

Abstract
Context:
Distinct exercises have been proposed for knee rehabilitation after anterior cruciate ligament (ACL) reconstruction. There is a need to understand ACL strain behavior during different rehabilitation exercises to protect the graft from excessive strain that could interfere with its healing process.
Objective:
To critically review studies that directly measured normal ACL strain in vivo during different movements, conditions, or exercises to gain insight into which of them may produce more strain on the ligament or the ligament graft in the case of reconstructed knees.
Data Sources:
A literature search of PubMed, CINAHL, SPORTDiscus, and PEDro databases was conducted. Keywords included anterior cruciate ligament, strain, stress, deformation, transducer, rehabilitation, rehabilitation exercise, physical therapy, and physiotherapy.
Study Selection:
Inclusion criteria were (1) peer-reviewed studies published in English or Spanish, (2) research conducted on adult human subjects with normal ACLs and healthy knees, and (3) ACL strain directly measured during different movements, conditions, or exercises by using a transducer.
Study Design:
Systematic review.
Level of Evidence:
Level 4.
Data Extraction:
Specific data were abstracted from the selected studies, including isometric quadriceps and hamstrings activity, active and passive flexion-extension of the knee, closed kinetic chain exercises, and application of joint compressive load.
Results:
A total of 10 studies met all criteria and were included in the final analysis. The strain values produced by closed kinetic chain and open kinetic chain exercises were similar. However, closed kinetic chain exercises appear to attenuate the strain increase that occurs in open kinetic chain exercises when increasing resistance.
Conclusion:
These data may be relevant to develop rehabilitation exercises or programs that do not endanger the healing ACL graft and to provide a basis for future clinical trials.
Keywords: anterior cruciate ligament, strain, biomechanics, rehabilitation
The choice of the optimal rehabilitation program after anterior cruciate ligament (ACL) reconstruction has always been a controversial issue since several different rehabilitation protocols have been prescribed.22,24,26 Many studies have investigated and compared the effects of closed kinetic chain (CKC) and open kinetic chain (OKC) exercises—also called weightbearing and nonweightbearing exercises, respectively—on the knees of subjects with ACL deficiency or reconstruction.5,11,19,21 In any case, there is no doubt that the healing ACL graft is vulnerable during the first stages of rehabilitation,27 suggesting that rehabilitation exercises should not produce strain levels sufficient to endanger the structural integrity of the graft. Orthopaedic physical therapists must therefore be cautious when loading the ACL graft because a too aggressive rehabilitation could be deleterious. Consequently, the optimal rehabilitation program may restore normal range of motion and rapidly recover muscle strength level previous to the injury without producing excessive strain on the ACL graft that could interfere with its healing process.25 Thus, it is of great importance to know which movements, exercises, or conditions produce more ACL strain.
The ACL strain behavior has been investigated both in human cadavers and living subjects through different approaches and techniques (directly with transducers and indirectly with instrumentation to measure anterior tibial translation or with biomechanical models, etc).1,6,17,23 The main purposes of this systematic review were to (1) identify studies that directly measured the human normal ACL strain in vivo during different movements, conditions, or rehabilitation exercises and (2) gain insight into which exercises or conditions produce more strain on the ACL and, consequently, on the ACL graft in the case of reconstructed knees. We selected only in vivo studies that performed direct measurements because their data may be more meaningful than those from in vitro studies and indirect approaches; normal muscle tone and activity characteristic of living musculature are factors that affect the ACL strain behavior.
Methods
Protocol and Registration
A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.20 The review was registered in the PROSPERO International Prospective Register of Systematic Reviews.
Data Sources and Searches
A literature search was conducted using the PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), SPORTDiscus, and Physiotherapy Evidence Database (PEDro) electronic databases from inception through November 2014. Search terms were anterior cruciate ligament, ACL, tension, tensile, strain, stress, deformation, transducer, sensor, rehabilitation, rehabilitation exercise, physical therapy, and physiotherapy. Combinations of 2 search terms were introduced in databases that did not allow complex algorithms. Additionally, when the database permitted, the search filter humans was used. Besides the electronic literature search, an additional search was completed by examination of reference lists from the articles included in the systematic review and from other relevant reviews to identify pertinent studies not retrieved by databases. Potential relevant studies from other sources were also considered.
Eligibility Criteria
Inclusion criteria were: peer-reviewed studies published in English or Spanish, conducted on adult humans who had normal ACLs and healthy knees, and that directly measured the ACL strain produced during movements, conditions, or exercises using a transducer. Exclusion criteria were: articles limited to abstract form, case studies, studies conducted on cadavers, deficient or reconstructed ACLs, and the use of functional knee braces or external stabilizers by the participants.
