

Abstract
[Purpose] The purpose of the present study was to investigate the relationship between the external knee adduction moment (KAM) during walking and the biomechanical characteristics of single-leg standing in healthy subjects. [Subjects and Methods] Twenty-eight healthy subjects were recruited for this study. Data were collected while the subjects performed walking and single-leg standing using a motion analysis system with six digital video cameras and two force plates. Pearson’s correlation coefficient was used to quantify the relationship between peak KAM during walking and single-leg standing. To determine whether the kinematic behavior of the pelvis and trunk during single-leg standing are associated with peak KAM during walking, Pearson’s correlation coefficients were calculated and stepwise linear regression was performed. [Results] The peak KAM during single-leg standing was significantly correlated with that during walking. The peak KAM during walking was significantly correlated with the peak lateral lean of the trunk and the peak lateral tilt of the pelvis during single-leg standing. The results of stepwise linear regression analysis show the peak KAM during walking was partially explained by the peak lateral lean of the trunk during single-leg standing. [Conclusion] Our findings suggest that single-leg standing might be a useful method for predicting the peak KAM during walking.
Key words: External knee adduction moment, Gait analysis, Single-leg standing
INTRODUCTION
The external knee adduction moment (KAM) during walking is used as a surrogate for load on the knee joint1), and its association with knee osteoarthritis (OA) has been discussed in many previous studies2,3,4,5,6). Miyazaki et al. examined the relationship between KAM at baseline and the progression of knee OA at a 6 year follow up in patients with medial compartment knee OA, and concluded that KAM could predict radiographic OA progression7). KAM is also associated with tibial cartilage size8), osteoarthritis biomarkers9) and cartilage degenerative changes observed in magnetic resonance imaging10). Other studies have reported a positive correlation between KAM and knee pain11,12,13). Therefore, a reduction of KAM during walking is an important goal for conservative interventions for knee OA.
Mündermann et al. stated that patients with severe knee OA lack the hip abductor muscle strength required to maintain the position of the trunk during the stance phase of walking14). They suggested that weak hip abductor muscle strength led to lateral movement of the trunk away from the support limb, resulting in higher KAM. Takacs et al. reported that contralateral pelvis drop and lateral trunk lean toward the swing limb side increase KAM during single-leg standing15). In addition, other studies have shown a reduction in KAM during walking due to lateral lean of the trunk toward the stance limb side16,17,18). All of these studies indicate that pelvic tilt and trunk lean in the frontal plane are associated with KAM.
Single-leg standing is used to assess movement of the pelvis and trunk in the frontal plane, such as in the Trendelenburg test. As KAM is affected by pelvic tilt and trunk lean in the frontal plane, the single-leg standing task is likely to be an effective and convenient assessment of KAM during walking, and might be useful as a treatment strategy for the reduction of KAM during walking. However, it remains unknown whether kinematics and KAM during single-leg standing reflect KAM during walking. The purpose of the present study was to investigate the relationship between KAM during walking and the biomechanical characteristics of single-leg standing in healthy subjects. We hypothesized that (1) KAM during single-leg standing is correlated with KAM during walking, and that (2) trunk lean and pelvic tilt during single-leg standing are correlated with KAM during walking.
SUBJECTS AND METHODS
Twenty-eight healthy subjects (15 males and 13 females) were recruited for this study. Their age, height and weight were 23.6 ± 4.0 years, 165.9 ± 8.5 cm and 57.1 ± 7.1 kg, respectively (mean ± SD). None of the subjects had a history of a musculoskeletal or neurological disorder. A written informed consent was obtained from each subject prior to their inclusion in this study, and ethical approval was obtained from the Faculty of Health Sciences of Hokkaido University.
