

Abstract
This study assessed the incremental utility of emotion reactivity and emotion regulation in relation to non-suicidal self-injury (NSSI). Participants included 379 college students aged 18-22 who completed self-report measures of emotion regulation, emotion reactivity, and NSSI. Emotion regulation was significantly related to NSSI both ignoring and controlling for reactivity, but the reverse was not true. Participants' use of NSSI for affect regulation appeared to moderate this relation. Findings support emotion regulation deficits as a target for intervention over-and-above heightened emotion reactivity, especially in those who use NSSI to regulate negative affect.
Keywords: Emotional regulation, self-injurious behavior, emotion reactivity, NSSI
Introduction
Non-suicidal self-injury (NSSI) refers to the intentional destruction of body tissue without the intent to die and is distinct from socially condoned behaviors such as tattooing or piercing (Nock, 2010). The prevalence of NSSI, particularly among adolescents and young adults, is high; yet few empirically-supported treatments exist for this behavior, and much work is needed to understand mechanisms of change that underlie the few interventions that do exist (Muehlenkamp, 2006; Swannell, Martin, Page, Hasking, & St. John, 2014). Growing evidence suggests a major function of the behavior is affect regulation. Clarifying how specific emotional vulnerabilities relate to NSSI may help researchers identify important targets for interventions. The present study examines both unique and incremental relations of emotion regulation and emotion reactivity to NSSI.
Recent work estimated the lifetime prevalence of NSSI in young adults at 13.4%, with slightly higher rates among college students (Swannell, Martin, Page, Hasking, & St. John, 2014). Across age, the behavior is related to depressive and anxiety disorders (Jacobson & Gould, 2007), externalizing disorders, substance abuse (e.g., Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006), and disordered eating (e.g., Svirko & Hawton, 2007). Other work has linked NSSI and risk of suicidality (e.g., Hamza & Willoughby, 2013), although the precise mechanisms of this link remain unclear (e.g., Hamza, Stewart, & Willoughby, 2012). Emotion reactivity and emotion regulation are both implicated in the etiology and maintenance of NSSI. Emotion reactivity typically refers to one's threshold for an emotional response, the intensity of one's experienced emotions, and the duration of one's emotional response (Davidson, 1998). Emotion reactivity thus refers to characteristics of an emotional experience independent of one's deliberate efforts to modulate that experience. Although emotion reactivity measures exist, no particular instrument has been shown to be superior. Consequently, we obtained multiple measures of the emotion reactivity.
Definitions of emotion regulation vary. Gratz and Roemer (2004) described four main dimensions of the construct: awareness of emotions, acceptance of emotions, control of impulsive behaviors when emotional, and access to strategies to modulate one's emotions. Theirs is an explicitly evaluative conceptualization, and the authors note its similarity to others' definitions of emotional competence (e.g., Saarni, 1999). In contrast, Gross's (1998) definition emphasizes processes people use to influence the timing and content of their emotions, along with the experience and expression of these emotions. According to his view, such efforts may be controlled or automatic; further, they can occur as early in the process as the appraisal of emotional cues or as late as during the production of a response. Which aspect or definition of emotion regulation has greater relevance for NSSI is unclear. In the current study, we administered multiple measures of emotion regulation. In this, we do not assume that all measures necessarily represent exactly the same thing; instead, we assume that collectively, they comprehend all aspects of the underlying construct.
Although we regard the constructs of emotion reactivity and regulation as distinct, we recognize conceptual linkages between them. This is particularly true when one considers the emotion regulation processes that Gross (1998) refers to as unconscious or automatic. At this level, it may not be possible (or even relevant) to distinguish between the intensity or speed of an emotional response and automatic regulation efforts. As such, we focus here on the conscious experience of emotion regulation, which we view as distinct from the initial characteristics (e.g., intensity) of an emotional experience. This is consistent with theoretical models of NSSI that implicate both emotion reactivity and emotion regulation in the etiology of NSSI. For example, Chapman, Gratz, and Brown (2006) proposed an Experiential Avoidance Model in which NSSI serves as a negative reinforcement strategy, allowing individuals to escape “unwanted internal experiences” (p.374). They theorized that experiencing more intense emotions, along with diminished capacity to regulate these emotions, contributes to risk for NSSI. Similarly, Nock (2010) hypothesized that high levels of emotion arousal and deficits in emotion regulation combine to form a general vulnerability for NSSI. These models share an emphasis on increased negative emotion reactivity and deficits in emotion regulation. As such, understanding the incremental utility of each construct, or how it relates to NSSI relative to the other construct, is an important goal for developing parsimonious theories and optimal interventions (Haynes & Lench, 2003). Consequently, we examined both the unique relation of emotion regulation to NSSI while controlling for emotion reactivity, and the unique relation of emotion reactivity to NSSI while controlling for emotion regulation.
Empirical work on NSSI supports the theoretical emphases on emotion regulation and reactivity. According to Klonsky (2007), individuals often engage in NSSI to regulate negative emotions, specifically to “alleviate acute negative affect or aversive affective arousal” (p. 229). In his review, Klonsky (2007) found that participants from 13 different clinical samples self-reported emotion regulation as a primary motivation for NSSI. Studies among non-clinical samples show similar findings. Whitlock et al. (2011) examined NSSI behavior and its functions in 11,529 college students in the United States. Among those who reported NSSI, 81% endorsed emotion regulation as one of its functions. In other studies of university students, affect regulation, coping or alleviating mental distress were the most commonly cited motivations for the behavior, and such motivations were related to increased NSSI frequency (Martin, et al., 2013; Saraff, Trujillo, & Pepper, 2015;Weinberg & Klonsky, 2012; Wilcox et al., 2012).
Several studies have examined the individual contributions of either emotion regulation or emotion reactivity to NSSI in university samples, a population containing older adolescents and young adults with elevated rates of the behavior. For example, Gratz and Roemer (2004, 2008) found that overall deficits in emotion regulation significantly discriminated between college students who self-injured and those who did not. Similar findings have emerged from other samples of university students (e.g., Brickman, Ammerman, Look, Berman, & McCloskey, 2014; Franklin, Aaron, Arthur, Shorkey, & Prinstein, 2012; Heath, Toste, Nedecheva, & Charlebois, 2008; Muehlenkamp, Kerr, Bradley, & Adams Larsen, 2010). Hamza and Willoughby (2013) observed a relation between overall emotion regulation deficits and NSSI only among those with severe NSSI; however; this discrepancy may be due to differing levels of severe NSSI behaviors across these samples. Research on emotion regulation deficits and NSSI among college students has also shown that this constructs mediates the relation between body image and NSSI and between NSSI and pain tolerance (Dugan, Toste, & Heath, 2013; Franklin, et al., 2012).
Fewer studies have examined how specific emotion regulation strategies relate to NSSI. Hasking, Momeni, Swannell, and Chia (2008) found that university students with a history of NSSI reported significantly greater use of behavioral disengagement strategies and substance abuse and less use of active coping strategies in comparison to non-self-injurers. Williams and Hasking (2010) reported significant positive relations of NSSI to emotional suppression and avoidant-focused coping. Conversely, they also reported significant negative relations between NSSI and cognitive reappraisal, emotion-focused coping, and problem-focused coping. Only emotion-focused coping and avoidant coping remained significantly related to NSSI after controlling for levels of distress and previous psychological diagnosis (Williams & Hasking, 2010). Overwhelmingly though, the literature supports the role of various emotion regulation factors in distinguishing individuals with a history of NSSI from those with no such history.