Study Selection
Two reviewers independently conducted the study selection process based on inclusion and exclusion criteria. Where necessary, studies were obtained in full text to finally determine whether they were valid for inclusion in the systematic review. Discrepancies between the independent reviewers were resolved by discussion and consensus between them.
Methodological Quality Assessment
The methodological quality of each study in the systematic review was assessed using the PEDro scale,18 which consists of 11 items. A study evaluated by this scale receives 1 point for each item that it meets, so the maximum possible total score is 11 points.
Results
Study Selection
After the full-text assessment of 19 studies, 9 were excluded because of the following reasons: 6 studies did not measure the ACL strain directly with a transducer but with biomechanical models, and 3 studies were in vitro (ie, conducted on cadavers), leaving a total of 10 studies2-4,7-10,12,14,16 that met the eligibility criteria and were selected for final inclusion in the systematic review (Figure 1). The additional search, consisting of examination of reference lists, did not identify any eligible study that had not been previously retrieved through database searching. All selected studies were from a single laboratory.
Figure 1.
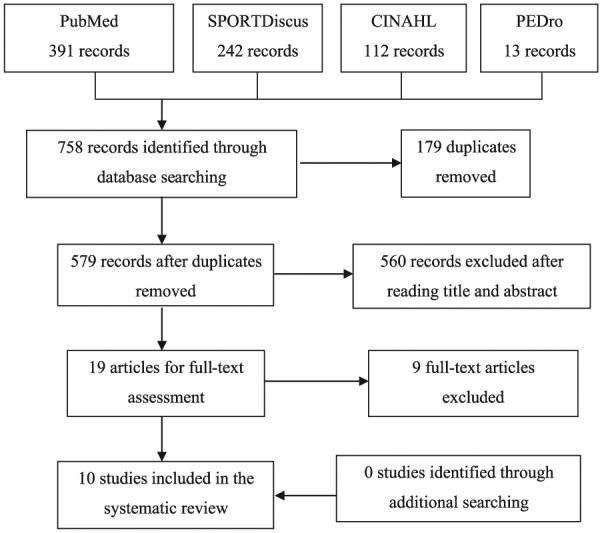
Flow diagram: Study selection process.
Methodological Quality
The 10 included studies scored 3 of 11 on the PEDro scale. They all met the same items: 1, 8, and 11.
Study Characteristics
All 10 included studies were controlled laboratory studies with the same experimental design. They included a total of 82 participants, of whom 52 were men and 11 were women; the sex of the remaining 19 participants was not reported. Therefore, the mean sample size was 8.2, ranging from 5 to 11. The overall age range of study participants was 18 to 64 years (Table 1). Subjects participating in all studies were healthy volunteers who were undergoing knee arthroscopy, immediately after which a transducer was implanted and they performed the exercises or activities in which ACL strain was measured (Table 2).
Table 1.
Study data
| Study | Year | Transducer | Sample Size (Sex) | Age, y, Mean (Range) |
|---|---|---|---|---|
| Howe et al16 | 1990 | HEST | n = 5 (5 M) | 30.6 (24-39) |
| Beynnon et al3 | 1992 | HEST | n = 10 (10 M) | 25 (18-40) |
| Fleming et al7 | 1993 | HEST | n = 5 (5 M) | NR (18-40) |
| Beynnon et al2 | 1995 | HEST | n = 11 (M and W) | NR (22-41) |
| Beynnon et al4 | 1997 | DVRT | n = 8 (NR) | NR (22-40) |
| Fleming et al9 | 1998 | DVRT | n = 8 (6 M and 2 W) | 41.9 (33-53) |
| Fleming et al8 | 1999 | DVRT | n = 5 (5 M) | 39.6 (23-49) |
| Fleming et al12 | 2001 | DVRT | n = 11 (9 M and 2 W) | 40.6 (26-64) |
| Fleming et al10 | 2003 | DVRT | n = 10 (7 M and 3 W) | 33 (20-49) |
| Heijne et al14 | 2004 | DVRT | n = 9 (5 M and 4 W) | 31.2 (20-49) |
DVRT, differential variable reluctance transducer; HEST, Hall effect strain transducer; M, men; NR, not reported; W, women.
Table 2.