While barefoot, the subjects performed walking and single-leg standing tasks which were recorded using a 3D motion analysis system. Each participant completed a minimum of three successful trials, sequentially, of each task. The Helen Hays marker set was used, with additional markers placed on the spinous processes of T2. The data for calculating the kinematics and kinetics of the leg, pelvis and trunk were collected using EVaRT 4.3.57 (Motion Analysis Corporation, Santa Rosa, CA, USA) software and a motion analysis system with six digital cameras (Hawk cameras, Motion Analysis Corporation, Santa Rosa, CA, USA) and two force plates (Kistler, Winterthur, Switzerland) that were synchronized and sampled data at 200 Hz and 1,000 Hz, respectively. The trajectories of markers were filtered with a low-pass fourth-order Butterworth filter with a cutoff frequency of 12 Hz. For the walking task, subjects walked at a self-selected speed along a 10-m walkway. Data were recorded during the stance phase of the dominant leg. In the single-leg standing trial, subjects stood on two force platforms in their natural stance position. They were instructed to lift their non-dominant leg off the force plate as fast as possible following an auditory cue, and to hold this posture for about 3 s. Subjects were instructed to lift the foot by slightly bending their knee and hip joints, and to maintain their trunk in a neutral position as much as possible. The onset of lift-off was defined as the time when the vertical component of the ground reaction force fell below 10 N. Data were recorded from the auditory cue until 1,000 ms after the onset of lift-off.
Based on inverse dynamics, the peak KAM during walking and single-leg standing were calculated from the kinematic and kinetic data using SIMM 6.0.2 (MusculoGraphics Inc., Santa Rosa, CA, USA) software. The KAM was normalized to body weight and height (Fig. 1a, b). The peak lateral lean of the trunk and lateral tilt of the pelvis during single-leg standing were calculated using custom-written code in Matlab 2009b (MathWorks, Natick, MA, USA). Pelvic tilt was defined as the angle formed by the line that connects the two anterior superior iliac spine markers and the horizontal axis; contralateral pelvic elevation was denoted as a positive angle (Fig. 2a). Trunk lean was defined as the angle formed by the line that connected the T2 and sacral markers and the vertical axis. Trunk lean toward the stance limb side was denoted as a positive angle (Fig. 2b). All angles were expressed relative to the static standing position.
Fig. 1.

a) Peak KAM during walking, b) Peak KAM during single-leg standing. Time 0 indicates the onset of lift-off of the swing limb.
Fig. 2.
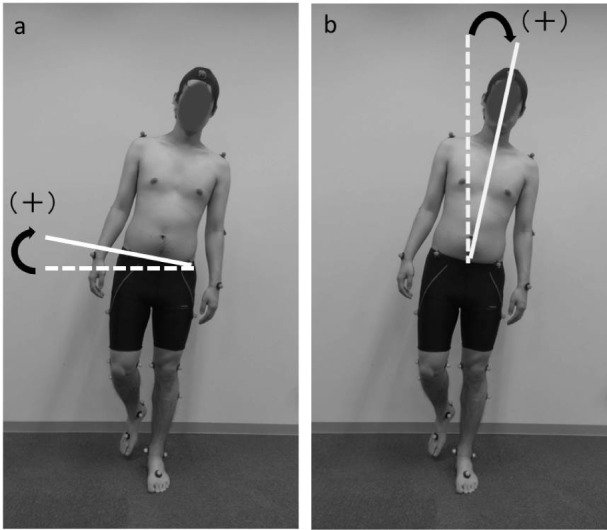
a) Pelvic tilt. Contralateral pelvic elevation was denoted as a positive angle. b) Trunk lean. Trunk lean toward the stance limb side was denoted as a positive angle.
Pearson’s correlation coefficient was used to quantify the relationship between peak KAM during walking and peak KAM during single-leg standing. Pearson’s correlation coefficients were also used to quantify the relationship between peak KAM during walking and the kinematic behavior of the pelvis and trunk during single-leg standing. Stepwise linear regression was performed to determine whether the kinematic behavior of the pelvis and trunk during single-leg standing is associated with peak KAM during walking. The dependent variable was peak KAM during walking. Independent variables were the peak lateral lean of the trunk and the peak lateral tilt of the pelvis during single-leg standing. All statistical analysis was performed using IBM SPSS Statistics 18 software (IBM, Chicago, IL, USA) and a level of significance of 0.05.