Emotion reactivity also shows significant relations to NSSI, although results vary by valence and assessment method. Several studies have shown that, among adolescent and university samples, self-injurers score significantly higher on a self-report measure of emotion reactivity than those who do not self-injure (e.g., Glenn, Blumenthal, Klonsky, & Hajcak, 2011; Knorr, Jenkins, & Connor, 2013; Nock, Wedig, Holmberg, & Hooley, 2008). In a sample of undergraduate women, Gratz (2006) used a different measure and identified a relation between NSSI and positive emotion reactivity (in the expected direction); however, no relation emerged between NSSI and either negative or global reactivity. In a follow-up study among undergraduate men, Gratz and Chapman (2007) found no relation between overall reactivity and membership in the self-harming group (vs. no self-harming) and found a negative relation between reactivity and frequency of NSSI behavior among those who self-harmed. Kleiman, Ammerman, Look, Berman, and McCloskey (2014) identified a significant relations between reactivity and NSSI among both men and women in a large, university-based sample. In a longitudinal study, Hamza and Willoughby (2014) reported a relation between NSSI and a composite “internalizing behaviors” variable that included emotion reactivity, although specific effects due to emotion reactivity could not be discerned from the results. In contrast, Franklin, Puzia, Lee, and Prinstein (2014) did not find longitudinal support for a relation between reactivity and NSSI. Physiological evidence of heightened reactivity is mixed. Nock and Mendes (2008) found greater skin conductivity among adolescent self-injurers compared to those who did not self-injure; however, Glenn et al. (2011) found no difference in the magnitude of startle response elicited by emotional images among young adult self-injurers and controls.
Despite evidence for the importance of both emotion reactivity and regulation to NSSI, few studies have examined the two constructs simultaneously to parse their contributions to NSSI. Brickman, Ammerman, Look, Berman, and McCloskey (2014) found significant relations of NSSI to emotion dysregulation but not to affect lability or anger intensity. Their measure of emotion dysregulation was composed of questions that combined affect lability and anger intensity, however, which complicates interpretation of their results. Turner, Chapman, and Layden (2012) found that limited access to emotion regulation strategies, use of suppression, and emotional intensity were related to NSSI among adults in an Internet-based sample who report using the behavior for affect regulation. Results differed for other self-reported functions of the behavior, suggesting that the intended function of NSSI may be an important moderator when evaluating the roles of emotion regulation and reactivity among those who engage in NSSI. However, their study only included individuals with a lifetime history of the behavior, thus precluding conclusions about the importance of either emotion regulation or reactivity to the distinction between people with and without NSSI.
Gratz and Roemer (2008) also found significant relations of both affect intensity and emotion dysregulation to NSSI in a sample of female undergraduates at a commuter university. Gratz and Roemer did not examine specific emotion regulation processes, and it is unclear if the results generalize to other types of samples. Finally, Jenkins and Schmitz (2012) examined the relation of both emotion dysregulation and emotion reactivity to lifetime acts of NSSI in a sample of college students. They found a significant direct effect of emotion dysregulation on NSSI (controlling for reactivity, gender, and affect experienced after the behavior) but mixed results regarding the relation of reactivity to NSSI. These conclusions could be problematic, however, insofar as (1) they used single measures to assess emotion regulation and reactivity without adjusting for reliability, which could bias various parameter estimates in their model (Cole & Preacher, 2014); (2) the reported results emerged after post-hoc model modifications that may have capitalized on chance, and (3) the results derived from a model that did not include a direct path from emotion reactivity to increased lifetime acts of NSSI.
Three broad goals guided the present study. Using multiple measures of both constructs in a university sample of older adolescents and young adults, our first goal was to clarify the individual associations of emotion regulation and emotion reactivity to NSSI. We expected that each set of variables would be correlated with NSSI. Second, we examined the incremental relation of the reactivity measures over and above the regulation measures (and vice versa) in order to assess the unique contribution of each. Finally, given preliminary evidence that the relation of emotion regulation and reactivity to NSSI may vary by self-reported function of the behavior, our third goal was to examine whether use of NSSI as an emotion regulation strategy moderates the relation of emotion regulation and reactivity to the behavior. In addressing these questions, two methodological issues arose. The first was whether to prescreen for NSSI. As factors contributing to behavior onset may differ from those involved in its maintenance, we chose not to prescreen participants for NSSI. This plus our use of a negative binomial hurdle model to analyze the data (see Results) enabled us to distinguish predictors of the presence/absence of NSSI from predictors of the amount/severity of NSSI. The second was selection of an appropriate data analytic model. The decision not to prescreen resulted in highly skewed data distributions. Fortunately, the negative binomial hurdle model accommodates this kind of extreme skewness quite well.
Methods
Participants
The sample consisted of 379 participants recruited from the undergraduate research pool at a mid-sized private university. Average age of participants was 18.62 (SD = .88), and 299 participants were women (79.1%). The sample was moderately diverse: 76.3% Caucasian, 14%, Asian American, and 9.8% African American. (Race/ethnicities were not mutually exclusive.) To assess the contributions of reactivity measures compared to regulation measures on total NSSI, model comparison procedures required equal observations. Thus, seven participants were eliminated from the total sample because they did not have complete data for both the reactivity and regulation measures, leaving 372 participants included in the final analyses.
Measures
Emotion Regulation
We used three measures (yielding 12 subscales) to assess emotion regulation. The Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) assesses how much respondents use cognitive reappraisal or suppression strategies to regulate emotions. The ERQ includes six items regarding participants' use of reappraisal (e.g., “When I want to feel less negative emotion, I change the way I'm thinking about a situation”) and four items about expression suppression (e.g., “I keep my emotions locked up”). Respondents rate their agreement with each statement on a 1 (strongly disagree) to 7 (strongly agree) Likert scale. In validation studies among undergraduates, Cronbach's alphas averaged .79 and .73 for the reappraisal and suppression scales, respectively, and test-retest reliability for each scale was .69 (Gross & John, 2003). In the current study, Cronbach's alpha for both subscales was .83.
The Regulation of Emotions Questionnaire (REQ; Phillips & Power, 2007) consists of 19 examples of possible emotion regulation techniques. Respondents are asked to rate the frequency with which they use each technique on a 1 (not at all) to 5 (always) scale. Factor analysis by Phillips and Power (2007) revealed four factors: internal-dysfunction regulation strategies (e.g., “I keep the feeling locked up inside”), internal-functional regulation strategies (e.g., “I put the situation into perspective”), external-dysfunction strategies (“I bully other people”), and external-functional strategies (“I ask others for advice”). We dropped one item from the internal dysfunctional scale (“I harm or punish myself in some way”) because of its potential confounding with our dependent variable, NSSI. Among participants ages 12-19, Phillip and Powers reported Cronbach's alphas for scales that ranged from .66 to .76. In our sample, Cronbach's alphas were .63 for both internal dysfunctional and internal functional scales, .65 for the external dysfunctional scale, and .54 for the external functional scale.
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) is a 36-item questionnaire assessing deficits in emotion regulation. Many of the items begin with the stem “When I'm upset…,” and respondents indicate the extent to which a particular behavior or cognition is true for them, using a 1 (almost never) to 5 (almost always) scale. The instrument was validated in an undergraduate sample and produces six subscales: nonacceptance of emotional responses (e.g., “…I feel ashamed of myself for feeling that way”), difficulties in engaging in goal-directed behaviors (e.g., “…I have difficulty focusing on other things”), impulse control difficulties (e.g., “…I have difficulty controlling my behaviors”), lack of emotional awareness (e.g., “I pay attention to my feelings,” reversed scored), limited access to emotion regulation strategies (e.g., “…I believe that I'll end up feeling very depressed”), and lack of emotional clarity (e.g., “…I have difficulty making sense out of my feelings”). Higher scores indicate greater difficulties in each area. Gratz and Roemer (2004) found that Cronbach's alphas for all scales exceeded .80 and that the instrument showed excellent test-retest reliability. In our sample, alphas for the six subscales were .92, .91, .84, .76, .90, and .85, respectively.
Emotion Reactivity
We selected three measures (yielding six subscales) to assess emotion reactivity. The Emotion Reactivity Scale (ERS; Nock, Wedig, Holmberg, & Hooley, 2008) instructs respondents to consider how they experience emotion (no particular emotion specified). Participants then rate their agreement with 21 statements on a 1 (not at all like me) to 5 (completely like me) scale. The ERS assesses three areas of emotion reactivity: how readily individuals react, the intensity of arousal, and the duration of response. Factor analysis indicates that although these areas can each be regarded as a separate factor, the ERS is best understood as consisting of a single factor of overall reactivity (Nock et al., 2008). An example item is “I tend to get very emotional very easily.” The ERS showed high internal consistency in an adolescent validation sample (Cronbach's alpha = .94), and the scale has been used successfully in studies of college-age participants (Glenn et al., 2011). Cronbach's alpha in our sample was .92.