Exercises or activities performed and results a
| Study | Exercises or Activities | Results (Strain Values, %) |
|---|---|---|
| Howe et al16 | A-P load at 30° and 90° (4 cycles to limits of ±200 N) Isometric quadriceps contractions at 30° and 90° (4 contractions to maximal effort) |
A-P load → MSV (at 150 N of anterior load) 30°: 4.0; 90°: 2.3 IsoQuadsCont → MSV (at 27 N·m) 30°: 3.9; 90°: NA (≤0) |
| Beynnon et al3 | A-P load at 30° and 90° (4 cycles to limits of ±150 N) Isometric quadriceps contractions at 30° and 90° (4 contractions to approximately 80% of maximal effort) AFE and PFE (4 continuous cycles from 5° to 110°) |
A-P load → MSV (at 150 N of anterior load) 30°: 3.7; 90°: 1.8 IsoQuadsCont → MSV (at 27 N·m) 30°: 3.2; 90°: −2.5 AFE → MPSV 2.8 at 20°; MmSV −3.5 at 110°; S-T transition at 48° PFE → MPSV 0.1 at 10°; MmSV −4.1 at 50°; S-T transition at 11.5° |
| Fleming et al7 | A-P load at 30° and 90° (4 cycles to limits of ±160 N) | A-P load → MSV (at 150 N of anterior load) 30°: 3.0; 90°: 0.9 |
| Beynnon et al2 | AFE with and without weight (45 N) on the ankle (4 continuous cycles from 5° to 90°) Alternating isometric quadriceps and hamstrings contractions at 15°, 30°, 60°, and 90° (4 cycles to approximately 80% of maximal effort) Simultaneous quadriceps and hamstrings contraction at 15°, 30°, 60°, and 90° (to maximal effort) |
AFE without weight → MPSV 2.8 at 10°; MmSV −2.0 at 90°; S-T transition at 35° AFE with weight → MPSV 3.8 at 10°; MmSV −1.5 at 90°; S-T transition at 45° IsoQuadsCont → MSV (at 30 N·m) 15°: 4.4; 30°: 2.0 SimQuadsHamsCont → MSV 15°: 2.8; 30°: 0.4 |
| Beynnon et al4 | AFE (4 continuous cycles from 5° to 90°) Squat (with and without elastic resistance) (4 repetitions) |
AFE → MPSV 3.8 at approximately 10° Squat without resistance → MPSV 3.6 at approximately 10° Squat with resistance → MPSV 4.0 at approximately 10° |
| Fleming et al9 | Stationary bicycling, 6 conditions: power levels (75, 125, and 175 W) at 2 cadences (60 and 90 rpm) | Stationary bicycling → MPSV range from 1.2 (for 175 W, 90 rpm) to 2.1 (for 125 W, 60 rpm); MPSV all conditions, 1.7 |
| Fleming et al8 | Stationary stair climbing; 2 cadences (80 and 112 spm) | Stationary stair climbing → MPSV 2.7 for 80 spm; 2.8 for 112 spm |
| Fleming et al12 | A-P load, internal-external axial torques, and varus-valgus moments during weightbearing and nonweightbearing conditions (with knee at 20°) | Loads during nonweightbearing → MSV −2.0 Loads during weightbearing → MSV 2.1 |
| Fleming et al10 | Extension and flexion of the knee (3 cycles) against controlled resistances (0, 12, and 24 N·m) with and without compressive load | Extension → MPSV 3.1 Flexion → MPSV 1.7 |
| Heijne et al14 | Step-up (3 repetitions) Step-down (3 repetitions) Lunge (3 repetitions) Single-leg sit to stand (3 repetitions) |
Step-up → MPSV 2.5 Step-down → MPSV 2.6 Lunge → MPSV 1.9 Single-leg sit to stand → MPSV 2.8 |
A-P, anterior-posterior; AFE, active flexion-extension; MmSV, mean minimum strain value; MPSV, mean peak strain value; MSV, mean strain value; NA, not applicable; PFE, passive flexion-extension; rpm, revolutions per minute; S-T, slack-taut; spm, steps per minute.
Anterior cruciate ligament strain reported as %.
The common aim of these studies was to measure ACL strain produced during the exercises, for which they all used a displacement transducer. Four studies2,3,7,16 used the Hall effect strain transducer (HEST), while the other 6 studies4,8-10,12,14 used the differential variable reluctance transducer (DVRT) (Table 1). The transducer (HEST or DVRT) was always implanted arthroscopically onto the anteromedial bundle (AMB) of the ACL.