RESULTS
The mean and SD of the outcome measures are shown in Table 1. The peak KAM during single-leg standing was significantly correlated with that of walking (r=0.40, p=0.03). The peak KAM during walking was significantly correlated with the peak lateral lean of the trunk during single-leg standing (r=−0.45, p=0.02), and the peak lateral tilt of the pelvis during single-leg standing (r=−0.40, p=0.04). The results of the stepwise linear regression analysis are shown in Table 2. The peak KAM during walking was partially explained by the peak lateral lean of the trunk during single-leg standing (p=0.02).
Table 1. The mean and SD of the outcome measures.
| Mean | SD | |
|---|---|---|
| KAM during walking (Nm/Bw*Ht) | 0.36 | 0.08 |
| KAM during singe-leg standing (Nm/Bw*Ht) | 0.19 | 0.05 |
| Trunk lean (°) a | 3.99 | 1.62 |
| Pelvic tilt (°)b | 7.01 | 2.30 |
aMaximum value of lateral lean angle of the trunk during single-leg standing
bMaximum value of lateral tilt angle of the pelvis during single-leg standing
Table 2. Regression models for predicting the peak KAM during walking.
| Dependent variable | Independent variable | Unstandardized coefficient (95%CI) | Standardized coefficient (β) | Adjusted R2 |
|---|---|---|---|---|
| KAM during walking | Trunk leana | −0.02 (−0.038 to −0.004) | −0.45 | 0.17 |
CI: confidence interval. aMaximum value of lateral lean angle of the trunk during single-leg standing
DISCUSSION
The purpose of the present study was to investigate the relationship between peak KAM during walking and the biomechanical characteristics of single-leg standing. The results of this study show that the peak KAM during single-leg standing and peak KAM during walking are correlated with each other, and that the kinematic behavior of the pelvis and the trunk during single-leg standing are related to peak KAM during walking.
Kim et al. reported that KAM during 3-s static single-leg standing was greater in patients with knee OA than in age-matched healthy sbjects19). They also reported that there was a significant correlation between KAM and scores on the pain and physical function subscales of the Western Ontario and McMaster Universities Osteoarthritis Index20). Thus, they concluded that single-leg standing may be useful in the selection of patients for surgery and for evaluating various treatment modalities for knee OA. However, it was not known if KAM during single-leg standing reflects peak KAM during walking. Our findings indicate that peak KAM during single-leg standing reflects peak KAM during walking, and this result supports previous conclusions.
Previous studies have reported that KAM during walking is affected by trunk lean16,17,18, 21) and pelvic tilt22). KAM is primarily the product of the ground reaction force vector in the frontal plane and the distance between the ground reaction force and the knee joint center in the frontal plane21). The ground reaction force vector depends on the position of the center of mass. Lateral lean of the trunk toward the stance limb and elevation of the contralateral pelvis shifts the center of mass toward the knee joint center, reducing the lever arm distance, consequently reducing the KAM. In the present study, the large contralateral pelvic elevation and lateral trunk lean toward the stance limb side during single-leg standing were found to be correlated with peak KAM during walking. Additionally, the results of the regression analysis indicate that lateral trunk lean toward the stance limb side during single-leg standing partially explained the peak KAM during walking. It appears that the movements of the pelvis and the trunk, to reduce the lever arm in the single-leg standing task, reflect the kinematic behavior, and consequently the KAM, during walking. Based on these findings, the magnitude of the lateral lean of the trunk and tilt of the pelvis during single-leg standing should be assessed as one of the predictors of the magnitude of peak KAM during walking.