The Affect Intensity and Reactivity Measure Adapted for Youth (AIR-Y; Jones, Leen-Feldner, Olatunji, Reardon, & Hawks, 2009) is a 40-item measure assessing respondents' perceptions of how strongly they experience emotions. The scale was adapted from the Affect Intensity Measure (Larsen, 1984) by simplifying the vocabulary. Respondents rate their agreement with statements about physical, cognitive, and affective components of emotion, using a 1 (never) to 6 (always) scale. Factor analysis revealed a three-factor structure for the AIM (Bryant, Yarnold, & Grimm, 1986): Positivity (how intensely and readily participants feel positive affect; e.g., “When I'm happy, I feel like I'm bursting with joy”), Negative Reactivity (how readily participants feel negative affect; e.g., “Sad movies deeply touch me”), and Negative Intensity (how intensely participants feel negative affect; e.g., “My feelings tend to be stronger compared to most people”). In an adolescent community sample, Cronbach's alphas for these scales were .90, .70, and .73, respectively (Jones et al., 2009). In our sample, alpha was .89 for Positivity and .62 for both Negative Intensity and Negative Reactivity.
The Emotional Intensity Scale (EIS; Bacharowski & Braaten, 1994) is a 30-item measure assessing intensity of emotional experiences. Respondents imagine themselves in 14 positive situations (e.g., “Something wonderful happens to me”) and 16 negative situations (e.g., “People do things to annoy me”). In each, they select one of five responses indicating the intensity with which they would feel the emotion. The EIS was validated in an undergraduate sample and showed strong internal consistency and test-retest reliability (Bacharowski & Braaten, 1994). Cronbach's alpha was .82 for each subscale in our sample.
Non-suicidal self-injury
The Inventory of Statements About Self-Injury (ISAS; Klonsky & Olino, 2008) is a two-part instrument assessing respondents' experiences with NSSI forms and reasons for engaging in the behaviors. The original measure asks respondents how many times they engaged in any of 12 self-harm behaviors. We omitted three behaviors from our analyses (interfering with wound healing, hair pulling, and swallowing dangerous substances) as these may better reflect compulsions or other forms of psychopathology less relevant to NSSI (E.D. Klonsky, personal communication, May 2015). Respondents also report the age at which they began self-harming, the amount of time that typically elapses between urges to self-harm and the act, and whether the individual would like to stop harming themselves. Klonsky and Olino (2008) validated the measure among college students who endorsed at least one lifetime experience with NSSI and found high internal consistency for Part I (Cronbach's alpha = .84) and strong test-retest reliability. Our measure of NSSI as an emotion regulation technique derives from the Part II of the ISAS. This section asks individuals to endorse their reasons for engaging in the self-injurious behaviors on a 0 (not relevant) to 2 (very relevant) scale. It assesses multiple functions of NSSI, using three questions per function (Klonsky & Glenn, 2009). Our primary focus was on the subscale measuring NSSI-as-affect-regulation (Cronbach's alpha for this scale in the present study was .81); however, we report correlations of all subscales with total NSSI.
Procedure
Participants independently completed all questionnaires online using the REDCap electronic data capture system (Harris et al., 2009). Those reporting elevated depressive symptoms and those who endorsed wanting help received referrals to the university counseling center. Participants received course credit in exchange for their participation.
Results
Descriptive Statistics
Table 1 shows descriptive statistics for the nine self-injury types examined here. In all, 24.46% of participants endorsed some form of NSSI over their lifetimes. This is comparable to rates reported in other, similarly-aged samples (Swannell, Martin, Page, Hasking, & St. John, 2014). In our sample, 38.46% of those endorsing NSSI reported episodes within the past year. As Table 1 shows, the sample was fairly heterogeneous with no single behavior endorsed by a majority of participants. Such heterogeneity is somewhat in contrast with other studies among university students, in which one behavior (typically cutting) dominated (e.g., Brickman, Ammerman, Look, Berman, & McCloskey, 2014; Franklin, Aaron, Arthur, Shorkey, & Prinstein, 2012; Glenn, Blumenthal, Klonsky, & Hajcak, 2011). All nine behaviors were summed to generate a total score. As anticipated, this was highly positively skewed (M = 18.65, SD = 89.88, skewness = 8.36, D'Agostino skew test z = 19.77, p < .01, D'Agostino & Pearson, 1973). Table 2 shows means and correlations regarding self-reported functions of NSSI. Affect regulation was the reason that participants most frequently endorsed for engaging in NSSI. NSSI-as-affect-regulation was also significantly correlated with total NSSI. Table 3 shows the descriptive statistics for each reactivity and regulation subscale as well as correlations of the subscales with total NSSI and NSSI-as-affect-regulation. Zero-order correlations between total NSSI and commonly used measures such as the ERS and DERS were slightly smaller (although still significant) than those observed in other samples from a similar population (e.g., Franklin, et al., 2012). Again, this may be due to the heterogeneity of NSSI behaviors observed in our sample. Additionally, we note that the absolute value of zero-order correlations among all regulation and reactivity measures ranged from .01 to .65, with 81% of these correlations falling below .30. This relatively small overlap between the reactivity and regulation measures reinforced our decision to begin by analyzing the contribution of each construct separately.
Table 1. Lifetime prevalence and frequency of NSSI behaviors.
| NSSI Behavior | % Sample Endorsing Behavior | M (SD) |
|---|---|---|
| Pinching | 15.24 | 6.54 (37.27) |
| Banging or hitting self | 13.57 | 1.80 (8.71) |
| Severe scratching | 11.42 | 2.55 (27.16) |
| Cutting | 7.78 | 3.05 (37.13) |
| Biting | 6.94 | 1.72 (13.44) |
| Rubbing skin against rough surface | 4.74 | 3.33 (53.04) |
| Burning | 2.23 | .48 (7.94) |
| Sticking self with needles | 2.23 | 0.11 (0.96) |
| Carving | 0.56 | 0.14 (2.64) |
Note. Response rates vary by question.
Table 2. Self-reported function of NSSI.
| Function | M (SD) | Correlation with total NSSI |
|---|---|---|
| Affect regulation | 2.99 (1.92) | .24* |
| Self-punishment | 2.18 (2.06) | .14 |
| Marking distress | 1.44 (1.63) | -.05 |
| Anti-dissociation | 1.10 (1.70) | .04 |
| Anti-suicide | 0.91 (1.68) | .19 |
| Toughness | 0.66 (1.20) | .05 |
| Interpersonal influence | 0.67 (1.18) | -.09 |
| Interpersonal boundaries | 0.65 (1.31) | -.03 |
| Self-care | 0.57 (0.99) | .16 |
| Sensation seeking | 0.42 (1.00) | .07 |
| Revenge | 0.40 (1.10) | -.11 |
| Autonomy | 0.40 (0.98) | -.12 |
| Peer bonding | 0.29 (0.99) | -.05 |
Note. Correlations calculated as Spearman's rho. Only participants with lifetime histories of NSSI answered these questions. Number of participants responding varied by function, ranging from 89 to 91.
p < .05.