Synthesis of Results
The exercises and conditions investigated are summarized in Table 2 and the Appendix (available at http://sph.sagepub.com/content/by/supplemental-data). Strain measurements are presented as a percentage (Table 2).
Discussion
Isometric quadriceps contraction at 15º of knee flexion produced the greatest ACL strain value (4.4%).2 Isometric contraction of the quadriceps also produced substantial strain values at 30°. From 45° to 60° to positions of greater flexion, this activity did not significantly affect ACL strain.2,3,16 Regarding knee flexion-extension, active motion strained the ACL from 30° to 50° to positions of less flexion, while passive mobilization only strained the ligament when the knee was approaching full extension.2,3
CKC exercises produced strain values similar to those from OKC exercises. Fleming et al12 recorded higher strain during weightbearing conditions than during nonweightbearing conditions. However, the increase of muscle activity, created by applying external weight or resistance, produced increased strain values at OKC concentric extensor exercises2,10 while, on the contrary, strain values did not change significantly when increasing resistance during CKC exercises.4,9 The application of a simulated compressive load10,12 to reproduce a weightbearing condition or CKC exercise obtained the same results: Strain values did not significantly decrease in any case but they did not differ significantly when increasing the resistance with the compressive load. Thus, CKC exercises may protect the ACL when increased rehabilitation resistances are applied. Besides this advantage, CKC exercises may reduce patellofemoral pain,5 enhance knee proprioception,5 and may be more effective for restoring normal knee function, including muscle strength and joint range of motion.13 Individuals who perform predominantly CKC exercises during their rehabilitation also tend to be more satisfied with the end result.15
Limitations
There are a number of limitations to this study that warrant consideration. The studies included in our review investigated healthy ACLs, not reconstructed ligaments. In general, activities that produce high ACL strain would produce similar strain on a properly positioned graft, although some variables associated with reconstructive procedures, such as graft material, tunnel positioning, initial tension applied to the graft, and so on, may influence graft strain responses. Another limitation was that only the AMB of the ACL was investigated. A study of the posterolateral bundle may complement these data. Finally, larger sample sizes would help confirm results in a more precise and generalizable way.
Conclusion
The main finding is that CKC exercises do not produce significantly lower ACL strain than OKC exercises; the strain values produced by both types of exercises are similar. However, the presence of the joint compressive load characteristic of CKC exercises appears to attenuate the strain increase that occurs in OKC exercises when increasing muscle activity as a response to an increased external resistance.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Barry D, Ahmed AM. Design and performance of a modified buckle transducer for the measurement of ligament tension. J Biomech Eng. 1986;108:149-152. [DOI] [PubMed] [Google Scholar]
- 2. Beynnon BD, Fleming BC, Johnson RJ, Nichols CE, Renstrom PA, Pope MH. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med. 1995;23:24-34. [DOI] [PubMed] [Google Scholar]
- 3. Beynnon BD, Howe JG, Pope MH, Johnson RJ, Fleming BC. The measurement of anterior cruciate ligament strain in vivo. Int Orthop. 1992;16:1-12. [DOI] [PubMed] [Google Scholar]
- 4. Beynnon BD, Johnson RJ, Fleming BC, Stankewich CJ, Renstrom PA, Nichols CE. The strain behavior of the anterior cruciate ligament during squatting and active flexion-extension. A comparison of an open and a closed kinetic chain exercise. Am J Sports Med. 1997;25:823-829. [DOI] [PubMed] [Google Scholar]
- 5. Bynum EB, Barrack RL, Alexander AH. Open versus closed kinetic chain exercises after anterior cruciate ligament reconstruction. A prospective randomized study. Am J Sports Med. 1995;23:401-406. [DOI] [PubMed] [Google Scholar]
- 6. Draganich LF, Vahey JW. An in vitro study of anterior cruciate ligament strain induced by quadriceps and hamstrings forces. J Orthop Res. 1990;8:57-63. [DOI] [PubMed] [Google Scholar]