The present study showed that peak KAM during walking is related to peak KAM in single-leg standing, and that pelvic tilt and the trunk lean during single-leg standing are related to peak KAM during walking. These findings suggest that single-leg standing might be a useful method for predicting the peak KAM during walking. In recent years, the importance of strengthening the hip abductor muscle for patients with knee OA has been emphasised by some investigators14, 22). However, Bennell et al. conducted a randomized controlled trial and found that hip strengthening did not affect the KAM during walking23). They noted that a motor control program incorporating eccentric hip abductor training in the single-leg stance and co-ordination during functional activities was more effective at achieving a reduction in KAM during walking. To our knowledge, the present study has been the first to demonstrate the relationship between the biomechanical characteristics of single-leg standing and KAM during walking. An intervention trial should be conducted in order to confirm the effect of the motor control program using single-leg standing.
There were a few limitations to this study. First, participants in this study were healthy subjects. We recruited healthy subjects to investigate the biomechanical relationship between single-leg standing and gait without the influence of pain and motor dysfunctions. Future studies should investigate individuals with knee OA. Second, the correlations in this study were moderate. Because there are many other factors that influence KAM during walking, e.g., walking speed24), toe-out angle25, 26), and varus alignment27), it appears not to have exhibited a strong correlation. For clinical application of the results of this study, the influence of these other factors should be considered.
REFERENCES
- 1.Prodromos CC, Andriacchi TP, Galante JO: A relationship between gait and clinical changes following high tibial osteotomy. J Bone Joint Surg Am, 1985, 67: 1188–1194. [PubMed] [Google Scholar]
- 2.Baliunas AJ, Hurwitz DE, Ryals AB, et al. : Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthritis Cartilage, 2002, 10: 573–579. [DOI] [PubMed] [Google Scholar]
- 3.Thorp LE, Sumner DR, Block JA, et al. : Knee joint loading differs in individuals with mild compared with moderate medial knee osteoarthritis. Arthritis Rheum, 2006, 54: 3842–3849. [DOI] [PubMed] [Google Scholar]
- 4.Cho Y, Kim M, Lee W: Effect of proprioceptive training on foot posture, lower limb alignment, and knee adduction moment in patients with degenerative knee osteoarthritis: a randomized controlled trial. J Phys Ther Sci, 2015, 27: 371–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ota S, Kano R, Fukuta S, et al. : Does decrease of the thoracic kyphosis influence decrease knee adduction moment during gait? A preliminary study of a healthy population. J Phys Ther Sci, 2015, 27: 3077–3079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sawada T, Kito N, Yukimune M, et al. : Biomechanical effects of lateral and medial wedge insoles on unilateral weight bearing. J Phys Ther Sci, 2016, 28: 280–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Miyazaki T, Wada M, Kawahara H, et al. : Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis, 2002, 61: 617–622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Creaby MW, Wang Y, Bennell KL, et al. : Dynamic knee loading is related to cartilage defects and tibial plateau bone area in medial knee osteoarthritis. Osteoarthritis Cartilage, 2010, 18: 1380–1385. [DOI] [PubMed] [Google Scholar]