Table 3. Descriptive Statistics for Emotion Regulation and Reactivity subscales and Correlations† with NSSI, NSSI-as–Affect-Regulation.
| Subscale | M (SD) | Correlation with total NSSI (n = 355) | Correlation with NSSI-as-Affect-Regulation (n = 91)a |
|---|---|---|---|
| Emotion Regulation Measures | |||
| ERQ Cognitive Reappraisal | 30.21 (6.23) | -.03 | -.20 |
| ERQ Suppression | 14.67 (5.72) | -.02 | .16 |
| DERS Nonacceptance | 13.74 (5.91) | .11* | .31** |
| DERS Impulse | 10.82 (4.05) | .15** | .18 |
| DERS Strategies | 18.12 (6.68) | .24** | .32** |
| DERS Clarity | 11.35 (3.68) | .04 | .25* |
| DERS Awareness | 14.09 (4.05) | -.03 | .00 |
| DERS Goals | 15.96 (4.87) | .17** | .02 |
| REQ Internal Functional | 17.48 (3.12) | -.10 | -.14 |
| REQ External Dysfunctional | 7.92 (2.69) | .04 | -.03 |
| REQ External Functional | 13.44 (2.96) | -.03 | -.23* |
| REQ Internal Dysfunctional | 11.02 (3.10) | .17** | .17 |
|
| |||
| Emotion Reactivity Measures | |||
| EIS Positive | 50.41 (5.72) | .02 | .13 |
| EIS Negative | 52.94 (7.32) | .08 | .28* |
| AIR-Y Positivity | 3.78 (0.69) | -.02 | .10 |
| AIR-Y Negative Intensity | 3.32 (0.75) | .06 | .32** |
| AIR-Y Negative Reactivity | 4.00 (0.78) | .03 | .35** |
| ERS Total | 30.03 (14.42) | .13* | .24* |
| ERS Sensitivity | 12.86 (7.24) | .10 | .27* |
| ERS Arousal/Intensity | 10.92 (5.50) | .15** | .28** |
| ERS Persistence | 6.27 (3.25) | .11* | .08 |
Note. ERQ=Emotion Regulation Questionnaire; DERS=Difficulties in Emotion Regulation Scale; REQ=Regulation of Emotions Questionnaire; EIS=Emotional Intensity Scale; AIR Y=Affect Intensity and Reactivity Measure for Youth; ERS=Emotion Reactivity Scale
All correlations calculated as Spearman's rho
Participants who did not report NSSI were not included in these statistics.
p < .05,
p < .01.
Count Model Selection
As noted, a major focus of the analyses (conducted using Stata Version 12, StataCorp, 2011, and R, R Core Team, 2014) was to assess the contributions of emotion regulation and emotion reactivity measures to total NSSI. Because the NSSI score that served as the primary dependent measure was in the form of counts, our first task was to identify the most appropriate count data model. Various criteria indicated that a negative binomial hurdle (NBH) model was the optimal approach. Although Poisson regression is the classic analytic model for counts, it often fails to accommodate overdispersion, that is, conditional variances around predicted values that are greater than assumed by the model (for reviews, see Agresti, 2013; Hilbe, 2011, 2014). A commonly recommended alternative is the negative binomial (NB) model which can account for overdispersion via an ancillary variance parameter (Hilbe, 2014). Bounded likelihood ratio chi-square tests indicated that the NB model fit better than the Poisson for both the regulation and reactivity prediction models (ps < .001). Another salient feature of the data, however, was a greater number of zero counts than would be assumed by a standard NB model. To accommodate this, we extended the standard NB model via the NBH model. The latter has two components: a binary logistic regression component that predicts the probability of a 0 vs non-zero (≥ 1) count on the dependent measure and a zero-truncated negative binomial (ZTNB) component that predicts the number of counts using only those participants with non-zero counts. When we assessed models with the regulation predictors, the NBH model fit dramatically better than the standard NB model according to the Akaike Information Criterion (AIC; Akaike, 1973). The AIC adjusts model likelihoods for model complexity, and a 18.52-point difference in AIC values indicated strong support for the NBH, relative to the NB, model (AIC NB = 1308.24, AIC NBH = 1289.72; Hilbe, 2011). Although the difference was less pronounced for the reactivity data (AIC NB = 1301.275, AIC NBH = 1299.99), it still favored the NBH model; furthermore, we deemed it important to use the same structural model for both sets of predictors.1
Effects of Emotion Regulation and Reactivity on NSSI
The emotion regulation set of predictors included the two ERQ subscales, six DERS subscales, and four REQ subscales, as noted in the description of the measures (see Methods). When compared to a null model with no predictors, the set of emotion regulation subscales showed a significant relation to NSSI behaviors (Likelihood Ratio χ2(24) = 50.85, p < .01; adjusted McFadden's R2 = .02). In hurdle models, predictors are evaluated for their contribution to each component (binary vs. count process) of the model. The top portion of Table 4 shows the effect of each regulation subscale on the binary component of the model (i.e., the prediction of at least one NSSI behavior vs. no NSSI behaviors). The bottom portion shows the effects on the count component (i.e., prediction of the number of NSSI behaviors among those who have done so at least once). Within the binary portion, only DERS Strategies showed a statistically significant effect (β = .10, z = 2.77, p = .01). The odds ratio (OR) associated with the coefficient was 1.10, indicating that a one standard-deviation (SD = 6.73) increase in the DERS Strategies score was associated with an almost twofold increase in odds (OR = 1.96) of engaging in at least one NSSI behavior. No individual regulation subscales were significant in the count process portion of the model (see Table 4).
Table 4. Robust Hurdle Regression of Emotion Regulation on NSSI (n=350).
| Emotion regulation subscale | Effect on log(odds) | OR | Robust SE | z |
|---|---|---|---|---|
| Contribution of emotion regulation subscales to binary component of hurdle model | ||||
| 1. ERQ Suppression | -0.03 | 0.97 | 0.03 | -0.99 |
| 2. ERQ Cognitive Reappraisal | 0.04 | 1.05 | 0.02 | 1.97 |
| 3. DERS Impulse | -0.00 | 1.00 | 0.05 | -0.02 |
| 4. DERS Strategies | 0.09 | 1.10 | 0.04 | 2.64** |
| 5. DERS Clarity | -0.05 | 0.96 | 0.05 | -0.99 |
| 6. DERS Goals | 0.02 | 1.02 | 0.04 | 0.53 |
| 7. DERS Awareness | 0.02 | 1.02 | 0.04 | 0.45 |
| 8. DERS Nonacceptance | -0.03 | 0.97 | 0.03 | -0.88 |
| 9. REQ Internal Functional | -0.06 | 0.94 | 0.05 | -1.18 |
| 10. REQ External Dysfunctional | -0.06 | 0.94 | 0.05 | -1.07 |
| 11. REQ External Functional | 0.03 | 1.03 | 0.05 | 0.54 |
| 12. REQ Internal Dysfunctional | 0.07 | 1.07 | 0.06 | 1.24 |
|
| ||||
| Emotion regulation subscale | Effect on log(counts) | IRR | Robust SE | z |
|
| ||||
| Contribution of emotion regulation subscales to positive-count component of hurdle model | ||||
| 1. ERQ Suppression | -0.06 | 2.65 | 0.05 | -1.06 |
| 2. ERQ Cognitive Reappraisal | -0.07 | 0.94 | 0.04 | -1.9 |
| 3. DERS Impulse | 0.04 | 1.04 | 0.05 | 0.88 |
| 4. DERS Strategies | -0.07 | 0.93 | 0.04 | -1.76 |
| 5. DERS Clarity | -0.05 | 0.95 | 0.05 | -1.02 |
| 6. DERS Goals | -0.06 | 0.94 | 0.05 | -1.28 |
| 7. DERS Awareness | 0.07 | 1.08 | 0.06 | 1.33 |
| 8. DERS Nonacceptance | 0.08 | 1.08 | 0.04 | 1.88 |
| 9. REQ Internal Functional | -0.03 | 0.97 | 0.08 | -0.41 |
| 10. REQ External Dysfunctional | -0.11 | 0.90 | 0.07 | -1.57 |
| 11. REQ External Functional | -0.17 | 0.84 | 0.10 | -1.68 |
| 12. REQ Internal Dysfunctional | -0.13 | 0.88 | 0.11 | -1.25 |
Note. Emotion regulation measures: DERS = Difficulties in Emotion Regulation Strategies (Nonacceptance, Impulse, Clarity, Strategies, Goals, Awareness subscales), ERQ = Emotion Regulation Questionnaire (Cognitive reappraisal, Suppression subscales), REQ = Regulation of Emotions Questionnaire (Internal Functional, Internal Dysfunctional, External Functional, External Dysfunctional subscales). Emotion reactivity and intensity measures: ERS = Emotion Reactivity Scale, AIR-Y = Affect Intensity and Reactivity Measure for Youth (Positivity, Negative Intensity, Negative Reactivity subscales), EIS = Emotional Intensity Scale (Positive, Negative subscales). OR = Odds Ratio, IRR = Incidence Rate Ratio
p < .01.