- 7. Fleming BC, Beynnon BD, Nichols CE, Johnson RJ, Pope MH. An in vivo comparison of anterior tibial translation and strain in the anteromedial band of the anterior cruciate ligament. J Biomech. 1993;26:51-58. [DOI] [PubMed] [Google Scholar]
- 8. Fleming BC, Beynnon BD, Renstrom PA, et al. The strain behavior of the anterior cruciate ligament during stair climbing. An in vivo study. Arthroscopy. 1999;15:185-191. [DOI] [PubMed] [Google Scholar]
- 9. Fleming BC, Beynnon BD, Renstrom PA, Peura GD, Nichols CE, Johnson RJ. The strain behavior of the anterior cruciate ligament during bicycling. An in vivo study. Am J Sports Med. 1998;26:109-118. [DOI] [PubMed] [Google Scholar]
- 10. Fleming BC, Ohlén G, Renstrom PA, Peura GD, Beynnon BD, Badger GJ. The effects of compressive load and knee joint torque on peak anterior cruciate ligament strains. Am J Sports Med. 2003;31:701-707. [DOI] [PubMed] [Google Scholar]
- 11. Fleming BC, Oksendahl H, Beynnon BD. Open- or closed-kinetic chain exercises after anterior cruciate ligament reconstruction? Exerc Sport Sci Rev. 2005;33:134-140. [DOI] [PubMed] [Google Scholar]
- 12. Fleming BC, Renstrom PA, Beynnon BD, et al. The effect of weightbearing and external loading on anterior cruciate ligament strain. J Biomech. 2001;34:163-170. [DOI] [PubMed] [Google Scholar]
- 13. Grodski M, Marks R. Exercises following anterior cruciate ligament reconstructive surgery: biomechanical considerations and efficacy of current approaches. Res Sports Med. 2008;16:75-96. [DOI] [PubMed] [Google Scholar]
- 14. Heijne A, Fleming BC, Renstrom PA, Peura GD, Beynnon BD, Werner S. Strain on the anterior cruciate ligament during closed kinetic chain exercises. Med Sci Sports Exerc. 2004;36:935-941. [DOI] [PubMed] [Google Scholar]
- 15. Heijne A, Werner S. Early versus late start of open kinetic chain quadriceps exercises after ACL reconstruction with patellar tendon or hamstring grafts: a prospective randomized outcome study. Knee Surg Sports Traumatol Arthrosc. 2007;15:402-414. [DOI] [PubMed] [Google Scholar]
- 16. Howe JG, Wertheimer C, Johnson RJ, Nichols CE, Pope MH, Beynnon BD. Arthoscopic strain gauge measurement of the normal anterior cruciate ligament. Arthoscopy. 1990;6:198-204. [DOI] [PubMed] [Google Scholar]
- 17. Lysholm M, Messner K. Sagittal plane translation of the tibia in anterior cruciate ligament-deficient knees during commonly used rehabilitation exercises. Scand J Med Sci Sports. 1995;5:49-56. [DOI] [PubMed] [Google Scholar]
- 18. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713-721. [PubMed] [Google Scholar]
- 19. Mikkelsen C, Werner S, Erikson E. Closed kinetic chain alone compared to combined open and closed kinetic chain exercises for quadriceps strengthening after anterior cruciate ligament reconstruction with respect to return to sports: a prospective matched follow-up study. Knee Surg Sports Traumatol Arthrosc. 2000;8:337-342. [DOI] [PubMed] [Google Scholar]
- 20. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151:264-269. [DOI] [PubMed] [Google Scholar]
- 21. Morrissey MC, Hudson ZL, Drechsler WI, Coutts FJ, Knight PR, King JB. Effects of open versus closed kinetic chain training on knee laxity in the early period after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2000;8:343-348. [DOI] [PubMed] [Google Scholar]
- 22. Noyes FR, Mangine RE, Barber S. Early knee motion after open and arthroscopic anterior cruciate ligament reconstruction. Am J Sports Med. 1987;15:149-160. [DOI] [PubMed] [Google Scholar]
- 23. Oh YK, Lipps DB, Ashton-Miller JA, Wojtys EM. What strains the anterior cruciate ligament during a pivot landing? Am J Sports Med. 2012;40:574-583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Shelbourne KD, Nitz P. Accelerated rehabilitation after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1992;15:256-264. [DOI] [PubMed] [Google Scholar]
- 25. Smith MA, Smith WT, Kosko P. Anterior cruciate ligament tears: reconstruction and rehabilitation. Orthop Nurs. 2014;33:14-24. [DOI] [PubMed] [Google Scholar]
- 26. Steadman JR. Rehabilitation of acute injuries of the anterior cruciate ligament. Clin Orthop Relat Res. 1983;172:129-132. [PubMed] [Google Scholar]
- 27. Villa FD, Ricci M, Perdisa F, et al. Anterior cruciate ligament reconstruction and rehabilitation: predictors of functional outcome. Joints. 2016;3:179-185. [DOI] [PMC free article] [PubMed] [Google Scholar]