have had small and medium disc size a statistically significant difference has not been established. It was also found that respondents with a higher degree of visual field changes have greater DDLS values (Chart 1). It is important to note that the subjects with terminal stage in visual field loss in the group with diagnosed glaucoma had average DDLS value 7.11, and those with a joint diagnosis of glaucoma and myopia 8.75 of the DDLS (Chart 2). By determining the average DDLS values in relation to the optic disc mophology in all study groups we established a statistically significant difference among the three groups considering the shape and DDLS values (Chart 3). Respondents with tilted discs had a significantly higher DDLS values in relation to the patients with other forms of the disc in all three groups (p <0.05).
Chart 1.

Average DDLS values in relation to the visual field changes of the respondents in all study groups
Chart 2.

Average DDLS values compared to the optic disc morphology in all analyzed groups
Chart 3.

The average value of myopia in relation to the size and shape of the optic disc
5. DISCUSSION
Previous studies on the relationship between myopia and open-angle glaucoma are based on the results of observational studies. However, according to recent findings, based on the available studies, the systematic approach to estimate the association between myopia and glaucoma does not exist. Myopic eyes have a longer axial length. Experimental models of myopia and epidemiological data have shown that myopia is most often the result of disproportionate elongation of the posterior segment of the eye, which physically limits the fibrous sclera. In general, the axial length is the most important element of the refraction of the eye, which most determines the occurrence of refractive errors (11). Such eyes seem to have a greater lamina cribrosae deformation. This could contribute to the greater sensitivity of the optic nerve head in glaucoma changes (12). No one knows with absolute certainty what causes myopia, but they noticed a certain connection between the occurrence of myopia and certain factors that are reasonably believed to have a significant role in its development. Some of the potential risk factors are: race, ethnicity, industrial development, heredity, education, profession, environment, gender, diet, stress, and other factors. Gvozdenovic and colleagues in their study concluded that optic discs of glaucoma patients with high myopia have a larger diameter, larger and more irregular distributed neuroretinal rim zone damage and thinner retinal nerve fiber layer than in glaucoma patients with low myopia (4). Kimura and colleagues have been examining the damage of retinal nerve fiber layer RNFL for early glaucoma in eyes with high myopia, reaching important results. These results suggest that in high myopia common nerve damage is the damage of the papillomacular nerve fiber layer in early stage of glaucoma (10).
6. CONCLUSIONS
The evaluation of morphological parameters of the optic nerve head and peripapillary areas of testing in patients with different degree of myopia we are one step closer to identifying changes in the optic disc as the earliest signs related to glaucoma. Via analysis of comorbidity of glaucoma and myopia, it is possible to make the algorithm of diagnostic techniques and procedures for early detection of glaucoma. Disc Damage Likelihood Scale (DDLS) is a new system for assessing glaucomatous damage of the optic disc which strongly correlates with the degree of visual field loss. The average age of the respondents ranged from 50 to 66 years and in all three groups dominated female patients. We did not found a statistically significant effect of age on the development of glaucoma. The analysis of the results did not established influence of gender on the form of an optic disc. The highest percentage of male respondents (50.9%) and female (62.4%) had a round optic disc, and then tilted (22.3%) and oval (14.3%). The highest degree of myopia, regerdless the optic disc size had patients with tilted optic disc in all three groups. The highest degree of myopia in category of tilted optic discs had patients with large disc(4.05 + -0.65). Values of the degree of myopia have linearly declined in relation to the size of the oblique disc. The analysis of the results revealed that the subjects who had a higher degree of myopia associated with glaucoma had frequent parapapillar atrophy of alpha and beta zones. The highest percentage of subjects with parapapillar changes were in the group of patients who had other than glaucoma and myopia (62%), then in the group of patients with glaucoma only (56%).
Footnotes
• Conflict of interest: None declared.
REFERENCES
- 1.Flammer J, Orgül S, Costa VP, Orzalesi N, Krieglstein GK, Serra LM, Renard JP, Stefánsson E. The impact of ocular blood flow in glaucoma. Prog Retin Eye Res. 2002;21:359–63. doi: 10.1016/s1350-9462(02)00008-3. [DOI] [PubMed] [Google Scholar]
- 2.Dervisevic E. Myopia impact on morphometric parameters of the optical disc in glaucoma patients. University of Tuzla, Doctoral thesis. 2015 [Google Scholar]
- 3.Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–7. doi: 10.1136/bjo.2005.081224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gvozdenovic R, Risovic D, Marjanovic Vukovic D, Stankovic B. Morphometric characteristics of optic disc in patients with myopia and primary open-angle glaucoma. Vojnosanit Pregl. 2013;70:51–6. doi: 10.2298/vsp111229024g. [DOI] [PubMed] [Google Scholar]
- 5.Medeiros FA, Pinheiro A, Moura FC, Leal BC, Susanna R., Jr Intraocular pressure fluctuations in medical versus surgically treated glaucomatous patients. J Ocul Pharmacol Ther. 2002;18:489–98. doi: 10.1089/108076802321021036. [DOI] [PubMed] [Google Scholar]
- 6.Susanna R, Medeiros FA. Optic nerve in glaucoma. 1. izdanje. Udruženje oftalmologa Srbije. Narodna biblioteka Srbije. 2011:15–46. [Google Scholar]
- 7.Chandra A, Bandyopadhyay AK, Bhaduri G. A comparative study of two methods of optic disc evaluation in patients of glaucoma. Oman J Ophthalmol. 2013;6:103–7. doi: 10.4103/0974-620X.116643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jonas JB, Budde WM. Optic nerve damage in highly myopic eyes with chronic open-angle glaucoma. Eur J Ophthalmol. 2005;15:41–47. doi: 10.1177/112067210501500107. [DOI] [PubMed] [Google Scholar]
- 9.Detry-Morel M.J. Is myopia a risk factor for glaucoma? Fr Ophtalmol. 2011;34:392–5. doi: 10.1016/j.jfo.2011.03.009. [DOI] [PubMed] [Google Scholar]
- 10.Kimura Y, Akagi T, Hangai M, Takayama K, Hasegawa T, Suda K, Yoshikawa M, Yamada H, Nakanishi H, Unoki N, Ikeda HO, Yoshimura N. Lamina cribrosa defects and optic disc morphology in primary open angle glaucoma with high myopia. PLoS One. 2014;22:45–8. doi: 10.1371/journal.pone.0115313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chang RT, Singh K. Myopia and glaucoma:diagnostic and therapeutic challenges. Curr Opin Ophthalmol. 2013;24:96–101. doi: 10.1097/ICU.0b013e32835cef31. [DOI] [PubMed] [Google Scholar]
- 12.Agarwal R, Gupta SK, Agarwal P, Saxena R, Agrawal SS. Current concepts in the pathophysiology of glaucoma. Indian J Ophthalmol. 2009;57:257–66. doi: 10.4103/0301-4738.53049. [DOI] [PMC free article] [PubMed] [Google Scholar]