The set of emotion reactivity predictors included three AIR subscales, two EIS subscales, and the ERS.2 In contrast to the emotion regulation subscales, the overall set of emotion reactivity measures did not significantly relate to NSSI behaviors (Likelihood Ratio χ2(12) = 16.60, p = .17), though one individual subscale emerged as significant.3
To compare the relative contributions of emotion regulation and reactivity, we conducted two hierarchical NBH model comparisons. The first entered the set of reactivity predictors in an initial step and evaluated whether adding the set of regulation predictors in a second step significantly enhanced fit. The second model comparison entered the two sets of predictors in the reverse order. Results indicated that the regulation measures significantly enhanced fit when added to the reactivity measures (Likelihood Ratio χ2(24) = 48.01, p < .01). In contrast, the reactivity measures failed to significantly increment relations to NSSI above and beyond the contribution of the regulation measures (Likelihood Ratio χ2(12) = 13.76, p = .32).
Self-reported function of NSSI as a Moderator Variable
An additional aim of the study was to assess whether individual differences in the use of NSSI for affect regulation purposes moderated the relation between NSSI behaviors and regulation and reactivity measures. Given that only the DERS Strategies contributed significant to NSSI in the hurdle analysis, we focused on the DERS Strategies subscale for analyses related to this aim. We used a zero-truncated negative binomial (ZTNB) regression model (Hilbe, 2014) because we were only interested in the participants with non-zero NSSI counts (thus truncating the response variable at zero). The ZTNB model used the conventional log-link function to linearize the relation between the predictors and the NSSI.
In the initial ZTNB model specifying only main effects, neither DERS Strategies nor NSSI as affect regulation showed a significant relation to the number of NSSI behaviors (both ps > 0.50). When added to the model, however, the interaction between DERS-Strategies and NSSI-as-affect-regulation score was significant (β = .05, z = 3.99, p < .01). Figure 1 depicts the interaction, with predicted values of logged total NSSI behaviors plotted as a function of DERS Strategies for three values of NSSI-as-affect-regulation score: the 25th percentile (0), 50th percentile (2), and 75th percentile (4). The pattern of the differences in slopes shows that the relation between NSSI and limited access to emotion regulation strategies (reflected by higher scores on DERS Strategies) was stronger among individuals who reported greater use of NSSI to regulate affect (see Figure 1).
Figure 1.
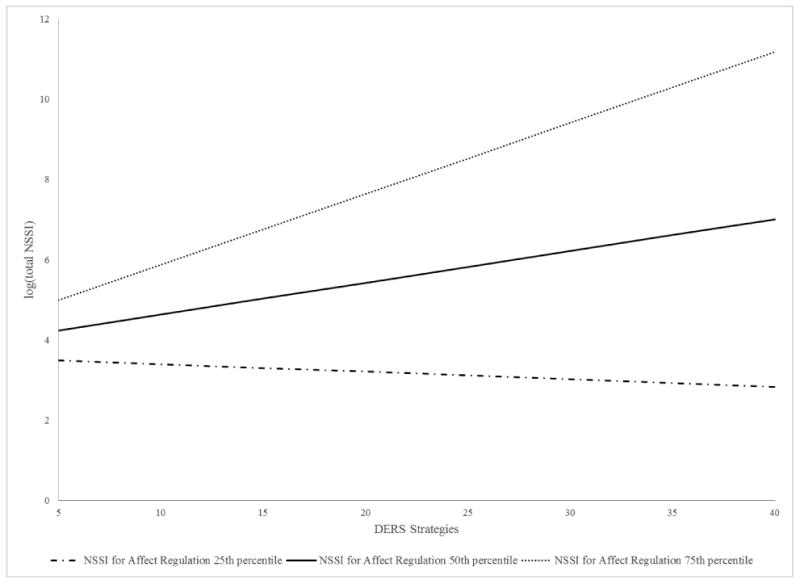
Self-reported use of NSSI to regulate affect moderates the relation between NSSI and DERS Strategies score (reflecting limited access to emotion regulation strategies). Lines represent the NSSI-DERS Strategies relation for those scoring at the 25th, 50th, and 75th percentiles for use of NSSI to regulate affect.
Discussion
The main goal of the study was to disentangle the roles of emotion regulation and reactivity in relation to NSSI. Three major findings emerged. First, a model consisting of 12 emotion regulation subscales (from three distinct measures) was significantly related to NSSI and proved superior to a model consisting of emotion reactivity measures. Second, a set of six emotion reactivity subscales (also from three measures) was not significantly associated with NSSI. Finally, self-reported use of NSSI to regulate one's affect moderated the relation between emotion regulation and the behavior. Results also generated an important question regarding the distinction between emotion regulation and reactivity. Details and clinical implications of these findings appear below.
First, multiple emotion regulation measures, based on different definitions of the construct, collectively showed a significant relation to NSSI and provided significantly greater explanatory power than did emotion reactivity. This finding extends previous work (e.g., Gratz & Roemer, 2004), revealing a significant relation of emotion regulation alone to NSSI. We built upon their work in two ways: (1) we used several measures of emotion regulation, thus representing multiple operationalizations of the construct, and (2) we used a model comparison approach allowing us to pit the incremental contribution of emotion regulation against that of reactivity. Evidence of the incremental importance of emotion regulation over emotion reactivity extends other work as well. Jenkins and Schmitz (2012) found a direct effect of emotion regulation deficits on NSSI when testing a path analytic model of the behavior incorporating both emotion regulation and reactivity (and other covariates). However, the additional covariates and focus on other hypotheses complicate application of their results to our question. Our study explicitly focused on the incremental importance of emotion regulation to NSSI, over and above emotion reactivity. Our use of the NBH model enabled us to conclude that emotion regulation contributes both to the distinction between those who do versus do not report NSSI and to the frequency of NSSI behaviors among those who engage in such behavior. Interestingly, the specific subscale that was significant in the binary (no NSSI vs. any NSSI) portion of the model was not a significant predictor of NSSI frequency. These results echo findings by Riley, Combs, Jordan, and Smith (2015) that a single psychological construct may play differential roles in NSSI initiation versus maintenance.
Our second major finding concerned emotion reactivity. As a block, the set of emotion reactivity measures did not show a significant relation to total NSSI either over and above emotion regulation or entirely ignoring emotion regulation. This is an important finding given that previous studies have been somewhat mixed on the relation of emotion reactivity to NSSI (e.g., Glenn, Blumenthal, Klonsky, & Hajcak, 2011; Kleiman, Ammerman, Look, Berman, & McCloskey, 2014; Knorr, Jenkins, & Connor, 2013; Nock, Wedig, Holmberg, & Hooley, 2008; Turner, Chapman, & Layden, 2012, but see Franklin, Puzia, Lee, & Prinstein, 2014; Gratz & Chapman, 2007). We note that observed effect sizes of individual emotion reactivity measures and NSSI were smaller in our sample compared to previous work (based on effect size benchmarks outlined by Cohen, 1988). Differences in sampling may explain some of the discrepancy. For example, Nock et al. (2008) observed a large effect size differentiating the ERS scores of clinical participants who had self-injured within the past year from non-self-injuring controls. Glenn et al. (2011) reported that medium effect sizes on the ERS subscales differentiated self-injurers from controls recruited from a university, whereas Kleiman et al. (2014) observed small effect sizes in the association of the ERS with self-injury history in a broader university sample. The present sample was most similar to that of Kleiman et al.'s general college student sample, and we observed comparable (small) effect sizes. Collectively, these results might suggest that researchers should place less emphasis on emotion reactivity when studying NSSI in non-clinical samples; however, future research efforts should first seek to confirm whether the relation of emotion reactivity to NSSI varies across different populations.