- 9.Hunt MA, Pollock CL, Kraus VB, et al. : Relationships amongst osteoarthritis biomarkers, dynamic knee joint load, and exercise: results from a randomized controlled pilot study. BMC Musculoskelet Disord, 2013, 14: 115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morgenroth DC, Medverd JR, Seyedali M, et al. : The relationship between knee joint loading rate during walking and degenerative changes on magnetic resonance imaging. Clin Biomech (Bristol, Avon), 2014, 29: 664–670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thorp LE, Sumner DR, Wimmer MA, et al. : Relationship between pain and medial knee joint loading in mild radiographic knee osteoarthritis. Arthritis Rheum, 2007, 57: 1254–1260. [DOI] [PubMed] [Google Scholar]
- 12.Kito N, Shinkoda K, Yamasaki T, et al. : Contribution of knee adduction moment impulse to pain and disability in Japanese women with medial knee osteoarthritis. Clin Biomech (Bristol, Avon), 2010, 25: 914–919. [DOI] [PubMed] [Google Scholar]
- 13.Henriksen M, Aaboe J, Bliddal H: The relationship between pain and dynamic knee joint loading in knee osteoarthritis varies with radiographic disease severity. A cross sectional study. Knee, 2012, 19: 392–398. [DOI] [PubMed] [Google Scholar]
- 14.Mündermann A, Dyrby CO, Andriacchi TP: Secondary gait changes in patients with medial compartment knee osteoarthritis: increased load at the ankle, knee, and hip during walking. Arthritis Rheum, 2005, 52: 2835–2844. [DOI] [PubMed] [Google Scholar]
- 15.Takacs J, Hunt MA: The effect of contralateral pelvic drop and trunk lean on frontal plane knee biomechanics during single limb standing. J Biomech, 2012, 45: 2791–2796. [DOI] [PubMed] [Google Scholar]
- 16.Mündermann A, Asay JL, Mündermann L, et al. : Implications of increased medio-lateral trunk sway for ambulatory mechanics. J Biomech, 2008, 41: 165–170. [DOI] [PubMed] [Google Scholar]
- 17.Hunt MA, Simic M, Hinman RS, et al. : Feasibility of a gait retraining strategy for reducing knee joint loading: increased trunk lean guided by real-time biofeedback. J Biomech, 2011, 44: 943–947. [DOI] [PubMed] [Google Scholar]
- 18.Simic M, Hunt MA, Bennell KL, et al. : Trunk lean gait modification and knee joint load in people with medial knee osteoarthritis: the effect of varying trunk lean angles. Arthritis Care Res (Hoboken), 2012, 64: 1545–1553. [DOI] [PubMed] [Google Scholar]
- 19.Kim WY, Richards J, Jones RK, et al. : A new biomechanical model for the functional assessment of knee osteoarthritis. Knee, 2004, 11: 225–231. [DOI] [PubMed] [Google Scholar]
- 20.Bellamy N, Buchanan WW, Goldsmith CH, et al. : Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol, 1988, 15: 1833–1840. [PubMed] [Google Scholar]
- 21.Hunt MA, Birmingham TB, Bryant D, et al. : Lateral trunk lean explains variation in dynamic knee joint load in patients with medial compartment knee osteoarthritis. Osteoarthritis Cartilage, 2008, 16: 591–599. [DOI] [PubMed] [Google Scholar]
- 22.Chang A, Hayes K, Dunlop D, et al. : Hip abduction moment and protection against medial tibiofemoral osteoarthritis progression. Arthritis Rheum, 2005, 52: 3515–3519. [DOI] [PubMed] [Google Scholar]
- 23.Bennell KL, Hunt MA, Wrigley TV, et al. : Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: a randomised controlled trial. Osteoarthritis Cartilage, 2010, 18: 621–628. [DOI] [PubMed] [Google Scholar]
- 24.Robbins SM, Maly MR: The effect of gait speed on the knee adduction moment depends on waveform summary measures. Gait Posture, 2009, 30: 543–546. [DOI] [PubMed] [Google Scholar]
- 25.Guo M, Axe MJ, Manal K: The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture, 2007, 26: 436–441. [DOI] [PubMed] [Google Scholar]
- 26.Lynn SK, Kajaks T, Costigan PA: The effect of internal and external foot rotation on the adduction moment and lateral-medial shear force at the knee during gait. J Sci Med Sport, 2008, 11: 444–451. [DOI] [PubMed] [Google Scholar]
- 27.Wada M, Maezawa Y, Baba H, et al. : Relationships among bone mineral densities, static alignment and dynamic load in patients with medial compartment knee osteoarthritis. Rheumatology (Oxford), 2001, 40: 499–505. [DOI] [PubMed] [Google Scholar]