Taken together, these findings on emotion regulation and reactivity have several implications for theories about NSSI. Chapman et al.'s (2006) theoretical Experiential Avoidance Model of NSSI posits that both high emotional intensity and poor capacity for regulation contribute to risk for NSSI. Nock's (2009) theory described high emotion reactivity as one of several distal factors that predispose the use of NSSI to regulate emotions. The current study is thus highly relevant. One possibility is that emotion regulation is a more proximal predictor of NSSI than is emotion reactivity, as outlined by Nock (2009). Longitudinal research is needed for rigorous tests of such mediational processes, but if true, then theoretical formulations and statistical models should explicitly state some sense of a reactivity → regulation → NSSI indirect causal flow. The second possibility is that the concept of emotion regulation subsumes the concept of emotion reactivity (at least as they are operationalized). Close examination of the emotion regulation measures suggests this could be true. Some measures appear to take emotion reactivity as indirect evidence of failure to regulate. For example, poor emotion regulation is indicated on the Difficulties in Emotion Regulation Scale through items like “When I'm upset, I feel out of control,” which seems to infer that high reactivity implies poor regulation. An important direction for further work would be analyzing the measures themselves to ensure they assess either regulation or reactivity directly and do not use one as an indirect measure of the other.
Our third major finding speaks to the importance of considering an individual's motivation in engaging in NSSI when examining psychological correlates of the behavior. We sought to determine whether use of NSSI as a mechanism for emotion regulation might moderate the relation of emotion regulation deficits to the behavior. Our results showed a stronger relation between NSSI and (limited) emotion regulation strategies for those who reported using NSSI to regulate affect. Due to the cross-sectional nature of the data, we cannot say whether such limited access to regulation strategies predicts use of NSSI to regulate affect or whether individuals who use the behavior for this function also happen to have fewer emotion regulation “tools” on which to draw. If confirmed longitudinally, such results could suggest that instruction in specific emotion regulation strategies may not be universally indicated. Rather, such strategies may be more effective for individuals who report using NSSI for affect regulation. The findings provide an important reminder that NSSI is a multifaceted behavior used for a wide variety of purposes. Bentley, Nock, and Barlow (2014) called for a targeted approach to research on risk factors for NSSI that considers differences in behavior function and personal motivation. Our results affirm that considering individuals' motivations for NSSI in etiological research may reveal important nuances in the behavior.
Limitations of the current study pave the way for future investigation. Our results raise questions about the convergent and discriminant validity of self-report measures of emotion reactivity and regulation. An important next step will be a multitrait-multimethod examination of these constructs. Furthermore, researchers should cross-validate self-report measures against physiological assessments, behavioral measures, or neuroimaging evaluations of emotion reactivity and regulation. We also note the self-report measures used here largely tap individuals' emotion regulation efforts in a general context (i.e., at a trait level). Such assessments may not fully capture how individuals regulate emotions in the timeframe surrounding an NSSI episode. Researchers should consider use of real-time assessment methods to explore regulation efforts immediately preceding and following a self-injury episode (e.g., Nock, Prinstein & Sterba, 2009).
In addition to these concerns, we note that our study was cross-sectional, which precluded examining truly prospective relations. An important direction for future research would be to administer the measures of NSSI, emotional reactivity, and emotional regulation in longitudinal research designs. Second, we only assessed lifetime NSSI. Even though roughly 40% of those who reported the timeframe of their most recent NSSI incident said it occurred within the past year, the relation of NSSI to emotion regulation may be stronger for individuals who have recently engaged in the behavior. Future research might consider recency, frequency, and severity of NSSI behaviors as covariates in statistical models. Third, our sample consisted of college students at an elite university. Even though slightly more than one-quarter of our sample reported having engaged in NSSI, researchers should examine the generalizability of these findings to more diverse populations and to populations in which the incidence of severe NSSI behaviors is even higher and potentially more homogenous.
Despite the limitations, the findings have important clinical and clinical research implications. Emotion regulation, particularly the inability to access strategies to reduce one's negative emotions, consistently emerged as an important correlate of NSSI. Clinicians treating patients who engage in NSSI should consider emotion regulation skills training. Indeed, preliminary evidence suggests dialectical behavior therapy, which explicitly includes such components, may help reduce NSSI incidents (Muehlenkamp, 2006; Pistorello, Fruzzetti, MacLane, Gallop, & Iverson, 2012). An important corollary to these results, however, is that clinicians should take care to thoroughly assess patients' motivations for engaging in NSSI. Interventions such as emotion regulation skills training may be more effective for those who use the behavior specifically for affect regulation purposes. Building these individuals' capacity to use non-NSSI emotion regulation strategies in moments of distress is likely to be crucial to reducing the behavior. As clinical research in this area develops, it will also be critical to examine whether behavioral function impacts the effect of a specific intervention on NSSI.
Acknowledgments
R.L. Zelkowitz and G.T. Han were supported in part from NIMH training grant T32MH018921-26
Footnotes
We also considered the zero-inflated negative binomial (ZINB) model as one that can accommodate a large number of zeros. Like the negative binomial hurdle model, the ZINB model predicts both zero vs. non-zero values and the number of positive counts among those with non-zero data. Results using a ZINB model were consistent with the negative binomial hurdle model: the regulation measures significantly enhanced fit when added to the reactivity measures (Likelihood Ratio χ2(24) = 56.10, p < .01). Again, the reactivity measures failed to contribute significantly to model fit over and above the regulation measures (Likelihood Ratio χ2(12) = 15.13, p = .23). In contrast to the negative binomial hurdle results, several more individual subscales emerged as significant in the ZINB regulation model. For the binary portion, significant subscales included: ERQ Cognitive Reappraisal (β = -0.10, z = -2.50, p = .01), DERS Strategies (β = -0.09, z = -2.16, p = .03), DERS Nonacceptance (β = 0.11, z = 2.34, p = .02), and REQ External Functional (β = -0.28, z = -2.36, p = .02). For the count portion of the model, significant subscales included ERQ Cognitive Reappraisal (β = -0.09, z = -2.45, p = .01) and DERS Strategies (β = -0.16, z = -3.15, p < .01).
Despite the additional significant subscales in the ZINB, we ultimately favored the hurdle model on conceptual grounds. The ZINB model is a mixture model that posits two types of zero scores: sampling and structural zeroes. We did not find this distinction theoretically justified or compelling in the context of NSSI. In addition, hurdle models explicitly reflect the notion that different factors might predict the onset of NSSI (i.e., crossing the “hurdle” from 0 to at least 1) versus the number of NSSI episodes in individuals who do engage in it. This is consistent with the notion that factors predicting the onset of behavior might differ from those predicting its maintenance, severity, and frequency. We thus opted to go with the hurdle model despite its more conservative results regarding the individual subscales.
Although the AIC and BIC statistical comparisons account for the number of predictors in each model, we wanted to rule out the possibility that the emotion regulation model proved superior to the reactivity simply because of the imbalance of predictors (12 in the regulation model vs. six in the reactivity model). Thus, we also conducted an analysis in which we parceled the ERS into its three component subscales: Arousal, Intensity, and Persistence, and dropped all four REQ subscales. This resulted in a model with equal numbers of regulation and reactivity predictors (eight and eight). Results were the same; the regulation model proved superior to a null model (Likelihood Ratio χ2 (16) = 38.97, p < .01), but the reactivity model did not (Likelihood Ratio χ2 (16) = 21.01, p = .18). When examining the relative contributions of emotion regulation and reactivity on NSSI, results indicated that the regulation measures significantly enhanced fit when added to the reactivity measures (Likelihood Ratio χ2(16) = 33.12, p = .01). In contrast, the reactivity measures failed to significantly increment predictions above and beyond the contribution of the regulation measures (Likelihood Ratio χ2(16) = 15.16, p = .51). Importantly, these results are consistent with our comparisons of the 12-predictor regulation model vs. the six-predictor reactivity model.
No individual subscales were significant in the binary portion of the model, but the EIS Negative was significant in the count portion of the model (β = 0.11, z = 2.10, p = .04). This result must be viewed with caution, however, given the overall lack of model fit.
References
- Agresti A. Categorical Data Analysis: 3rd Edition. Hoboken, New Jersey: John Wiley & Sons; 2013. [Google Scholar]
- Akaike H. A new look at the statistical identification model. IEEE Transactions on Automatic Control. 1974;19(6):716–723. [Google Scholar]
- Bachorowski JA, Braaten EB. Emotional intensity: Measurement and theoretical implications. Personality and Individual Differences. 1994;17(2):191–199. http://dx.doi.org/10.1016/0191-8869(94)90025-6. [Google Scholar]
- Bentley KH, Nock MK, Barlow DH. The four-function model of non-suicidal self-injury: Key directions for future research. Clinical Psychological Science, Epub January. 2014;3:2014. doi: 10.1177/2167702613514563. [DOI] [Google Scholar]
- Brickman LJ, Ammerman BA, Look AE, Berman ME, McCloskey MS. The relationship between non-suicidal self-injury and borderline personality disorder symptoms in a college sample. Borderline Personality Disorder and Emotion Dysregulation. 2014:1–14. doi: 10.1186/2051-6673-1-14. http://dx.doi.org/10.1186/2051-6673-1-14. [DOI] [PMC free article] [PubMed]
- Bryant FB, Yarnold PR, Grimm LG. Toward a Measurement Model of the Affect Intensity Measure: A three-factor structure. Journal of Research in Personality. 1996;30(2):223–247. http://dx.doi.org/10.1006/jrpe.1996.0015. [Google Scholar]
- Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: The experiential avoidance model. Behaviour Research and Therapy. 2006;44(3):371–394. doi: 10.1016/j.brat.2005.03.005. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Lawrence Earlbaum Associates; 1988. [Google Scholar]
- Cole DA, Preacher KJ. Manifest Variable Path Analysis: Potentially Serious and Misleading Consequences Due to Uncorrected Measurement Error. Psychological Methods. 2014;19(2):300–315. doi: 10.1037/a0033805. http://dx.doi.org/10.1037/a0033805. [DOI] [PubMed] [Google Scholar]
- D'Agostino RB, Pearson ES. Tests for departure from normality. Biometrika. 1973;60:613–22. [Google Scholar]
- Davidson RJ. Affective style and affective disorders: Perspectives from affective neuroscience. Cognition and Emotion. 1998;12(3):307–330. http://dx.doi.org/10.1080/026999398379628. [Google Scholar]
- Dugan JM, Toste JR, Heath NL. An examination of the relationship between body image factors and non-suicidal self-injury in young adults: The mediating role of emotion dysregulation. Psychiatry Research. 2013;206(2-3):256–264. doi: 10.1016/j.psychres.2012.11.016. http://dx.doi.org/10.1016/j.psychres.2012.11.016. [DOI] [PubMed] [Google Scholar]
- Franklin JC, Aaron RV, Arthur MS, Shorkey SP, Prinstein MJ. Nonsuicidal self-injury and diminished pain perception: the role of emotion dysregulation. Comprehensive Psychiatry. 2012;53(6):691–700. doi: 10.1016/j.comppsych.2011.11.008. http://dx.doi.org/10.1016/j.comppsych.2011.11.008. [DOI] [PubMed] [Google Scholar]
- Franklin JC, Puzia ME, Lee KM, Prinstein MJ. Low Implicit and Explicit Aversion Toward Self-Cutting Stimuli Longitudinally Predict Nonsuicidal Self-Injury. Journal of Abnormal Psychology. 2014;123(2):463–469. doi: 10.1037/a0036436. http://dx.doi.org/10.1037/a0036436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glenn CR, Blumenthal TD, Klonsky ED, Hajcak G. Emotional Reactivity in Nonsuicidal Self-injury: Divergence Between Self-Report and Startle Measures. International Journal of Psychophysiology : Official Journal of the International Organization of Psychophysiology. 2011;80(2):166–170. doi: 10.1016/j.ijpsycho.2011.02.016. http://dx.doi.org/10.1016/j.ijpsycho.2011.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gratz K. Risk factors for deliberate self-harm among female college students: the role and interaction of childhood maltreatment, emotional inexpressivity, and affect intensity/reactivity. American Journal of Orthopsychiatry. 2006;76(2):238–250. doi: 10.1037/0002-9432.76.2.238. http://dx.doi.org/10.1037/0002-9432.76.2.238. [DOI] [PubMed] [Google Scholar]
- Gratz KL, Chapman AL. The role of emotional responding and childhood maltreatment in the development and maintenance of deliberate self-harm among male undergraduates. Psychology of Men & Masculinity. 2007;8(1):1–14. http://dx.doi.org/10.1037/1524-9220.8.1.1. [Google Scholar]
- Gratz KL, Roemer L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment. 2004;26(1):41–54. http://dx.doi.org/10.1023/B:JOBA.0000007455.08539.94. [Google Scholar]
- Gratz KL, Roemer L. The Relationship Between Emotion Dysregulation and Deliberate Self-Harm Among Female Undergraduate Students at an Urban Commuter University. Cognitive Behaviour Therapy. 2008;37(1):14–25. doi: 10.1080/16506070701819524. http://dx.doi.org/10.1080/16506070701819524. [DOI] [PubMed] [Google Scholar]
- Gross JJ. The emerging field of emotion regulation: An integrative review. Review of General Psychology. 1998;2(3):271–299. http://dx.doi.org/10.1037/1089-2680.2.3.271. [Google Scholar]
- Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. Journal of Personality and Social Psychology. 2003;85(2):348–362. doi: 10.1037/0022-3514.85.2.348. http://dx.doi.org/10.1037/0022-3514.85.2.348. [DOI] [PubMed] [Google Scholar]
- Hamza C, Willoughby T. A longitudinal person-centered examination of nonsuicidal self-injury among university students. Journal of Youth and Adolescence. 2014;43(4):671–685. doi: 10.1007/s10964-013-9991-8. [DOI] [PubMed] [Google Scholar]
- Hamza CA, Willoughby T. Nonsuicidal Self-Injury and Suicidal Behavior: A Latent Class Analysis among Young Adults. PLoS ONE. 2013;8(3):e59955. doi: 10.1371/journal.pone.0059955. http://dx.doi.org/10.1371/journal.pone.0059955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamza CA, Stewart SL, Willoughby T. Examining the link between nonsuicidal self-injury and suicidal behavior: a review of the literature and an integrated model. Clinical Psychology Review. 2012;32(6):482–495. doi: 10.1016/j.cpr.2012.05.003. http://dx.doi.org/10.1016/j.cpr.2012.05.003. [DOI] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. http://dx.doi.org/10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasking P, Momeni R, Swannell S, Chia S. The nature and extent of non-suicidal self-injury in a non-clinical sample of young adults. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research. 2008;12(3):208–218. doi: 10.1080/13811110802100957. http://dx.doi.org/10.1080/13811110802100957. [DOI] [PubMed] [Google Scholar]
- Haynes SN, Lench HC. Incremental validity of new clinical assessment measures. Psychological Assessment. 2003;15(4):456–466. doi: 10.1037/1040-3590.15.4.456. http://dx.doi.org/10.1037/1040-3590.15.4.456. [DOI] [PubMed] [Google Scholar]
- Heath NL, Toste JR, Nedecheva T, Charlebois A. An examination of nonsuicidal self-injury among college students. Journal of Mental Health Counseling. 2008;30(2):137–156. [Google Scholar]
- Hilbe JM. Negative binomial regression. New York: Cambridge University Press; 2011. [Google Scholar]
- Hilbe JM. Modeling count data. New York: Cambridge University Press; 2014. [Google Scholar]
- Jacobson CM, Gould M. The epidemiology and phenomenology of non-suicidal self-injurious behavior among adolescents: a critical review of the literature. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research. 2007;11(2):129–147. doi: 10.1080/13811110701247602. http://dx.doi.org/10.1080/13811110701247602. [DOI] [PubMed] [Google Scholar]
- Jenkins AL, Schmitz MF. The roles of affect dysregulation and positive affect in non-suicidal self-injury. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research. 2012;16(3):212–225. doi: 10.1080/13811118.2012.695270. http://dx.doi.org/10.1080/13811118.2012.695270. [DOI] [PubMed] [Google Scholar]
- Jones RE, Leen-Feldner EW, Olatunji BO, Reardon LE, Hawks E. Psychometric properties of the Affect Intensity and Reactivity Measure adapted for Youth (AIR-Y) Psychological Assessment. 2009;21(2):162–175. doi: 10.1037/a0015358. http://dx.doi.org/10.1037/a0015358. [DOI] [PubMed] [Google Scholar]
- Kleiman EM, Ammerman B, Look AE, Berman ME, McCloskey MS. The role of emotion reactivity and gender in the relationship between psychopathology and self-injurious behavior. Personality and Individual Differences. 2014;69:150–155. http://dx.doi.org/10.1016/j.paid.2014.05.021. [Google Scholar]
- Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clinical Psychology Review. 2007;27(2):226–239. doi: 10.1016/j.cpr.2006.08.002. http://dx.doi.org/10.1016/j.cpr.2006.08.002. [DOI] [PubMed] [Google Scholar]
- Klonsky ED, Glenn CR. Assessing the Functions of Non-suicidal Self-injury: Psychometric Properties of the Inventory of Statements About Self-injury (ISAS) Journal of Psychopathology and Behavioral Assessment. 2009;31(3):215–219. doi: 10.1007/s10862-008-9107-z. http://dx.doi.org/10.1007/s10862-008-9107-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klonsky ED, Olino TM. Identifying clinically distinct subgroups of self-injurers among young adults: a latent class analysis. Journal of Consulting and Clinical Psychology. 2008;76(1):22–27. doi: 10.1037/0022-006X.76.1.22. http://dx.doi.org/10.1037/0022-006X.76.1.22. [DOI] [PubMed] [Google Scholar]
- Knorr AC, Jenkins AL, Conner BT. The role of sensation seeking in non-suicidal self-injury. Cognitive Therapy and Research. 2013;37:1276–1284. http://dx.doi.org/10.1007/s10608-013-9554-z. [Google Scholar]
- Larsen RJ. Theory and measurement of affect intensity as an individual difference characteristic. Dissertation Abstracts International. 1984;85:2297B. [Google Scholar]
- Martin J, Cloutier PF, Levesque C, Bureau JF, Lafontaine MF, Nixon MK. Psychometric properties of the functions and addictive features scales of the Ottawa Self-Injury Inventory: a preliminary investigation using a university sample. Psychological Assessment. 2013;25(3):1013–1018. doi: 10.1037/a0032575. http://dx.doi.org/10.1037/a0032575. [DOI] [PubMed] [Google Scholar]
- Muehlenkamp JJ. Empirically supported treatments and general therapy guidelines for non-suicidal self-injury. Journal of Mental Health Counseling. 2006;28(2):166–185. [Google Scholar]
- Muehlenkamp JJ, Kerr PL, Bradley AR, Adams Larsen M. Abuse subtypes and nonsuicidal self-injury: preliminary evidence of complex emotion regulation patterns. The Journal of Nervous and Mental Disease. 2010;198(4):258–263. doi: 10.1097/NMD.0b013e3181d612ab. http://dx.doi.org/10.1097/NMD.0b013e3181d612ab. [DOI] [PubMed] [Google Scholar]
- Nock MK. Why do people hurt themselves? New insights into the nature and function of self-injury. Current Directions in Psychological Science. 2009;18(2):78–83. doi: 10.1111/j.1467-8721.2009.01613.x. http://dx.doi.org/10.1111/j.1467-8721.2009.01613.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK. Self-Injury. Annual Review of Clinical Psychology. 2010;6(1):339–363. doi: 10.1146/annurev.clinpsy.121208.131258. http://dx.doi.org/10.1146/annurev.clinpsy.121208.131258. [DOI] [PubMed] [Google Scholar]
- Nock MK, Joiner TE, Jr, Gordon KH, Lloyd-Richardson E, Prinstein MJ. Non-suicidal self-injury among adolescents: diagnostic correlates and relation to suicide attempts. Psychiatry Research. 2006;144(1):65–72. doi: 10.1016/j.psychres.2006.05.010. http://dx.doi.org/10.1016/j.psychres.2006.05.010. [DOI] [PubMed] [Google Scholar]
- Nock MK, Mendes WB. Physiological arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. Journal of Consulting and Clinical Psychology. 2008;76(1):28–38. doi: 10.1037/0022-006X.76.1.28. [DOI] [PubMed] [Google Scholar]
- Nock MK, Prinstein MJ, Sterba SK. Revealing the form and function of self-injurious thoughts and behaviors: A real-time ecological assessment study among adolescents and young adults. Journal of Abnormal Psychology. 2009;118(4):816–827. doi: 10.1037/a00169480021-843X/09/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK, Wedig MM, Holmberg EB, Hooley JM. The emotion reactivity scale: development, evaluation, and relation to self-injurious thoughts and behaviors. Behavior Therapy. 2008;39(2):107–116. doi: 10.1016/j.beth.2007.05.005. [DOI] [PubMed] [Google Scholar]
- Phillips KFV, Power MJ. A new self-report measure of emotion regulation in adolescents: The Regulation of Emotions Questionnaire. Clinical Psychology & Psychotherapy. 2007;14(2):145–156. http://dx.doi.org/10.1002/cpp.523. [Google Scholar]
- Pistorello J, Fruzzetti AE, MacLane C, Gallop R, Iverson KM. Dialectical Behavior Therapy applied to college students: A randomized clinical trial. Journal of Consulting and Clinical Psychology. 2012;80(6):982–994. doi: 10.1037/a0029096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2014. [Computer Software] [Google Scholar]
- Riley EN, Combs JL, Jordan CE, Smith GT. Negative urgency and lack of perseverance: Identification of differential pathways of onset and maintenance risk in the longitudinal prediction of nonsuicidal self-injury. Behavior Therapy. 2015;46(4):439–448. doi: 10.1016/j.beth.2015.03.002. http:dx.doi.org/10.1016/j.beth.2015.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saarni C. The Development of Emotional Competence. New York: Guilford Press; 1999. [Google Scholar]
- Saraff PD, Trujillo N, Pepper CM. Functions, consequences, and frequency of non-suicidal self-injury. The Psychiatric Quarterly. 2015;86(3):383–393. doi: 10.1007/s11126-015-9338-6. http://dx.doi.org/10.1007/s11126-015-9338-6. [DOI] [PubMed] [Google Scholar]
- Schwarz G. Estimating the dimension of a model. The Annals of Statistics. 1978;6(2):461–464. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP; 2011. [Google Scholar]
- Svirko E, Hawton K. Self-injurious behavior and eating disorders: the extent and nature of the association. Suicide & Life-Threatening Behavior. 2007;37(4):409–421. doi: 10.1521/suli.2007.37.4.409. [DOI] [PubMed] [Google Scholar]
- Swannell SV, Martin GE, Page A, Hasking P, John NJ., St Prevalence of Nonsuicidal Self-Injury in Nonclinical Samples: Systematic Review, Meta-Analysis and Meta-Regression. Suicide and Life-Threatening Behavior. 2014;44(3):273–303. doi: 10.1111/sltb.12070. [DOI] [PubMed] [Google Scholar]
- Turner BJ, Chapman AL, Layden BK. Intrapersonal and interpersonal functions of non suicidal self-injury: associations with emotional and social functioning. Suicide & Life Threatening Behavior. 2012;42(1):36–55. doi: 10.1111/j.1943-278X.2011.00069.x. [DOI] [PubMed] [Google Scholar]
- Weinberg A, Klonsky ED. The effects of self-injury on acute negative arousal: A laboratory simulation. Motivation and Emotion. 2012;36:242–254. http:dx.doi.org/10.1007/s11031-011-9233-x. [Google Scholar]
- Whitlock J, Muehlenkamp J, Purington A, Eckenrode J, Barreira P, Baral Abrams G, Marchell T, Kress V, Girard K, Chin C, Knox K. Nonsuicidal Self-injury in a College Population: General Trends and Sex Differences. Journal of American College Health. 2011;59(8):691–698. doi: 10.1080/07448481.2010.529626. [DOI] [PubMed] [Google Scholar]
- Wilcox HC, Arria AM, Caldeira KM, Vincent KB, Pinchevsky GM, O'Grady KE. Longitudinal predictors of past-year non-suicidal self-injury and motives among college students. Psychological Medicine. 2012;42(4):717–726. doi: 10.1017/S0033291711001814. http:dx.doi.org/10.1017/S0033291711001814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams F, Hasking P. Emotion regulation, coping and alcohol use as moderators in the relationship between self-injury and psychological distress. Prevention Science. 2010;11:33–41. doi: 10.1007/s11121-009-0147-8. http://dx.doi.org/10.1007/s11121-009-0147-8. [DOI] [PubMed] [Google Scholar]